It is very important that the insoles are shaped in such a way that all the individual nuances of the foot are taken into account. The European Center for Orthopedics and Pain Management produces insoles with an innovative technology that determines the correct foot configuration using a unique device and special information tests. The insoles can then be adapted to the changing condition of the foot.
- Prevention of heel spurs
- The right footwear
- What you should know about flat feet
- First-class care: what modern diapers can do
- Physiotherapy for flat feet
- Rule
- Exercises for preschool children
- Step aerobic exercises for health and fitness for older preschool children
- Connection № 1.
- Small ball ensemble for preschool children
- What do you need to get started?
- What is heart failure?
- What types of heart failure are there and what are their symptoms?
- Left-sided heart failure
- Right-sided heart failure
- Running children and the phenomenon of toe walking
- keywords
- Introduction
- Benefits of physical therapy for flat feet
- Read the article
- contraindications
- Adverse effects of NSAIDs
- What can NSAIDs be replaced with?
Prevention of heel spurs
Heel spurs are an extremely painful condition. In advanced cases, it can lead to disability if the foot loses mobility and the patient can only move with crutches. Can this pathology be prevented, and if so, how?
Prevention of foot problems should be addressed from an early age: literally from birth, and prevention of rickets in infancy. Consider a vitamin D regimen (especially in areas with little sun) and regular visits to the child's orthopedist.
In addition, preventing plantar fasciitis is all about foot care, a healthy and active lifestyle, and timely treatment of musculoskeletal system diseases.
Let's talk briefly about each point.
The right footwear
The foot bears the shock loads that occur from constant walking, running and jumping. Choosing the right footwear is therefore very important. It is no coincidence that women - lovers of high heels and tight shoes - often suffer from heel spurs. There are certain orthopedic recommendations that should be followed at any age:
- Footwear should be selected depending on the type of activity (walking, working, shopping, sport), e.g. B. for walking it is advisable to choose shoes with a wide and stable heel of up to 4 cm and a rounded toe, for physical education the sole should be padded;
- for sports: lightweight running shoes with flexible toe box and air pockets, aerobic shoes with cushioning to protect against injuries, good padding, etc.
- Avoid shoes with a hard sole, flat and without sole;
- shoes should be sized to fit without resting on the toes, taking into account the size of the foot;
- It is best to choose shoes in the evening, as the foot is wider and swollen at the end of the day;
- When trying on shoes, wear two shoes and walk around the store; the shoes should not be uncomfortable, they should not 'stretch' or 'wear out';
- Shoes should be made of natural materials such as suede, leather or fabric; Rubber shoes can be worn in rainy weather, but should not be worn all day long.
- Older women should prefer shoes with Velcro or laces so they can be easily repaired.
What you should know about flat feet
A healthy foot has 3 points of support: the heel and the heads of the first and fifth toe bones. If this position is disturbed, the foot cannot provide the body with the necessary cushioning during movement. As a result, the spine and joints suffer, and scoliosis, arthritis and other diseases occur that reduce the quality of life. It is important to treat flat feet early.
The cause is weak foot muscles that cannot shape the foot properly. The bones begin to deform. If treatment of the disease is delayed, it is very difficult to restore the normal position of the foot in adulthood.
Parents should know that flat feet can only be diagnosed after the age of five. However, you should see the orthopedist much earlier. The doctor can detect bone deformities and early signs of rickets and determine normal posture and gait. This is very important for the health of the bones and muscles of the foot.
To prevent the development of flat feet, the child should be physically active and wear comfortable and correct shoes with an insole and a firm back. At the first signs of the disease, a doctor should be consulted and physiotherapy should be started.

First-class care: what modern diapers can do
Physiotherapy for flat feet

Physical therapy for children with deformed feet is carried out in the form of games. Good results are achieved:
As fitness increases, the LFC exercises and the pace at which they are performed should become more difficult. The child should learn to hop on different parts of the foot and walk on the outside and inside of the foot. These exercises strengthen the muscles and ligaments of the foot and shape its correct alignment.
At the age of 5-6 years it is easiest for the child to regain foot health. It is important that the child understands why he is being treated and that he enjoys the exercises. If we correct the position of our feet at a young age, we don't have to worry about flat feet later.
It should always be remembered that any procedure to correct foot position should be carried out under the supervision of an orthopedist. Only he or she can choose the appropriate LFC exercises and their load. These exercises can be performed in a specialized physical therapy practice or at home. Start with a general warm-up and only then move on to specific exercises. The frequency of the training sessions is 15 minutes twice a day.
