The unpleasant smell of stool and sweat not only causes discomfort in those affected, but also leads to infections of the skin and mucous membranes. Therefore, the cleanliness of the body of the immobilized person should be monitored with special care. Caring for the bedridden person includes the following hygiene measures:
- 'Other stigmata: 10 theses on communicating with people with disabilities
- General advice on care after an amputation
- What complications are possible with an amputation?
- Treatment of pain in amputated limbs
- Aid program COVID-19
- Make a donation
- Read the news
- Stump pain and phantom limb pain have different causes and are not related. The prevalence of phantom pain is up to 75-85 %, that of residual limb pain 60-70 %.
- Rules for turning the patient
- Pay attention to hygiene
- How to deal with phantom pain
- care of the stump
- Complication factors in operations in the elderly
- Anesthesia and its effects on the body of an elderly or senile person
- Suture care after the operation
- Anti-edema therapy for the amputated limb
- Postoperative care of patients after thoracic surgery
- How to choose a nurse to care for a loved one after surgery?
- Treatment
- phantom pain
'Other stigmata: 10 theses on communicating with people with disabilities
The stigma most people write about in connection with HIV is not unique. In addition to people living with the immunodeficiency virus or, for example, LGBT people, countless other groups are also affected by stigma. For example, most people with disabilities.
'Amputees' in English means 'a person with amputated limbs'. The Russian equivalent sounds blunt and somewhat vulgar: 'Amputant'.
According to the US Amputee Coalition, about 2 million people in the United States have been amputated or were born with a different limb. 185,000 are surgically amputated each year.
It's not easy to find two identical stories in the overall statistics: A limb can be removed due to an accident, injury, illness or other health problem.
Self America correspondent Susie Hermitage spoke more than a year ago with Erin Ball, a circus performer who is continuing her career after amputating both her legs. Last summer she organized a week-long camp for adult amputees who wanted to learn circus skills.
Hermitage was so impressed by the encounter with Ball and her fellow amputees that after many conversations and interviews with amputees, she developed a special ten-point list on how to properly communicate with them, what questions about their limbs are inelegant, what language they speak about themselves use it yourself and much more. AIDS.CENTER is releasing a translation of their material from May this year.

1. Do not mix up the experiences of all people with different limbs
Like any group that shares a particular trait, amputees and people with limb differences are not a monolithic whole. For example, the experience of having an arm or leg amputated is different, and people with congenital amputations differ from those who were amputated as adults.
Goldberg, on the other hand, uses the term 'limited ability', even if those around him sometimes correct it. 'Sometimes sane people tell me that the words and phrases I use when talking about myself are inappropriate and that I should use phrases like 'alternatively complex,'' he laments. – he laments. In his opinion, this is a euphemism and condescension.
New Jersey-based human rights activist Ana Chilakos, who had a leg amputated after an accident, says not all people use language that's acceptable to them: 'For example, I say I'm an amputee and they call me ,Disabled people'. It sounds like they need to remind themselves or me that I'm human. I think that's quite clear!'.
Amputees use a wide range of terms to describe their 'stumps', a technical term for the part of an arm or leg that remains after amputation. Chilakos, for example, is comfortable with the word 'blunt'. He plans to have the remaining stump tattooed: 'stump - tree trunk - on the leg stump'.
'When I finally had the surgery, my concern was to get rid of something that wasn't working, something that was getting in my way,' explains Chilakos. – I believe that the stump is not something dead where nothing grows because my member is now more alive than usual. I feel a continuous phantom energy where my leg used to be.
Ball is disgusted by the word 'blunt' applied to her body. She simply refers to her atrophied limbs and prosthetic limbs as 'legs'.
If you don't know which word a person prefers, ask them and follow their lead.
3 If you're going to ask a question, remember that amputees are people, not exhibits
Amputees are often asked questions in public, sometimes in absurd ways. 'I was on the subway once and a woman asked: Do my children have one arm?' – recalls Goldberg.
There's nothing wrong with honestly declaring that you're curious or have never met an amputee,' says Chilakos. She doesn't usually mind questions, even from strangers, as long as people are tactful and communicate with her as a person and not as a 'Google search box'. She's annoyed by questions in a series of stories with big details about what happened, but doesn't mind taking the time to say, 'Yeah, you know, I lost my leg, but It's okay'.
General advice on care after an amputation
Rehabilitation after an amputation includes the postoperative period and the recovery period. In the first days after the operation, special attention is paid to the care of the seams, as well as treating the skin with antiseptic and anti-inflammatory agents.
