Another cause of tiptoe walking is severe neck tension. In this case, this gait may be an adaptive function of the body: the body protects the injured neck by tensing the muscles under the back of the head. The contraction affects the entire posterior muscle chain and runs from the neck through the cervical spine to the thoracic and lumbar spine without affecting the calf muscles. It is as if the body redistributes the voltage away from the original source.

- Idiopathic toe walking and a heterozygous mutation in the NDGR1 gene: two clinical cases.
- To quote:
- general characteristics
- classification
- Treatment
- How does this disease come about?
- What does that mean?
- How to stop your child from tiptoeing
- Exercises to help children stop walking on their toes
- characteristics
- Physical therapy
- Isometric exercises
- Isotonic exercises
- When is it normal?
- What to do if your child walks on tiptoes?
- The answer to the most important question: Is it worth the pain?
- When is toe walking normal?
- How do you know that walking on tiptoes is not normal?
- Why does my child tiptoe? The main causes
- Up to the age of 3 years
- Purchasing age-appropriate orthopedic shoes
- Your child likes to do this
- Your child moves frequently on the walker
- Emotional shock or personality traits
- Chaplin's gait
- clubfoot
- Child development: Does the gait need to be corrected?
- How to help your child: advice for parents
Idiopathic toe walking and a heterozygous mutation in the NDGR1 gene: two clinical cases.
1) Ruzbarsky JJ, Scher D., Dodwell E. Toe walking: causes, epidemiology, assessment and treatment // Curr Opin Pediatr. 2016; 28(1): 40-46. DOI: 10.1097/MOP.0000000000000302.
2) Pomarino D., Ramírez Lamas J., Martin S., Pomarino A. A review of the literature on idiopathic toe walking: Etiology, Prevalence, Classification, and Treatment // Foot Ankle Spec. 2017; 10(4):337-342. DOI: 10.1177/1938640016687370.
3 Pomarino D., Thren A., Morigeau S., Thren J. Genetic causes of toe walking in children // Genetics and Molecular Biology Research. 2018; 2(9): 1-5.
4 Kalaydjieva L, Gresham D, Gooding R, Heather L, Baas F, de Jonge R, Blechschmidt K, Angelicheva D, Chandler D, Worsley P, Rosenthal A, King RH, Thomas PK N-myc downstream-regulated gene 1 is mutated in hereditary motor and sensory neuropathy-Lom // Am J Hum Genet. 2000; 67(1): 47-58. DOI: 10.1086/302978.
5. NLM, 2019 Clinvar. [Online] Available at: https://www.ncbi.nlm.nih.gov/clinvar/variation/639524/ [Accessed June 28, 2020].
To quote:
Pomarino D, Tren JR, Emelina AA. Idiopathic toe walking and heterozygous mutation in the NDGR1 gene: 2 clinical cases. Lechashi Vrach. 2021;(6):7-8. (In Russian.) https://doi.org/10.51793/OS.2021.24.6.001
general characteristics
Gait is a complex motor act that requires the coordinated work of central brain structures, pathways, peripheral nerves, body muscles and limbs. The involvement of different levels of neuronal structures leads to a variety of etiological factors in gait disorders. Many neurological and some orthopedic diseases are accompanied by the development of typical gait changes. The assessment of the pathological gait is an important part of the initial diagnosis.
The prevalence of gait disorders increases with age. This symptom is rare in children and adolescents; most cases are associated with trauma, infections and purulent processes. After the age of 40, the number of those affected begins to increase, primarily due to strokes. In the age group of 60 to 69 years the prevalence is 15 %, in the age group over 70 years it is 35 % and in the age group over 80 years it is 60 %, which is related to the development of degenerative pathologies and an increasing proportion of complex diseases .
classification
There are more than 20 different types of gait disorders. The classification is based on the causes of development and the external symptoms. The most important variants are:
- Shaky (ataxic) gait. It arises from cerebellar and thalamic involvement. Due to the imbalance, the patient staggers and spreads his legs wide. Staggering is noted both when walking and when standing.
- Tumbling. Reflects a decrease in depth sensation when the pathways (more commonly the dorsal horns of the spinal cord) are damaged. The feet are 'pushed' into the ground with effort, pressing all soles simultaneously, and walking is visually controlled.
- Jerking. Occurs in old age, some neurological disorders and general weakness. The stride length is shortened and the soles of the feet are not or only slightly lifted off the ground.
