When amoxicillin is administered intravenously or intravenously, the concentration of the active substance in the blood is similar. The active ingredient binds to plasma proteins to around 20 %. The active ingredient is distributed throughout the body in the fluids and tissues. Higher concentrations of the active ingredient are observed in the liver.

- longitudinal vault
- Metatarsal arch
- Side bow
- function
- Transverse arch of the foot Latin
- Projection of the lateral neurovascular bundle onto the skin
- The most important anatomical axes:
- Fitness training courses for trainers.
- Symptoms of transverse flatfoot
- Diagnosing flat feet
- Possible complications
- diagnosis
- Structure of the temporomandibular joint sinus structure
- Types of sinuses
- Superior sagittal sinus
- Inferior sagittal sinus
- Direct sine
- Instructions for use for Bac-Set® Forte
- Holder of the registration certificate:
- overdose
- interactions
- Why do customers choose ortmann-pro insoles?
- How orthopedic technicians make ORTMANN-PRO insoles
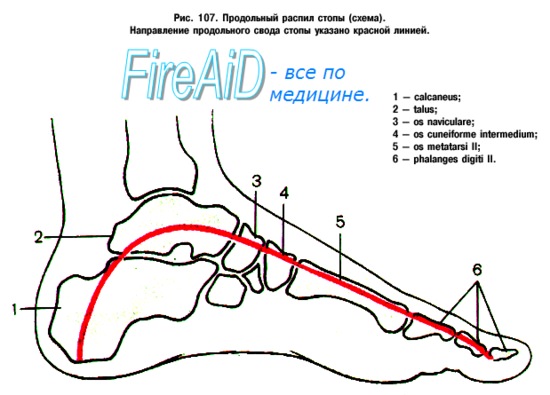
longitudinal vault
The longitudinal arches of the foot can be divided into a medial and a lateral arch.
Metatarsal arch
The metatarsal arch is higher than the lateral longitudinal arch. It is composed of the heel bone, the talus bone, the scaphoid bone, the three sphenoid bones (medial, medial and lateral) and the first, second and third metatarsals.
Its apex lies on the upper articular surface of the talus, and the two shanks or supports on which it stands are tubercles on the sole surface of the talus. the calcaneus behind and the heads of the first, second and third metatarsals in front. The main characteristic of this vault is its elasticity due to its height and the number of flat joints between its components.
Its weakest part (that is, the one most susceptible to deformation in the event of excessive pressure) is the joint between the talus and the heel bone, but this part is bound by the plantar heel ligament, also called the elastic ligament, which is elastic and therefore capable , to quickly return the vault to its original state when a hindering force subsides. This ligament is strengthened medially by its connection to the deltoid ligament of the ankle and is supported from below by the tendon of the posterior tibial muscle, which runs in a fan shape and prevents the ligament from being overstretched or stretched to the point where it stretches.
The arch of the foot is additionally supported by the soleus tendon, the small soleus muscles of the foot (short muscles of the big toe), the tendons of the anterior and posterior tibialis and the tendon of the peroneus longus, the flexor digitorum longus, the M. flexor hallucis longus and the ligaments of all involved joints.
Side bow
The lateral arch of the foot consists of the heel bone, the elbow, the fourth and fifth metatarsals.
Two notable features of this bow are its strength and its easy lift. Two strong ligaments, the long plantar and transverse plantar ligaments, along with the short muscle of the little toe, ensure its integrity.
function
In particular, the medial longitudinal arch creates space for elastic soft tissues that act like springs, especially for the thick plantar aponeurosis that runs from the heel to the toes. Due to their elastic properties, these soft tissues can transmit the reaction forces during contact with the ground over a longer period of time, thus reducing the risk of wear or damage to the musculoskeletal system; in addition, they can store the energy of these forces and return it to the next phase, reducing the cost of walking and especially running, where vertical forces are higher.
The anatomy and shape of a person's longitudinal and transverse arches can determine what type of injuries they are susceptible to. The height of the arch of the foot depends on the height of the heel bone. A collapse of the longitudinal arch leads to so-called flat feet. A person with a low longitudinal arch or a flat foot may stand and walk with a pronated position of the feet, with the foot pointing inward or twisted. This makes the person prone to heel pain, arch pain, and plantar fasciitis. People with flat feet may also find it more difficult to perform exercises that require weight bearing on the toes.
People with a high longitudinal arch or hollow foot tend to walk and stand with their feet in a supinated position, in which the foot rolls over or rolls outward. A high arch of the foot can also cause plantar fasciitis because it causes the plantar fascia to pull away from the heel bone. Additionally, a high or low arch of the foot can increase the risk of shin splints because the front shin muscle (tibialis anterior) has to work harder to prevent the foot from hitting the ground.