The second phase is about normalizing blood circulation in the residual limb, maintaining joint mobility and strengthening muscle tissue. For this purpose, a number of rehabilitation and therapy programs aimed at the mental and physical recovery of the patient are used.
Basic principles of care in the postoperative period:
- Checking the cleanliness of the wound – Gently clean the incision site daily.
- reduce swelling. Swelling is a normal condition after an amputation, caused by the stagnation of venous blood and lymph. However, if this symptom does not go away on its own, anti-edema compresses, ointments and other drugs can be used.
- pain relief – The patient may have many types of pain, including phantom pain. Both general and local medications prescribed by the doctor can be used to relieve the syndrome.
- ensure blood circulation – Avoid squeezing the soft tissue around the scar and take care to keep the residual limb in its natural position at rest.
As a rule, recovery from an amputation is free of side effects if all recommendations are followed. That's why it's important to continue following the doctor's recommendations even after you're discharged from the hospital. But even with appropriate care, complications cannot be completely ruled out. This is because the body as a whole is weakened and does not always respond to surgery in a predictable manner.
What complications are possible with an amputation?
After the operation, the patient may experience various problems. Often there is a decrease in immunity, the development of secondary infectious diseases and metabolic disorders. All this can lead to inflammatory processes in the stump. These, in turn, lead to a series of complications that usually only become apparent after discharge from the hospital. The most common include:
- The formation of a keloid-like scar – A red or purple thickening of connective tissue that protrudes from the skin and may enlarge over time.
- muscle cramps – The problem can be treated with physical therapy, massage and a gradual return to lost activity.
- Pelvic Bone and Spinal Displacement – This happens because the patient tries to adapt to the changes in the body and has difficulty properly distributing the load during the movement.
- Joint contractures in the operated extremity – Limitation of range of motion leading to muscle wasting. Resulting from staying in a static position for a long time.
- phantom pain – The feeling that the removed limb is still there and can be itchy and painful.
Older people can experience exacerbation of chronic diseases after amputation.
There are a number of troubling clinical signs. These include fever and reddening of the skin in the wound area. Severe swelling, severe pain, bleeding and an unpleasant odor cannot be overlooked.
Read more:If you experience even one of these symptoms, see your doctor immediately!
Treatment of pain in amputated limbs
Amputees suffer from two types of pain syndromes: residual limb pain and phantom limb pain.
Aid program COVID-19
Make a donation
Read the news
Stump pain and phantom limb pain have different causes and are not related. The prevalence of phantom pain is up to 75-85 %, that of residual limb pain 60-70 %.
A common cause of residual limb pain is neurofibromas, which are nodular growths at the end of the nerve. Surgeons cut them out, but the pain doesn't always go away. If the surgical treatment is unsuccessful, the patient is referred to the pain management clinic. Phantom pain is related to brain activity and treating it is challenging.
Treatment of pain in amputated limbs at Ilya Hospital is:
In Russia, there is no special designation for a pain management specialist. Abroad, the discipline of pain management is called pain treatment. In Ilya Hospital there is a specialist in pain management. Ilinska anesthesiologists work together with surgeons, neurologists, physiotherapists and psychotherapists to treat pain in amputees. This collaboration enables our specialists to make responsible and science-based decisions when examining and treating patients. In their practice, our doctors follow the current international guidelines and choose the best treatment method for each individual case.
We use the latest and safest drugs with proven effectiveness. Patients with residual limb pain are first treated with drugs that alter the levels of neurotransmitters, slowing nerve impulses and blocking the pain sensation in the brain. If this treatment is ineffective, narcotic pain relievers are used.
Rules for turning the patient
The patient's position in bed should be changed every 2 hours to avoid pressure sores. This can also happen at night, being careful not to wake the sleeping person. Observe the following rules when transferring patients in bed:
- When lifting or turning the person onto their side, keep their back straight.
- Always check the skin in the areas where pressure ulcers occur most often: heels and ankles, buttocks, hip area, sacrum, spinous processes, elbows, shoulder blades, occiput and ears.
- The person should not lie sideways directly on a bony prominence - the trochanter of the thigh.
Difficulty with movement may arise if the patient has drain tubes placed or is suffering from chronic pain, so the caregiver advises the person what they will do before any movement.
The maximum time spent in a chair or wheelchair is 1 hour. If the bedridden person is partially able to move independently, every 15 minutes you should remind them to slightly change their posture: lean forward, sidestep, lean on the arms of a chair.
