Treatment of congenital clubfoot in infants begins on the 7th to 10th day after birth. Only the mildest cases can be treated with flannel bandages, corrective exercises and massage. As a rule, plaster casts are used, which are changed for the first time after 7 days and after 3 to 5 months of treatment, if the foot is in a moderate position, after 9 to 12 days. When applying the cast, the child is placed on his stomach and the leg is bent at the knee joint, which brings the attachment points of the calf muscles closer together (Fig. 1). Some orthopedists put a cast on the foot and lower leg, others on the knee joint and the lower third of the thigh. By the age of 6-7 months, and sometimes by the time walking begins, the deformity can be completely eliminated in most patients. After treatment, the child must be fitted with a plaster splint, which in mild cases of C. should only be worn at night. If there is a risk of recurrence, the child must wear them all the time. Special exercises to correct the deformity and strengthen the muscles of the lower limbs should be included in the treatment (Fig. 1). Vilensky suggested placing a wedge-shaped foam pad on the back surface of the foot when applying the cast. Removing this pad allows corrective active and passive exercises for the foot. To keep the foot in the correct position, the shapers are made of thermoplastic material (polycarbonate), monolithic polyethylene, etc.

- How to correct a clubfoot?
- Possible causes
- Non-idiopathic clubfoot
- Treatment
- What is clubfoot?
- Popular
- What is a flat foot?
- Causes of flat feet
- Clubfoot in children
- Clubfoot in adults
- Congenital clubfoot in children. Treatment
- Symptoms of clubfoot in a newborn:
- symptoms
- Symptoms of acquired clubfoot in children
- Symptoms of clubfoot in adults
- complications
- overview
- Treatment of clubfoot
- The Ponseti method for treating clubfoot without surgery
- Surgery for clubfoot
- Splint for clubfoot in children
- Acquired clubfoot
- OSTEOPATHY AND TREATMENT OF CLUB FOOT
- PREVENTION OF CLUBFOOT
How to correct a clubfoot?
We have known the poem about clubfoot since childhood. But the clubfoot problem can occur not only in Bear, but also in Teddy Bear, Seryoshka, Aneka, Taneka and other children, regardless of their name. In this blog article we will try to understand what clubfoot is, how to recognize it and how to correct it.
The term refers to a deformity of the foot when it deviates inward from the axis of the lower limbs. To put it simply, they are turned inward from the foot, although they are usually a straight extension of the foot.
Possible causes
Experts differentiate between congenital and acquired clubfoot. The former can be detected using ultrasound during pregnancy. Its causes are still unknown. The cause could be physiology, e.g. B. a narrow uterus that presses on the child, lack of water or a breech position. There is also evidence that severe stress or the consumption of alcohol or drugs during pregnancy can influence the development of the disease. However, the anomaly can also occur at a genetic level.
The disease can also occur after birth. Causes include fractures and irregular bone fusions, stunted growth, burns, and tumors. To be fair, these cases are much rarer than congenital cases.
Depending on the complexity, the condition is divided into three stages. In the first stage it is often corrected manually, while in the third stage the mobility of the joints is already limited and treatment with conservative methods is not advisable.
Non-idiopathic clubfoot
Non-idiopathic clubfoot does not occur alone and is caused by other malformations and/or diseases.
In the terminology of pediatric orthopedists who treat clubfoot, it is a complex form that includes:
- Neurogenic (related to neurological diseases);
- Syndromic (according to statistics, there are more than 115 syndromes that include a combination of clubfoot and mental retardation);
- Teratogenic (impairment of embryonic development under the influence of teratogenic factors - certain physical, chemical (including drugs) and biological agents (e.g. viruses) with morphological abnormalities and malformations);
- Previous treatments (an improperly applied cast can lead to secondary deformities);
- In older children.
In typical idiopathic clubfoot there is a local problem with foot deformity and there is the Ponseti method which helps in most cases.