- Articulated foot (stepping). Observed in damage to the ankle nerves and a number of other pathologies. When lifting the hanging foot, the affected person bends the knee sharply so that the tip of the foot does not touch the ground and throws the leg forward.
- 'Duckfoot'. Occurs in patients with paresis or mechanical damage to the adductors of the thigh. With bilateral gait abnormalities, the patient tilts from side to side, while with unilateral damage, the pelvis tilts toward the moving leg.
- Paretic. Detected in muscle paresis of the lower limbs. The type of lesions is determined by the involvement of different muscle groups.
- Hemiparetic. Characteristic of hemiparesis of various etiologies. The painful arm is pressed against the body, the painful leg is not bent and moves in a semicircle, the body tilts to the healthy side.
In addition to these gait disorders, a distinction is also made between freezing when walking (release disbiosis) and propulsion - irresistible acceleration when walking or after a light shock. These two disorders are observed in patients with Parkinsonism. Frising's disbiosis sometimes occurs after multiple strokes or in elderly patients without signs of neurological disease.
Treatment
The treatment is individual. Surgery (surgical repair of the Achilles tendon) is rarely necessary; Treatment is usually conservative. It consists of wearing special orthoses and physiotherapy and lasts between 6 and 24 months. If there is no improvement, plaster casts and orthoses are used (sometimes in combination with botulinum toxin injections). Special footwear (hard ankle shoes and hard soles) is effective for temporary walking.
Since ICH syndrome has no specific etiology, there are no preventive measures. Wearing well-fitting shoes and frequent barefoot walking may be recommended. Early diagnosis and treatment can help prevent further complications.
How does this disease come about?
Scientists suspect that one of the reasons for the economical gait of humans lies in the structure of the foot, which is unusual for mammals: a large heel bone, a powerful and strong big toe, which is parallel to the index toe.

'These features are characteristic of great apes and form the mechanical basis for energy-efficient walking. However, humans use more energy when running than most other mammals. We are well adapted to running long distances, but human sprinting ability is less than that of many animals. This is due to an energy-inefficient running style, explains the study's leader, biology professor David Carrier.
What does that mean?
The results of the study by American and German scientists should help doctors, especially with back pain. But the findings of this experiment also have practical applications. It turns out that walking on tiptoes helps burn calories faster and also strengthens the ankles, back, knees and hips.
Of course, the usual way of walking should not be completely abandoned. However, walking on your toes for five minutes every day helps strengthen the muscles involved in walking while burning off extra calories and getting closer to your desired figure.
How to stop your child from tiptoeing
What to do if a child walks on tiptoes? Orthopedist Anton Kustikov wants to know whether it is possible to stop a child from walking on tiptoes:
'From a medical perspective, the answer is more likely to be 'no' than 'yes'. For many children, this running mechanic is part of the process of learning about the world and acquiring 'adult' skills. Therefore, no special weaning technique has been medically developed to date. The only thing to do is to wait until the habit no longer bores the child. However, if the process drags on, it is better to see a doctor.

At the same time, the doctor emphasizes that it is important not to wean the child, but not to miss the moment when toe-walking develops from a 'game' into a permanent habit:
'Otherwise, this gait may still be present in the child even after the age of five. The calf muscles are permanently contracted and treatment and prevention can take several years. Preventive measures are helpful: massages, exercise therapy and physiotherapeutic treatments.
Comfortable shoes have also proven to be a good preventive measure.
For example, many children often walk barefoot on their toes, but in sneakers or sandals with insoles they begin to rely on the whole foot.
Exercises to help children stop walking on their toes
According to Igor Novokrinitsky, a specialist in early motor development and author of the 'Baby Fitness' course, up to the age of one and a half or two years, a child can alternately walk on tiptoes and with the whole foot, which may be a variant of the norm .
Are there any special exercises that will help stop a child from toe walking? Before answering this question, the expert warns: 'I would recommend first introducing the child to a neurologist and an orthopedist to determine the causes of these 'tiptoes'.
Igor Novokrinitsky explains that foot exercises help the child's heel sink to the floor:
'In summer you should walk barefoot more often on the ground, sand, grass and stones.