Rule
A daily routine that includes regular exercise is important. The exercises can be done in the form of games and it is advisable to have a wall bumper as it has a good effect on the feet. The child should understand and walk on the toes, heels, inside and outside of the foot, jump, train the foot with special accessories - massagers, a roller.
Soft, flat shoes should not be worn until the foot has improved, especially in the formative age of the foot, and girls should not walk in heels or pointed-toe shoes. Supinators can be worn by school-aged children, but orthotics and orthopedic shoes are not advisable at younger ages as they weaken the muscles, which is bad for the misshapen foot.
Recommended physical activities include swimming, playing ball and running, although the intensity should be increased gradually. As with any exercise, the initial workout should last no longer than 15 minutes. Remedial gymnastics should be performed barefoot three times a day and must not be too strenuous or cause muscle pain.
Exercises for preschool children
Choose five exercises and increase the number of exercises. It is advisable that the exercises are not simply performed as gymnastics, but that they become games. This prevents the child from becoming tired and feeling stressed.
- While sitting, bend and stretch each foot ten times.
- Let your feet vibrate while standing.
- Roll on your feet from toes to heels, up to 10 times.
- Walking on toes and heels, on the inside and outside of the foot.
- Perform a half squat on tiptoes.
- Use your toes to pick up pencils and toys from the floor.
- Drawing with a pencil (this exercise is particularly fun for children).
Step aerobic exercises for health and fitness
for older preschool children
Connection № 1.
In a well-ventilated room, the bars are placed on the floor one after the other. With cheerful, rhythmic music, the children enter the room and stand behind the bars. (Children in light-colored clothing, barefoot).
Preparatory phase.
1. Walking in place. (The children have to feel the music, grasp the tempo, tune in to it).
2. Walking at a walk.
3. Backward march from the step to the floor and back to the step, with the right foot, quick hand work.
4. go backwards from the step, go forward from the step.
5. walk on the step; Hands alternately forward, up, forward, down.
Core part 1.
1. Walk on the step, hands alternately drawing large circles along the body, fingers clenched into fists.
Step on the step - away from the step, making small circles on your torso with your hands one after the other.
(Repeat 1 and 2 three times).
3) Step to the right and left, arms stretched, lifting forward and down at the same time.
4) Step on the right-left step with half squat (step – squat); the arms are bent at the elbows to the shoulders, downwards.
5. March on the step, lifting your knee up while clapping your straight hands forward and back.
6. Step onto the step - away from the step with straight hands clapping front and back.
(Repeat 3, 4, 5 and 6 three times).
7. Jog in place on the floor.
8. Light jogging on the step.
9. Jog around the step.
10. Jog around the step.
(Repeat 7, 8, 9 and 10 three times).
11. Regular walking on the step.
12 Walk around the step on tiptoes, alternately lifting your arms.
13 Walk sideways from step to step.
14 Walk around the step on your heels, raising and lowering your arms at the same time.
15 Walk sideways from step to step.
16 'Cross'. step from the step – forward; from the step – back; from the step – right; from the step – left; Hands on waist.
17. Do the same with dance movements with your hands.
18. Breathing exercises.
19. gradual walking.
20. Go from step to step, hands up to shoulders.
Walk one step with your legs half bent, hands on your waist. 22.
Walking in circles with clapping over your head.
23. Climb a step from a step.
24 repetitions in a circle. Walk in a circle on one step.
Small ball ensemble for preschool children
1. musical part. Introductory part.
Exercises on the wall for correct posture (3-4 exercises). walking in a column alternating with running; Walking on tiptoes, on heels, on the outside of flat feet; Weaving between the running boards and jumping over them; Walking on correction tracks (while walking, children take a small ball in their right hand); Realign in groups of three to the running boards (pre-spreaders); Walking in place: turn to the running boards.
Bulk is divided into four musical sections. Step planks exercise with a small ball:
1. P: Standing on the step, ball in right hand. Step forward from the step, pass the ball overhead to the other hand; return to the starting position.
2. p: Same. Step back, pass the ball over your head to your other hand; back to HP.
3. p: Similar. Step back and forth, passing the ball from hand to hand over your head.
4. pos on step, ball in right hand. Step forward with the right (left) foot in front of the step and at the same time bring the right (left) hand forward with the ball; back to p., pass the ball to the other hand.
5) Back to pos Perform the same movement to the right (left) of the step.