In non-idiopathic clubfoot, there is a local problem of foot deformity and a general health problem of the child. An individual approach is taken to treat complex clubfoot.
During the examination, the specialists pay attention to the clinical features:
Radiologically, the deformity is confirmed by:
- abnormal ossification of the ossification nuclei;
- unusual combination of angular parameters;
- Narrowing of the joint spaces;
- Atypicality of the deformity.
The pediatric orthopedist will be able to answer this question during the direct examination.
Any treatment for complex non-idiopathic clubfoot begins with a Ponseti cast. In most cases, the number of casts statistically increases twofold compared to standard Ponseti treatment. Depending on the initial diagnosis, a surgical option is suggested in the surgical phase. The goal of the pediatric orthopedic surgeon is to return the foot to a state where it is supportive, functional, and capable of learning.
Treatment
The severity of the disease varies and determines the type of therapeutic measures. In all cases the child wears orthopedic shoes.
The movement of the ankle joint is not restricted and the elements of the foot can be corrected. The specific massages for congenital clubfoot take into account the child's elastic bone tissue in order to achieve the correct position. Reduction exercises and soft tissue bandages help.
The feet cannot be adjusted with the hands, are springy and a hindrance is felt. Freedom of movement in the ankle joint is slightly restricted. Here an effects complex is prepared for the light scene. Plaster casts are then made with further corrections of supination, toes, heel elevation and other elements.
The bones and joints are significantly deformed, and the peculiarities of massage for congenital clubfoot and manual correction methods do not allow the position to be normalized at this stage. Surgical intervention is indicated.
The Progress Medicine Circle Center specializes in comprehensive care and rehabilitation for children with orthopedic problems.
What is clubfoot?




We guarantee that your personal information will not be shared and that no commercial communications will be sent to the phone number provided. Providing your details is necessary to provide you with feedback and to arrange an appointment with a specialist at the clinic.
- About Us
- Our doctors
- Pediatric Dentistry
- QUESTIONS AND ANSWERS
- reviews
- Prices
- Images and videos
- partner
- Contact
Popular
The material on this website is provided for informational purposes and is intended for educational purposes. It should not be relied upon as medical advice by visitors to this website. The determination of the diagnosis and the choice of treatment rests solely with the doctor! 'The Clinic of Pediatrics and Pediatric Surgery is not liable for any possible negative consequences resulting from the use of the information provided on pedclin.ru
THERE ARE CONTRAINDICATIONS. PLEASE CONSULT A SPECIALIST.
Professional Medical Center Ltd.
What is a flat foot?
Flat feet in children and adults – a pathology in which the shape of the arch of the foot changes. It occurs for various reasons and is accompanied by functional disorders. There are several types: transverse, longitudinal and combined.
Transverse arch occurs in most adult patients. It is characterized by divergence of the metatarsals and deformation of the big toe, forming 'ankle'.
Longitudinal flatfoot is characteristic of adolescents and children. The patient has a flattened longitudinal arch of the foot, resulting in an elongated and flattened foot. There is a combined variant in which the two aforementioned forms occur together.
Causes of flat feet
Flat feet can be congenital or acquired. The congenital variant is diagnosed in childhood and is associated with the features of the formation of the ligamentous apparatus of the feet.
Congenital flatfoot is characteristic of people with weak ligaments in the feet and lower legs. Due to this hereditary predisposition, a person gradually develops flat feet. The risk factors for the development of pathology include.
● high body weight;
lack of exercise and sedentary work;
Working while standing, e.g. E.g. assembly line workers, hairdressers, etc.;
● Foot injuries with bone fractures.
A patient may have multiple risk factors present at the same time. Eliminating them is essential for a full recovery. In our clinic, an orthopedist and trauma surgeon always carries out a comprehensive examination to determine all causes.
Clubfoot in children
The first signs of a congenital clubfoot can be seen at birth: the foot is in an unnatural position and hangs with the outer edge downwards. Congenital clubfoot is characterized by the fact that in the first year of life the child walks with the sole turned inwards and rests on the outside of the foot.