Pay attention to hygiene
The unpleasant smell of stool and sweat is not only unpleasant, but also causes infections of the skin and mucous membranes. Therefore, the cleanliness of the body of the immobile person should be monitored especially carefully. Caring for the bedridden person includes the following hygiene measures:
- intimate hygiene – twice a day, morning and evening;
- washing hands and feet – daily;
- comb hair – daily;
- washing eyes and mouth - daily;
- wash hair – once a week;
- Men's shaving - once or twice a week;
- Whole body washing – once a week;
- Cut nails - as often as the nails grow.
A mild or liquid soap is suitable for hygienic washing. A cloth or towel is moistened with it and the skin rubbed with it. Areas with thin skin or wounds should not be rubbed heavily but should be treated several times a day. After the treatment, all product residues should be completely removed from the body. The skin is then dried with paper towels or a soft towel and a moisturizing or nourishing cream is applied.
If the bedridden patient is partially mobile, they will ask to go to the toilet themselves. It is the nursing staff's job to get the person to the toilet on time. In other cases, a bassinet is used, and diapers are used for incontinence.
How to deal with phantom pain
Phantom pain is an uncomfortable sensation in the removed limb that the patient may have after surgery. If the leg has been amputated up to the thigh, the affected person often still feels itching in the heel, numbness in the fingers or stabbing pain in the knee.
Phantom Pain Syndrome (Ph. (FBS) is very poorly researched and no doctor can pinpoint the exact cause of this pain. However, it has been found that the sensations most often begin to bother the patient who is immobilized for a sufficiently long period of time.
Early physical activity, toughening up, residual limb massage, training with a prosthesis, physical therapy, and wearing a special compression shirt that spreads the load on the residual limb can help reduce FBS.
One cause of phantom limb pain can be improper nerve capping during surgery. In rare cases, this may lead to a second surgical procedure. Doctors usually prescribe drug therapy.
If the pain occurs later after the operation, this may be due to improper care of the residual limb and infection of the residual limb. A poorly fitting or worn prosthesis is also often the cause of severe pain. In such cases, a doctor should be consulted and a prosthesis replacement ordered.
care of the stump
In the first phase after the operation, it is important that the patient learns to take care of the residual limb himself. Preventing infection includes washing the residual limb daily with baby soap, wiping with a stiff towel, and taking contrast showers. To reduce the sensitivity of the skin at the amputation site, it is recommended to rub it with a stiff towel or massage it with a special brush.
Daily inspection of the residual limb for damage or inflammation can help prevent infection from entering the wound and further complications. In rehabilitation after the amputation of a hand or finger, the residual limb inspection can be performed by the patient alone and unaided, or the residual limb can be inspected by someone close to them. If it is not possible to ask for help, the limb can be independently inspected with the help of a mirror.
After fitting the prosthesis, irritation or even a wound may appear on the healed scar. If this is the case, the scar should be cleaned and treated with an antiseptic, and the prosthesis should not be fitted until it has completely healed.
The scar should also be constantly moistened with special, unscented creams. If you sweat profusely, you can also use an antiperspirant.
Complication factors in operations in the elderly
At the top of the list of complications are the patient's chronic diseases. The most serious are those that cannot be corrected Hypertension, atherosclerosis, heart, liver or kidney failure, endocrine disorders. Chronic diseases are often not a categorical contraindication, but require that surgeons, anesthesiologists and medical personnel more closely monitor the patient's condition during the operation and be ready to conduct intensive care if necessary. In addition, new surgical methods – laparoscopy, avoidance of large incisions, surgery with cybernetic knives, etc. – minimize the risks of operating on elderly patients.
- anesthesia and its impact on the elderly;
- Impaired tissue regeneration after surgery;
- difficulties during the rehabilitation period after surgery;
- Changes in emotional state after anesthesia, psychosis and depression.
Anesthesia and its effects on the body of an elderly or senile person
With the current level of development of medicine in general, surgery and anesthesiology in particular, the concept of severe, traumatic and life-shortening anesthesia is completely a thing of the past. The variety of anesthetic techniques and drugs makes it possible to operate on patients of all ages. For example, in patients with cardiac insufficiency, general anesthesia can be replaced by general anesthesia for epidural anesthesia, where the patient does not feel the area being numbed but is conscious during the procedure.
In the elderly and old people, it is necessary to correctly and accurately calculate the dose with which the drugs are put into anesthetic sleep. At this point, the risks associated with anesthesia end. However, older patients tend to be overly emotional about the preparation for surgery and the procedure itself. This emotionality manifests itself in the fear of death, the fear of complications during the operation, and the fear that the anesthesia, while sufficient to sedate the patient, is not sufficient to completely relieve the pain. In other words, the patient fears that although they are in pain, they are unable to report it. Such fears are unfounded. Those close to the patient should do their best to calm them down and put them in a positive mood.