On the flat, I recommend running on orthopedic mats, the most important thing is to make the ground as varied as possible. In addition to normal walking, I recommend rolling from heel to heel on the orthopedic mats. A foot massage with a piercing rubber ball (6 cm diameter) is also effective. And everyone probably has a mop at home. If it has a round handle, try letting your child walk on this mop a few times a day.
characteristics
- The generation of maximum muscle force is directly related to the number of muscle fibers involved in the movement and the cross-sectional area of the muscle.
- The arrangement of the fibers depending on the angle of their attachment to the tendon, the length of the muscle, the extent of joint flexion and the speed of contraction can change the expression of muscle strength.
- The magnitude of the force also depends on the degree of activation of the motor unit (according to the magnitude principle).
Adaptation to resistance training allows for the production of greater force through multiple neuromuscular mechanisms. Muscle strength can increase significantly in the first week after beginning training (improved control by the nervous system), and long-term strength gains are achieved through improved changes in muscle architecture, increased muscle cross-sectional area, and adaptation to increased metabolic processes.
You can read about chronic ankle instability here and syndesmotic sprains here.
The speed of strength gains depends on the type of program and careful implementation of the recommendations regarding intensity, selection and sequence of exercises, volume, frequency and length of rest periods between sets.
Physical therapy
Once the desired range of motion is achieved and the swelling and pain intensity have decreased, the patient can move on to the next phase of rehabilitation: strengthening exercises. Strengthening the weakened muscles is essential for a rapid recovery of the ankle. It is also a preventative measure against re-injury. Rehabilitation should focus on all muscles of the ankle, including the calf muscles.
Bilateral exercises are considered important to prevent damage to the ankle ligaments.
Continuous monitoring of strength is important. Isokinetic strength testing is a common method for assessing the ankle joint. A hand dynamometer can also be used.
It is important to understand that the rehabilitation program must be individualized. Mental training during treatment can be a useful addition to standard measures that focus on increasing muscle strength.
Increasing strength begins with isometric exercises and progresses to dynamic resistance exercises.
Isometric exercises
Resistance is provided by a stationary object (wall or floor), a contralateral foot, or resistance from a physical therapist. The exercises must be performed without pain (within a pain-free range of motion).
Muscle contraction should be maintained for 5-10 seconds. Perform 5-10 repetitions in each direction, 3-5 times per day.
- Plantar flexion – the foot is bent towards the head.
- Dorsiflexion – the foot bends towards the head.
- Inversion – the foot turns inwards (towards the center of the body).
- Eversion – the foot rotates outward (away from the midline of the body).
Isotonic exercises
Resistance is provided by a contralateral foot, an elastic band, weights, or a physical therapist.
When is it normal?
Studies have shown that children as young as five years old can walk on their toes for no reason without any impact on their health. In young children, this is due to the immaturity of the nervous system and lack of muscle development. With increasing age, this idiopathic gait disappears spontaneously and without treatment.
According to doctors, there is no need to worry if a child occasionally walks on tiptoes in the following cases:
- The motor skills are age-appropriate;
- The child has no developmental delays;
- He occasionally walks on tiptoes and places his foot in the correct position;
- There is no motor coordination disorder;
- Both feet go on tiptoes.
Sometimes toe walking is hereditary if one parent walked on tiptoes as a child.

It can be caused by premature birth.
What to do if your child walks on tiptoes?
If the child walks on tiptoes most of the time, he or she should see a doctor. First, the condition should be assessed by a pediatrician, then by a neurologist and an orthopedist.
A comprehensive treatment includes special therapeutic physical exercises and foot massages. A simple exercise – squatting on a small chair – helps. The child cannot stand on tiptoes, but has to stand up with the whole foot.
Massage helps improve blood flow to the calf muscles, their nutrition and growth.
A course of 10 sessions with short breaks is effective. Parents can learn this technique themselves with the help of a professional.
In neurological diseases, drugs are administered to inhibit the pathological impulses and reduce the number of contractions.
Different forms of muscle hypertonicity can be treated with physiotherapy:
Neurologists and orthopedists recommend that these young children always wear shoes. In mild cases, this can be any footwear with a stiff heel and an orthopedic insole. In severe cases, orthopedic insoles or special joint splints are used. In the case of a shortened Achilles tendon, surgical correction is required. Surgery increases the length of the ligament.
The child walking on tiptoes is one of the symptoms to look out for. If the condition is corrected in a timely manner, it is easy to tolerate and has few consequences. If left untreated, clumsy gait, bowing of the legs and the development of flat feet are possible.