Without treatment, the disease progresses and can lead to pronounced muscle wasting in the lower leg by the age of 3-5 years. Your child will have an irregular gait and difficulty walking and running. The leg becomes shorter.
During an examination in the clinic of Dr. The doctors determine the severity of Anna's illness. This determines the treatment approach and the prognosis for healing.
Clubfoot in adults
Clubfoot in adults has similar symptoms to those in children. The main symptom is the inability to fully place the foot on a surface. The foot is turned to one side and part of the heel always remains raised.
Congenital clubfoot in children. Treatment

Clubfoot in children is a congenital bone and foot abnormality that occurs before birth. It can be diagnosed in the expectant mother by ultrasound in the 8th to 12th week of pregnancy. Congenital clubfoot can be effectively treated immediately after birth, otherwise it can lead to disability. It can also be a manifestation of other illnesses, such as: B. spina bifida in the lumbar spine, and can be combined with hip dysplasia.
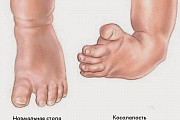
Symptoms of clubfoot in a newborn:
- The foot is smaller and the heel is significantly smaller than in a healthy foot;
- The forefoot is directed downwards;
- The plantar surface of the clubfoot faces the other foot;
- The foot is turned outwards (supinated), with the sole pointing downwards.
A newborn with congenital clubfoot should be evaluated by an orthopedic surgeon. There are conservative and surgical methods to treat clubfoot in children.
For conservative treatment, the podiatrist prescribes an orthopedist:
If the foot deformity is severe or the parents go to the doctor too late, surgery is performed. It should be noted that the operation is carried out when the child is six months old. With the Ponzetti method, surgical treatment is used earlier.
symptoms
The symptoms of clubfoot in newborns are as follows. At birth, clubfoot is suspected due to the following symptoms: the child's foot is smaller than its age, the outer edge of the foot is directed downward and the inner toe is elevated (equinus), the big toe or all of the toes are inward rotated, the toe is pointed downward and the heel is elevated. There is a deep longitudinal groove in the foot and a bulge on the inside of the foot.
A complete inversion of the foot (adduction), an outward twisting of the ankle joints, support only on the outside of the foot (varus) and a lack of full mobility of the ankle joint are also observed. It is important to differentiate between congenital clubfoot and spastic paralysis. In congenital clubfoot, muscle tone is unchanged, while in childhood spastic paralysis there is pronounced muscle hypertonicity.

Symptoms of acquired clubfoot in children
The development of the musculoskeletal system continues after birth. That's why it's so important that parents pay attention to their child. Acquired clubfoot in a child under 3 years old manifests itself as follows:
- Misalignment of one or both feet. This is easy to see if the child is walking on wet sand or snow.
- Change in gait.
- A restriction of mobility in the ankle joint occurs.
- Changes in the position of the knees.
- The big toe is tilted towards the inside.
Symptoms of clubfoot in adults
The main symptom is the inability to fully place the foot on a flat surface. The person supports himself on the outside of the foot, the heel is raised and the foot is turned inwards. In adults, the characteristic 'Winnie the Pooh' pattern appears: flattening of the lumbar spine, bulging of the thoracic spine and a rounded shape of the back. A typical somersault gait develops.
complications
Complications in children are manifested by the following pathologies:
- Frequent injuries to the foot and ankle joints.
- Impairment of the function of the knee joints.
- Thickening of the skin on the outside of the foot.
- Atrophy of the foot muscles.
- Scoliosis and other spinal deformities.
- Psychological problems – the child becomes withdrawn and has difficulty communicating with peers.