Suture care after the operation
The postoperative suture must be monitored by the doctor and nursing staff. The patient must follow the doctor's instructions. This is especially true for patients who have been diagnosed with diabetes and vascular diseases, since the likelihood of infection in this category is increased.
The skin on the residual limb is extremely sensitive after the operation. To reduce hypersensitivity, a soft brush or massage ball can be used to gently massage the residual limb. Rubbing the residual limb with a stiff towel or terrycloth flannel is also an effective method. This massage involves moving from the outermost part of the residual limb to its base.
Skin care on the residual limb requires hygiene. The residual limb should be showered with contrast, washed with mild soap and dried with a soft towel. The skin on the stump should be inspected daily to observe any changes. If they occur, the doctor should be informed immediately. The stump is viewed with a small hand mirror.
It usually takes 2 to 3 weeks for the surgical wound to heal; after that, a scar remains, which must be regularly moistened. It should be rubbed daily with an odorless cream.
Patients with diabetes or circulatory problems require longer treatment. These patients are more likely to become infected at the surgical site. These patients sometimes develop dermatological complications. It is appropriate for them to use special drugs during care.
Anti-edema therapy for the amputated limb
A serious problem to solve is the edema that occurs as a result of the operation. It is a consequence of the surgical procedure. It usually goes away within 2 weeks.
The wound should be loosely bandaged until the sutures are removed. Initially, no pressure should be exerted on the residual limb. To reduce swelling, the residual limb should be positioned over the heart for the first few postoperative days. A compression treatment is then performed to reduce the edema and prepare the residual limb for the insertion of the prosthesis. This improves blood circulation in the residual limb, reduces pain and accelerates the healing process.
To reduce edema, it is best to use a special elastic bandage, a compression cord, a silicone sleeve, and lymphatic drainage by a specialist. First of all, all this is carried out by medical personnel who are trained for the patient's family and the patient himself. Then these measures are carried out by the patient himself.
The bandage should be neither too loose nor too tight. The residual limb should be bandaged in the morning after the patient wakes up. The bandage should be removed before bedtime. It is important that the distal portion of the residual limb is subjected to maximum pressure but not painful. The higher the bandage is applied, the less pressure is exerted.
If the leg was amputated above the knee, it is advisable to lie face down for half an hour twice a day. The head should be on the side opposite the amputation. This makes it easier to stretch the muscles of the residual limb.
In order to assess the success of the anti-edema treatment, the diameter of the residual limb is measured at the same points in the morning and in the evening. It is advisable to log these measurements.
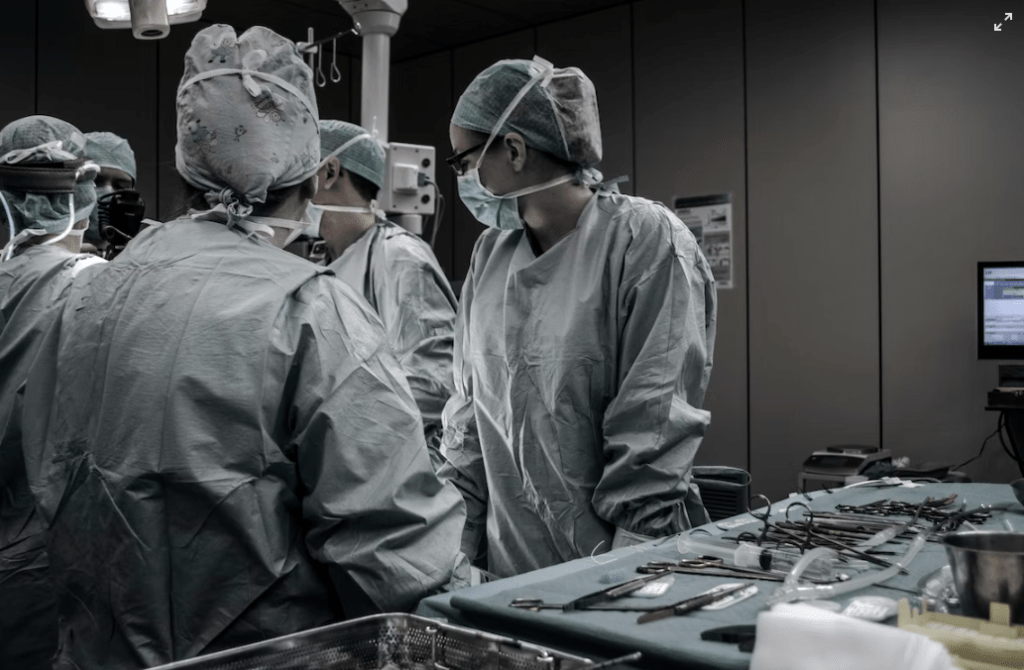
Postoperative care of patients after thoracic surgery
During the postoperative period after thoracic surgery, the nursing staff should monitor the patient's condition and the condition of the drains. Care should be taken to monitor the nature of the draining fluid and to ensure that the drain does not accidentally detach from the aspirator and leak out of the wound. Inhalation of sputum thinning agents is recommended to improve bronchial patency.