6. p: os Perform the same movement backwards from the step.
7. p: os on the step, arms stretched to the sides, ball in the right hand. Lunge to the right (left) from the step, three swings, back to HP, pass the ball to the other hand.
1. os on step, hands forward, ball in right hand. Turn to the right (left), fingers up and the right (left) hand with the ball backwards. Return to your hips and pass the ball to your other hand.
2. ip: Same. Same rotation to the right (left), but alternately placing your foot behind the step board. Right turn - right leg: Left turn - left leg.
3rd P.: os on step. Step outward with right (left) foot behind footboard; hands forward; put down the ball; back to the starting position.
4th P.: os on the step, ball in the right hand. Place your right (left) foot behind the running board and stand on your toes; Raise your hands up, put the ball down; return to the starting position.
5) Back to pp: os in front of the step, ball in right hand. Step on the step and place the ball above your head; return to the HP.
What do you need to get started?
Very little: sticks, comfortable clothes, shoes and a good mood. As with athletic walking, comfortable footwear is important - sports shoes. Some people complain that Nordic walking is a Western fad, a business focused on selling sticks. But no one forces you to buy something expensive right away. Many people start with the cheapest lightweight poles that you can buy on any Chinese website. The poles should fit your height And remember that hiking poles are very different in length from ski poles: if you take the 'real' hiking poles, you will notice that the part of your arm from elbow to wrist is now exactly parallel to the ground.
Walking with sticks takes about 40-50 minutes, So it's a good way to start the day or an evening walk in the park or nearby forest. After the first walk, it is difficult to understand the 'salt' of the sport: many people don't even break a sweat. But they usually have sore muscles the next day. You can hike in any weather, barring natural disasters. Even in snow and ice, the sharp points on the ends of the sticks, which are covered with a 'boot' in the warm season, help to prevent the sticks from rubbing on the pavement.
Photo. sumke24.ru
If you hesitate to run with sticks in public places, remember that jogging also existed in the past (former US President Jimmy Carter practiced it for the first time) and people also looked at it with amazement. And if you still can't decide to walk alone, do Nordic walking in a group under the guidance of a trainer or train outside the city.
As a reminder: 30 minutes of walking a day can help, among other things to prevent the development of cancer.. Yellmed has already talked about this. This is what experts from Harvard University assure. Studies with breast and colon cancer patients have shown that. regular physical activity has a major impact on life expectancy.
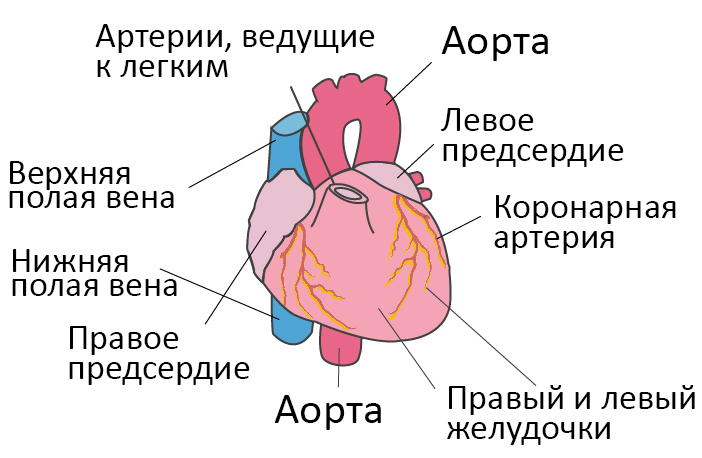
What is heart failure?
In a healthy heart, oxygen-rich blood is pumped from the left ventricle through the body to the organs and supplies them with oxygen and nutrients. After supplying the organs, the oxygen-poor blood returns from the body to the right side of the heart, from where it is transported to the lungs. In the lungs, the blood is enriched with oxygen so that it can be pumped back through the body by the left ventricle.