Clubfoot in adulthood is complicated by a number of serious diseases: pronounced deformation of the chest leading to reduced lung capacity, obstruction of venous outflow from the lower limbs with the development of venous insufficiency, arthritis of the ankles and knees, venous thrombosis. There are nutritional disorders of the skin of the feet and lower extremities with the formation of trophic ulcers, displacement of abdominal and pelvic organs due to spinal deformities.
overview
Clubfoot is a congenital deformity of the foot and/or ankle. With early intervention, its position and function can be largely corrected.

In clubfoot, the infant's foot is twisted downward and inward. Although this does not cause discomfort, if left untreated it will prevent normal walking and cause pain as the child grows older. Clubfoot is relatively common. About half of all cases are bilateral clubfoot.
The cause of clubfoot is unclear in most cases, but sometimes genetic changes that are inherited cause deformities of the feet and other joints in the legs. If a child in a family is born with clubfoot, there is a 1 in 35 chance that the other child will also have it. If a parent had clubfoot as a child, there is a 1 in 30 chance that the child will also have clubfoot. If both parents had clubfoot, the chance increases to about 1 in 3. Less commonly, the cause of clubfoot is certain serious diseases that affect the child's development, such as: B. Spina bifida – incomplete closure of the spinal canal.
Clubfoot is usually diagnosed shortly after birth, but is sometimes detected during an ultrasound scan between weeks 18 and 21. It is not possible to start treatment before birth, but early diagnosis gives doctors time to Discuss the illness in detail and plan the next steps after the baby is born. Additional tests for other diseases and malformations may be necessary during pregnancy.
Treatment of clubfoot
Treatment is best started in the first week or two after birth, but can be done later. There are now both non-surgical methods of treating clubfoot and methods of surgically correcting the shape of the foot.
The Ponseti method for treating clubfoot without surgery
The Ponseti method is the most important method for treating clubfoot because it is more effective and efficient compared to surgery.
With this method, the orthopedist slightly corrects the position of the child's foot with his hand once a week. The foot is fixed in this position with a plaster cast. After a week, the procedure is repeated and the doctor corrects the position of the foot a little more. The cast is changed once a week, and each time the position of the foot is brought a little closer to normal. Typically 5-6 bandages are required, sometimes a little more or less depending on the severity of the clubfoot.
The procedure is painless and the doctor proceeds very carefully. Children often cry during the procedure, but usually not because they are in pain.
Surgery for clubfoot
If the Ponseti method has not completely corrected the alignment of the foot, the doctor may recommend minor surgery to cut the Achilles tendon (above the heel). This is the case when the forefoot has already been trained, but the ankle is not yet in the correct position.
The operation is performed under local anesthesia on an outpatient basis, meaning no overnight stay in the hospital is required. In some cases, doctors may recommend general anesthesia. In this case, the child sleeps during the operation. The surgeon makes a small incision in the Achilles tendon to allow the foot to assume its natural position. The child's foot is then placed in a cast for three weeks. In rare cases, the tendon at the front of the ankle may need to be operated on again after a few years to help the leg function better.
Splint for clubfoot in children
After treatment, the child must wear an orthosis - a splint to which a shoe is attached. You fix your feet in a slightly outward position at shoulder width. This is done to consolidate the treatment and prevent clubfoot from recurring.
Acquired clubfoot
Paralytic clubfoot occurs after polio, when the peroneal muscles are paralyzed and the supinating muscles of the foot are functional, or after an isolated injury to the peroneal nerve. The treatment principles for these forms of clubfoot are identical. It begins with the elimination of the C. by gradual plaster casts, and if the integrity of the ankle nerve is compromised, it is sutured; if the nerve cannot be sutured, tendons of healthy muscles are transplanted from the inner edge of the foot to the outer edge.
When pes varus is paralyzed but dorsiflexion is active, arthrodesis can be performed at three joints: the talocrural, talo-femoral, and calcaneocuboid joints. For pes equinovarus paralyticus, a Z-shaped extension of the heel tendon should be performed in the sagittal plane, severing the medial portion of the tendon below, simultaneously with supination of the tendon transposition on the outer edge of the foot.