When caring for a patient after thoracic surgery, the nursing staff should administer cardiac, analgesic, and antimicrobial medications as prescribed by the physician.
Severe pain in the chest area makes it difficult for the patient to breathe, which leads to reduced ventilation of the lungs and the development of oxygen starvation. Limited mobility, especially in older patients, can also lead to congestion in the lungs, obstructing sputum production and contributing to the development of pneumonia. In order to improve sputum drainage and prevent constipation, nurses help patients to change their body position regularly.
We have previously published an article on the care of patients with respiratory diseases. You can read it on this page.
How to choose a nurse to care for a loved one after surgery?
A good nurse should not only be an experienced professional, but also have positive personal qualities. To choose the right nurse for your patient after surgery, go to 'Our Staff'. There you can read a description of each employee, see a photo of them and get to know them better:
You can choose any caregiver for your loved one. To do this, call us and tell us the name of the person you would like to hire. If it is available, we will send it to your home or hospital as soon as possible.
If for any reason you don't like the caregiver, we will replace her at no additional cost. The number of representatives is not limited.
You can take out your contract with Carer 24 at the office or at home. In the latter case we will send a courier with the nursing services. He will come to the address you specified with the necessary documents. All you have to do is sign the appropriate places and our nurse can start work.
Why Nurse 24
Caring for patients after surgery is a demanding task. Your loved one's recovery directly depends on the choice of caregiver. If you want to surround him or her with care, choose Nurse 24. We have:
- Experienced staff. Each nurse has impressive experience of working with different patients. We only select a responsible, careful, kind and calm nurse with whom the patient feels comfortable.
- affordable prices. We are chosen by customers from all over Moscow. Also, unlike other companies, we don't charge for recruitment. Check the aftercare price list under the 'Prices' tab.
- Regular special offers. We often do special offers and discounts for our customers to save money. Current special offers can be found on our homepage.
- Satisfied costumers. By studying user comments, you can choose the right tutor for you. Reviews about our company – on the website.
- Wide range of services. The supervisor does not only take care of the patient after the operation. She can do wet and dry cleaning in the room, go to the pharmacy, accompany the patient to the clinic, cook him a meal and much more. See the Pricing section for a list of additional services and their prices.
Treatment
pain in the stump. The cause of residual limb pain is usually an ill-fitting prosthesis. A correctly fitted prosthesis can therefore eliminate most symptoms.
If the patient has a trigger point caused by the formation of a neuroma, injections of local anesthetic into that point may be necessary.
Surgery is only done if the wound needs to heal. Repeated, more proximal amputations are not indicated for pain management.
phantom pain
A promising new approach to treating phantom limb pain is mirror therapy, which uses a special mirror box. It is known that motor response changes when sensory impulses are not transmitted to the somatosensory cortex.
It is assumed that the motor system requires sensory impulses from the periphery in order to carry out movements in the limbs. In the absence of impulses, the motor system perceives the absent limb as paralyzed, and contractures occur.
The pain may be preceded by a constant feeling of stiffness.
The principle of mirror therapy The principle of mirror therapy is to trigger sensory impulses from the missing limb to relieve pain.
A mirror is held in front of the healthy limb and when the patient moves it, he perceives these movements as movements of the missing limb.
This is how the sensory impulses get to the brain. Studies have shown that this type of treatment reduces symptoms.
However, it is not known whether this is due to the mirror training itself or to the ideomotor training.
Various medications are used to treat phantom limb pain.
So far, clinical trials have not shown any advantage of one drug over another. Phantom pain is believed to be neuropathic in nature. It is common to prescribe Antidepressants and anticonvulsants..
In the case of very severe pain, the administration of opioids. There is evidence that percutaneous electronic neurostimulation of the residual limb relieves phantom limb pain.
The procedure is safe, which is an additional advantage.
A major limitation of this type of treatment is the need for electrode space and the need for prostheses.
Phantom pain is also treated with SCM and sympathetic blocks can also be used to treat phantom limb pain..



- The reamputation is.
- Limb amputation.
- blunt.
- Life after a leg amputation.
- acetabulum.
- The toe formation.
- prosthetic legs.
- Indications for amputation.