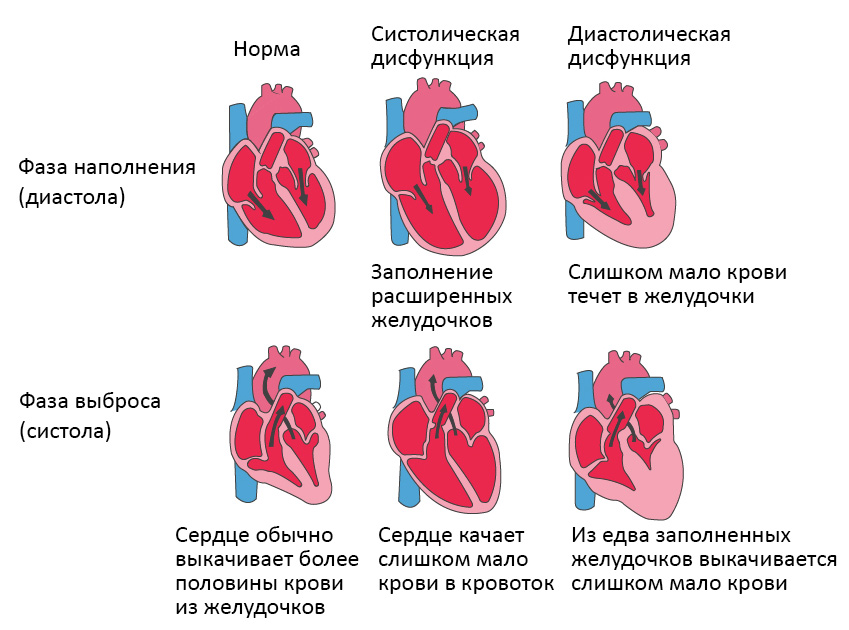
Heart failure is an impairment of the heart's blood pumping function. As a rule, either the right side of the heart (right-sided heart failure) or the left side of the heart (left-sided heart failure) is affected. In advanced heart failure, both sides of the heart can be affected (global heart failure). Heart failure can also be chronic or acute. Chronic heart failure is more common than acute heart failure, which occurs suddenly and unexpectedly. Acute heart failure can occur suddenly on the background of an acute cardiovascular accident and/or congestive heart failure.
What causes heart failure?
Heart failure is caused by diseases that attack or damage the heart muscle. The most common cause of chronic heart failure is coronary heart disease (CHD).
Coronary heart disease (CHD) is caused by a narrowing of the coronary arteries, usually as a result of atherosclerosis. The coronary arteries are the vessels that supply oxygen and other important nutrients to the heart. Progressive narrowing (also called stenosis) of the arteries leads to poor blood flow to the heart muscle. Irritable bowel syndrome is often diagnosed when angina pectoris (chest pain and tightness) occurs, but otherwise goes undiagnosed.
What types of heart failure are there and what are their symptoms?
Each type of heart failure has different symptoms, and the intensity of the symptoms can vary. However, the main symptom of heart failure is shortness of breath during exercise or at rest. Warning signs may include sweating with mild exertion, inability to lie flat, chest tightness, or swollen feet.
Left-sided heart failure
The left side of the heart is responsible for pumping oxygen-rich blood to organs in the body. In left-sided heart failure, the pumping function of the left ventricle is restricted, so that oxygen-rich blood is no longer pumped through the body in sufficient quantities. Instead, the blood remains in the pulmonary circulation, which can lead to fluid buildup in the lungs (pulmonary edema), difficulty breathing, throat irritation, a 'rattling' sound when breathing, weakness or dizziness.
It is most commonly caused by coronary artery disease (CHD), high blood pressure or a heart attack, more rarely by heart muscle or heart valve failure.
Left-sided heart failure can occur acutely or develop over time. It usually first becomes noticeable as shortness of breath during physical activity. In severe cases, it can even cause hypotension (low blood pressure) at rest.
Right-sided heart failure
The right side of the heart is responsible for transporting oxygen-poor blood back to the lungs. In right-sided heart failure, the right ventricle of the heart does not work properly. This causes increased pressure in the veins, forcing fluid into the surrounding tissues. This causes swelling, particularly in the feet, toes, ankles, and lower legs. It can also lead to an acute need to urinate at night when blood flow to the kidneys is better.
The cause is usually an acute or chronic increase in pulmonary blood flow resistance. Caused by lung diseases such as pulmonary embolism, asthma, severe emphysema, chronic obstructive pulmonary disease (COPD, usually caused by tobacco use) or left heart failure. Rare causes include heart valve problems or heart muscle disease.
Running children and the phenomenon of toe walking

The meaning of. A review of studies found little evidence of the possible influence of walking aids on the development of toe walking.
Hypotheses and research objectives. The present study investigated a hypothesis about the emergence of an abnormal movement pattern in the form of a preferred movement without heel support when using walking aids. The aim of the study was to identify a series of epidemiological aspects related to the use of walkers, to identify the abnormal movement pattern in the form of toe walking, to determine the validity of its association with walkers and to evaluate the characteristics of the phenomenon.