The answer to the most important question: Is it worth the pain?

Statistically, 5 % of children in the world occasionally walk on their toes for no reason. This often begins by the age of one and a half, and by the age of 5 or 6 the habit goes away on its own.
When is toe walking normal?
It is completely normal for your child to start walking on their toes when they are just learning to move on their feet. Always be guided by your child's age and remember that The ability to walk develops before the age of two. There is no reason to panic, run to the neurologist or orthopedist and ask about orthopedic shoes.
It may happen that the child first begins to walk properly, that is, to take full steps on the foot, and then begins to trot on tiptoes. This is normal and only means one thing – the child is learning and securing their new skills.
It's also normal for a toddler to stand on their toes every now and then. However, it is important to pay attention to the presence or absence of other complaints or symptoms. You can always ask the pediatrician who is observing the child about this.
If a parent is holding the baby's hand and the baby suddenly starts walking on tiptoes, this is also no reason to panic. Your baby learns a new skill every day. All children try different ways of walking until they learn to do it correctly and confidently. And walking on tiptoes, among other options, is also possible and normal.
How do you know that walking on tiptoes is not normal?

If a child older than three years old suddenly begins to tiptoe while walking, or if he has been doing this for a long time and the habit has still not disappeared, it is necessary to consult a doctor. He or she will help understand, guide, and correct the problem.
Why does my child tiptoe? The main causes

Up to the age of 3 years
A condition in which a child walks on tiptoes until the age of three without any specific problem is called Idiopathic running. It occurs most often in children whose parents also walked on their toes when they were children (usually before the age of one). This means that the phenomenon can be genetically inherited. This gait requires no correction or treatment. If there are no underlying abnormalities, the problem will resolve itself without the need for medical intervention.
Other reasons why a child can walk on their toes:
Purchasing age-appropriate orthopedic shoes
Sometimes parents who want their child to walk faster purchase orthopedic shoes when their child tries to take independent steps for the first time. This is wrong and can be harmful. Such shoes disrupt the natural development of the feet. In addition, they are not suitable for healthy children.
Your child likes to do this
He has learned another skill and wants to consolidate it.
Your child moves frequently on the walker
The walker was originally developed for children with limited mobility to make it easier for them to get around. It is not recommended for healthy children. When a healthy child is in a walker, abuse (e.g. being too high) may force them to stand on tiptoes. This way he learns to walk on his toes.
The second possibility is that standing on a walker (especially over a longer period of time) reflexively encourages the child to walk on tiptoes. Later, learning to walk properly can be difficult.
Emotional shock or personality traits
The child is overstimulated, hyperactive, has a burst of energy or wants to show his temper. This can unbalance the child's nervous system. Toe walking can occur especially in times of great psychological stress. In this way, the child tries to cope with feelings that he does not yet understand. In addition, very shy children walk on their tiptoes as if they were crawling, trying to be inconspicuous to others.
Chaplin's gait
The Chaplin gait is characterized by strongly spread legs and steps on almost straight legs. This gait leads to twisting of the hip joints due to muscle tension. While Chaplin films evoke positive emotions and nostalgia, as soon as parents see their child walking in this way, the question arises: 'Is everything OK? While this can be seen with the naked eye in older children, the condition is not always obvious in younger children.
- If the child is still walking, it is worth paying attention to how he stands in the bed (especially with loft beds). If his feet are always pointing to the side, it is possible that his feet are turning outwards.
- As your baby begins to walk, make sure his knees are not pointing in opposite directions.
TIP: When your baby is just learning to walk – Do not put on a diaper or hang toys on the belt. Nothing should hinder your baby's first steps.
In most healthy children, the problem resolves itself: over time, the pelvis separates completely. However, if the child has already separated and the problem persists, exercise can help. If the problem is ignored, there is a risk of developing clubfoot.
clubfoot
Clubfoot is a very common problem that is congenital in most cases. It is a deformation of the bones, joints, ligaments and feet in the womb. Clubfoot can be detected by ultrasound during pregnancy and treated from birth.