C. It also occurs after inadequately treated fractures of the talus or several bones of the foot, as well as after fractures of the talus with subluxation of the foot at the ankle or talus-foot joint. Treatment consists of surgical repositioning and wedge resection of the foot and tibia bones and arthrodesis.
C. can be caused by various inflammatory processes of the ankle joint. C. Scar formation after deep burns, inflammatory processes or excision of the scar with subsequent plasticity with a phyllar stem, or bone surgery is performed. C. may occur after ischemic necrosis of the lower leg muscles.
References: Bohm GS Clinical forms of congenital clubfoot, Orthop. and Traumatology, Vol. 5, p. 55, 1937, bibliography;
Vreden RR Practical Guide to Orthopedics, p. 156, L., 1936; Zatsepin TS Congenital Clubfoot and its treatment in childhood, M., 1947, bibliography; Movshovich IA and Vilensky VY Polymers in traumatology and orthopedics, pp. 279, M., 1978; Moroz PF Surgical treatment of congenital clubfoot in children, Kishinev, 1976, bibliography; Osten-Sacken E. Yu. Amniotic forms of Clubfoot, Orthop. and Traumat., vol. 1-2, p. 29, 1929, bibliography; Early conservative treatment of Congenital Clubfoot with products of polymeric materials, by. VJ Vilensky et al, M., 1973; Campbell WC Operative Orthopedics, St Louis, 1949; Henkel HL The treatment of congenital clubfoot in infants and children, Stuttgart, 1974.
OSTEOPATHY AND TREATMENT OF CLUB FOOT
If you notice signs of clubfoot in your newborn, it is advisable to take your baby to an osteopath as soon as possible after discharge from the hospital or, if there is such a person in the maternity hospital, to see an osteopath.
The earlier a correction is made, the faster progress will be made.
Osteopathy is so effective in treating club feet and other conditions caused by birth trauma that positive results can be achieved after just two or three sessions. Infants have very flexible and supple ligaments and are very easy to treat.
However, it is worth remembering that the treatment process is lengthy and one should not stop halfway. Treatment should be completed when the foot is in a stable and normal position.
When you see an osteopath, an experienced therapist will help your child move the bones into the correct position and correct changes that have not yet caused clinical symptoms.
In the case of club feet, the osteopath uncovers the cause of the disease and applies manual techniques that are individually tailored to each case.
PREVENTION OF CLUBFOOT
Prevention is better than cure. Clubfoot is no exception to this rule.
During pregnancy, you should lead a normal lifestyle, take care of your health and the condition of the baby, eat healthy, regularly visit the gynecologist and undergo all examinations, visit an osteopath three times during pregnancy, starting from 12 weeks, in order to promote the baby's harmonious development and prepare the body for birth.
After giving birth, doctors recommend following certain rules to prevent the appearance of clubfoot:
- Pay attention to your baby's footprints in the wet sand.
- Pay attention to your child's gait.
- Make sure your child gets regular exercise.
- Make sure swimming is part of your 'exercise routine'.
- If your child is overweight, adjust the diet and bring the weight down to the age limit.
- Your child's diet should be nutritious and varied.
- It is important that your child has comfortable, good quality shoes with a good insole and a stiff back.
If your child has the prerequisites for developing clubfoot (infections, a history of rickets, heredity) or had a clubfoot at birth but has healed, a visit to an osteopath at least every six months is essential to prevent primary or recurrent clubfoot. This ensures that your child is healthy and has a happy, flying gait for life.
Dear parents, if you still have any questions, we are happy to help you! You can ask us your questions in the form below and we will answer them for you!
Read more:- Congenital clubfoot.
- 1 year old child with clubfoot.
- The Ponseti method.
- clubfoot.
- Clubfoot in 7-year-old children.
- Why does a child develop clubfoot?.
- Ponseti breeches.
- Clubfoot Treatment.