Materials and Methods.. Three retrospective cohort studies were conducted. A total of 749 children were included in the studies; the number of children in the learning-to-walk groups was 363. The methods chosen were an anamnestic survey of the parents using specially developed anonymous questionnaires and a statistical analysis of the data.
The results.. A decline in the use of walkers in the population has been noted over several years. The reasons for using baby walkers were identified. The relative risk of walking without heel support in the walking aid groups was calculated: RR2 = 3.555 (2.535-4.990 95% CI) and RR3 = 2.766 (1.178-6.494 95% CI) for the second and third trials, respectively. A longer duration of toe walking was found in the 'walking' group: M gen = 14.58 ± 3.49; 11.09-18.07 months (95 % KI). An increased correlation between toe walking and walking aids was found with longer periods of use. The population-based risk of toe walking in the walker group was calculated: PAR = 19.647 %. The study found no static deformations associated with the use of walkers.
conclusion. Walkers have been identified as a contributing factor to toe walking patterns. It is possible that walking aids are an etiologic factor in idiopathic toe walking.
keywords
Introduction
In today's world, humans are influenced not only by natural factors but also by the human environment. This influence begins in infancy, including through the use of various devices: cots with electronic components, development mats, automatic rockers, 'jumpers', etc. This article presents the data from a study on some aspects of the effects of a device called a 'walker' . The question of the effects of walkers on infants has repeatedly arisen in the world scientific community, but information about the negative effects is not sufficiently comprehensive.
The modern baby walker is a technical device on wheels that keeps the child upright. The exact time when the baby walker was introduced in this form is not known. However, the first patents for improvements to the walker were registered in the 1880s. [1, 2].
Baby walkers are used extensively by parents around the world and for a variety of reasons. Researchers in Dublin, Ireland (1995) found that 55 % out of 158 infants had been in such devices for some time. The main reasons given were the baby's positive emotions and early experiences with older children [3].
A survey in the USA (Virginia, 1998) found that 77 % of 119 firstborns and 85 % of second and subsequent babies had used a walker with their parents. Of those surveyed, 78 % thought the walker was useful and 72 % expected it to promote their child's development [4]. In Austria (1994), a study of families with small children aged 2 to 6 years found that 55 out of 240 respondents used a baby walker [5].
In the United Kingdom (Nottingham, 1998), 55 % of 2152 children surveyed had a walking aid [6].
A study in Iraq (Baghdad, 2006) found that 83 % out of 100 infants (44 % girls, 39 % boys) between the ages of 5 and 8 months used a walker. The reasons were: 'to keep the child busy'. – 71 %; 'to let the child walk sooner' – 54%; and 'to strengthen the legs'. – 28% [7].
Benefits of physical therapy for flat feet
Physical therapy for flat feet should be started as early as possible. The feet are closely related to posture and the musculoskeletal system, so regular physical activity helps reduce deformities, build muscle strength and endurance, keep the feet in the correct position when walking, and prevent scoliosis. Most exercises can be done at home. The exercises should only be started after consulting your doctor and undergoing an examination. Standing on the floor is not recommended at first so as not to put too much strain on your feet. The load should be increased gradually. To reduce the degree of flat feet, it is useful to do exercises that involve grasping and moving small objects with your toes. Rolling objects helps relieve pressure on the foot and reduce pain and other symptoms. Walking barefoot on pebbles or sand is helpful for flat feet because it affects the reflex zones of the foot. You can also walk on a rope or gymnastic bar that lies on the floor. The therapeutic exercises should be performed 2-3 times a day. In addition to exercises, podiatrists recommend walking on your toes and heels, alternating between the inside and outside of your feet. This type of walking helps tone the calf and thigh muscles and also strengthens the back muscles. You can walk barefoot or in special shoes with balls of your feet.
Read the article
contraindications
- cardiac and respiratory failure;
- skin diseases;
- severe restless legs syndrome;
- infections;
- viral diseases.
Sitting on a mat, you can perform the following exercises:
- Extend your legs forward. Slowly alternately bend and straighten the toes of your feet.
- Continue to pull your legs further apart and bring your feet closer together.
- Bend your knees. Bring your heels together and spread them apart without lifting your toes off the floor.
- Bend your left knee. Spread one foot up and back over your right shin.
- Pull your toes in and out.
- Stretch your limbs forward. Grab the ball and lift your feet off the floor.
- Try to kick the ball up.
- Bend your knees. Roll the ball along the foot from heel to toe.