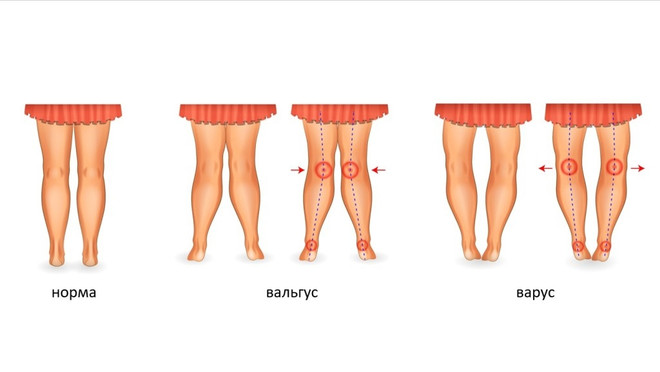
However, there are cases when clubfoot is acquired as a result of untreated foot problems - Chaplin gait, varus and valgus deformities.
TIP: Do not correct a clubfoot by intentionally turning the feet inward. This can lead to a valgus foot.
An acquired clubfoot is always the result of a previous problem. The above deformities should therefore be taken seriously to prevent them from developing into clubfoot.
Child development: Does the gait need to be corrected?
Tiptoe walking is not a harmless symptom that can be dismissed. It is a serious sign that the child's development is not progressing completely normally. Such a gait in an infant is a sign of serious muscle contraction and possible limitation in the mobility of the cranial sutures. Furthermore, this reaction is not random. It just so happens that this type of walking is best for this child at this time. There is no point in correcting them artificially.
Some parents follow the recommendations of experts and put their child in orthopedic shoes with a stiff sole, supination and a shaft that immobilizes the foot and ankle. The only problem is that the special footwear has no effect on the development of the child, that is, it eliminates the effects, but not the cause of the pathology. The only problem is that the special footwear has no effect on the development of the child, that is, it eliminates the effects, but not the cause of the pathology. Wearing orthopedic shoes cannot affect the brain centers responsible for muscle tension. In addition, if the dura mater and suboccipital muscles are tense, orthopedic shoes can worsen the problem rather than solve it.
During birth trauma, the baby's muscles constantly receive nerve impulses from the brain, causing them to contract. This reaction is the only way to relieve tension along the entire posterior muscle chain. When parents put an orthopedic shoe on the baby, the calf muscles are stretched and the nerve impulses continue to come. If the muscle doesn't have the opportunity to respond and contract, it can eventually collapse. And it will be more difficult to recover.
There is an opinion that children 'outgrow' this pathology and after a while begin to walk normally with the whole foot. This is actually very often the case, and visually it may seem as if the problem has gone away. However, this is not entirely true. After a while, the child will actually stand on their whole foot because their own weight will definitely put pressure and overwhelm the tense muscles. However, this can lead to other problems: in the future, the child, and later the adult, will quickly tire the calf muscles and will experience some pain when massaging this area. Walking becomes difficult and after a while the muscles can even atrophy. In general, if the problem is not solved, it will not go away.
How to help your child: advice for parents

If your child only walks on their toes, the first thing you should do is see a specialist. A neurologist is the first port of call. In some cases, it may be useful to see an osteopath who can help restore the correct position of the skull bones and ensure that the subcortical centers of the brain receive proper blood flow. The doctor will also help relax the muscles in the neck and relieve pressure on the dura.
This is best done in conjunction with massage sessions. Treatment should begin as early as possible because the smaller the child, the easier it is to restore the position of the skull bones as long as the injury has not yet 'fused' with the body.
If it is not possible to take the child to an osteopath, a chiropractor can be consulted. In this case, the use of so-called 'trust' techniques (quick and selective manipulation), which can cause crunching and cracking of the joints, should be avoided.
Children with this pathology benefit from swimming and therapeutic exercises. Swimming is a sport that almost everyone can do. In the swimming pool, the whole body is trained evenly, which strengthens the muscles and relieves excessive tension.
Walking barefoot on uneven ground brings good results. In summer the child can run on the lawn in the garden shed or on stones on the beach, and in winter on a massage mat at home.
It is important to know that gait disorders do not disappear immediately, even if the osteopathic doctor does a good job, in combination with massage. Initially, the child will only occasionally stand on one full foot. As the muscles relax, this will happen more and more often, and eventually the child's gait will be completely normal.
Read more:- Causes of tiptoe walking in babies.
- Tiptoe as an adult.
- Tiptoe walking.
- Why people tiptoe.
- Why girls tiptoe.
- A person walks on tiptoe.
- Toe movement in children.
- The child walks on its toes.