Make sure that your back stays straight.
Perform the following exercises while sitting on a chair:
- Alternately bend and straighten your toes.
- Pull your toes in and out with great force.
- Make circular movements with your feet inward and then outward.
- Open and bring your heels together without lifting your toes off the floor.
- Alternately lift your heels and toes off the mat.
- Alternately raise your right and left legs as high as possible.
Perform the exercises while sitting and using a handheld device:
- Throw a few pieces of fabric on the floor. Try to catch the fabric with your fingers and toes.
- Roll a ball or pencil with your feet. Use your feet to pick up an object from the floor.
- Roll small objects on the floor.
Practice in a well-ventilated room, in comfortable clothing, and with bare feet.
Adverse effects of NSAIDs
Even short-term use of NSAIDs can cause serious side effects in many patients. The most common side effects of NSAIDs include:
Platelet aggregation disorders
undesirable effects on the cardiovascular system
The side effects of NSAIDs are associated with inhibition of the activity of the physiological isomer of COX (COX-1). Other undesirable effects occur less frequently. The most common adverse effects are coronary heart disease, diabetes mellitus and renal failure in the elderly with comorbidities when taking NSAIDs for a long time.
The risk of serious complications increases as follows: Ibuprofen, Diclofenac, Naproxen, Indomethacin. For most NSAIDs, the risk of gastrointestinal bleeding peaks on average on the eighty-fourth day of treatment, and for indomethacin within the first seven days. The endoscopic features of NSAID-induced gastropathy that distinguish it from Helicobacter pylori-related ulcers are the predominant location of the lesions in the antral part of the stomach and moderate to minimal signs of mucositis.
There is a relative risk of serious gastrointestinal complications:
- knowledge of previously diagnosed peptic ulcer disease;
- use of high doses of NSAIDs;
- simultaneous use of different groups of NSAIDs (including low-dose aspirin);
- Older age (over 70 years);
- Anticoagulants and high doses of glucocorticosteroid hormones.
If there is a risk of gastrointestinal complications from NSAIDs, doctors at Yusupov Hospital prescribe synthetic prostaglandins and proton pump inhibitors. H2-histamine receptor blockers are effective in the treatment of NSAID-induced duodenal ulcers and erosions, but not gastric ulcers. Proton pump inhibitors appear to be more effective than histamine receptor blockers and misoprostol. Proton pump inhibitors should be used for at least four weeks. For larger ulcers and localized stomach ulcers, this period varies from eight to 12 weeks. 'Gastroprotectors' are taken for the duration of NSAID treatment.
What can NSAIDs be replaced with?
Nonsteroidal anti-inflammatory drugs (NSAIDs) are medications used for the primary treatment of arthritis. There is no complete replacement for them. To avoid or limit the side effects of NSAIDs, doctors at Yusupov Hospital provide comprehensive treatment for patients with arthrosis, use optimal doses of drugs and observe the maximum permissible duration of anti-inflammatory therapy.
For osteoarthritis, patients use topical forms of NSAIDs (gels, ointments, and creams). These have a satisfactory analgesic effect on pain associated with joint damage and are safer than the drugs available in powder and tablet form; If the pain is severe, opioid analgesics are prescribed. Tramadol is used to treat severe pain when paracetamol and NSAIDs are ineffective or when these medications cannot be prescribed in sufficient doses.
Slow-acting symptomatic medications include colchicine. It is used both as monotherapy and in combination with selective or non-selective NSAIDs. In the latter case, there is a significantly increased risk of inhibition of white blood cells and platelets. Colchicine is indicated for generalized polyarthritis with severe inflammatory and painful components unresponsive to standard treatment.
Intra-articular corticosteroid injections are used to relieve severe secondary synovitis in arthritis. Glucosamine sulfate and chondroitin sulfate are used for the symptomatic treatment of arthritis. The drugs have a moderate, delayed analgesic effect that is often greater than therapeutic doses of ibuprofen in patients with moderate osteoarthritis of the knee, hip and hand.

Hyaluronic acid has a moderate pain-relieving effect. Two types of hyaluronic acid are used in the treatment of arthritis: low molecular weight and high molecular weight. The latter has a stronger pain-relieving effect that lasts three to twelve months.
Read more:- Bracers for children with cerebral palsy.
- lateral bone.
- Toe movement in children.
- Tiptoe as an adult.
- Walking school with prosthesis.
- Tiptoe walking.
- Walking in heels.
- legs 14 years.