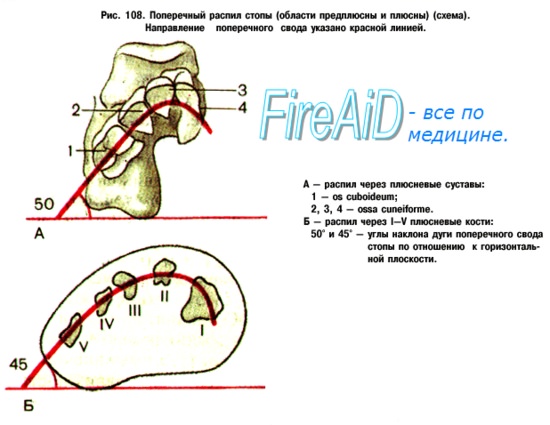
Transverse arch of the foot Latin
External landmarks of the sole of the foot. A longitudinal arch and two transverse arches can be seen on the surface of the sole of the foot. The lateral part of the longitudinal arch is formed by the calcaneus, scaphoid and metatarsal bones IV-V; the medial (elastic) part of the longitudinal arch is formed by the heel bone, the scaphoid bone, three sphenoid bones and the I-III metatarsal bones. Of the ligaments, the Lig. plantare longum, the longitudinal ligament, plays a crucial role in strengthening the arch of the foot. It begins at the underside of the heel bone, moves forward and attaches with deep fibers to the cuboid tuberosity and superficially to the base of the metatarsal bone.
It crosses the sulcus ossis cuboidei, the long sole band transforms this groove into a bony-fibrous canal through which the tendon of the fibularis (peroneus) longus muscle runs.

Figure 4.43. Longitudinal impressions (far right for flat feet).
The distal transverse arch is formed by the metatarsal bones and reinforced by the transverse head of the fibularis longus muscle. adductor hallucis; The proximal transverse arch is formed by the tarsal bones and reinforced by the tendons of the tibialis posterior and the fibularis (peroneus) longus.
When the reinforcing apparatus is weakened, the vault lowered and the foot becomes flattened, which leads to the development of flat feet as a pathological phenomenon (Fig. 4.43).
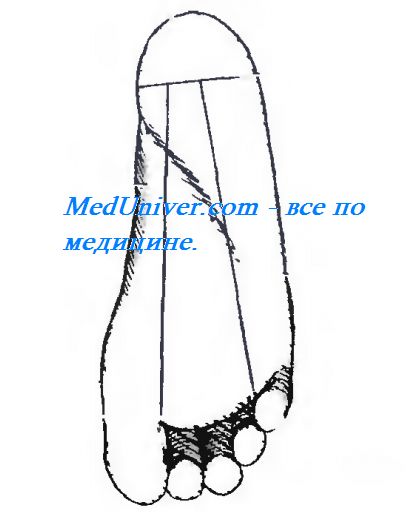
Fig. 4.44. Projections of the lateral and medial plantar hump.
Projection of the lateral neurovascular bundle onto the skin
Projection of the lateral vascular bundle onto the skin and the intermuscular septum corresponds to a line from the midpoint of the sole width (or from the midpoint of the line connecting the tops of the ankles) to the fourth interdigital space. The medial bundle projects along a line drawn from the midpoint of the inner half of the sole width to the first interdigital space (Fig. 4.44).
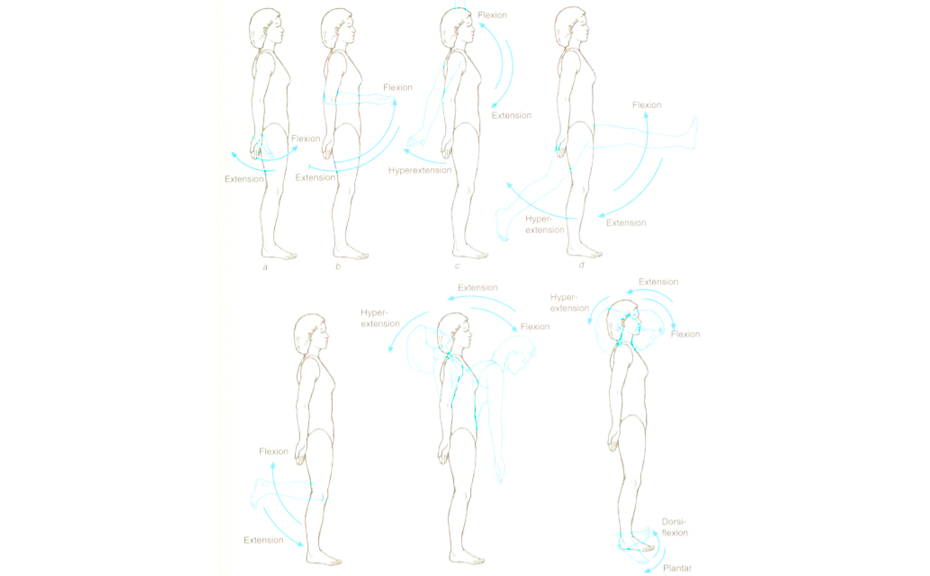
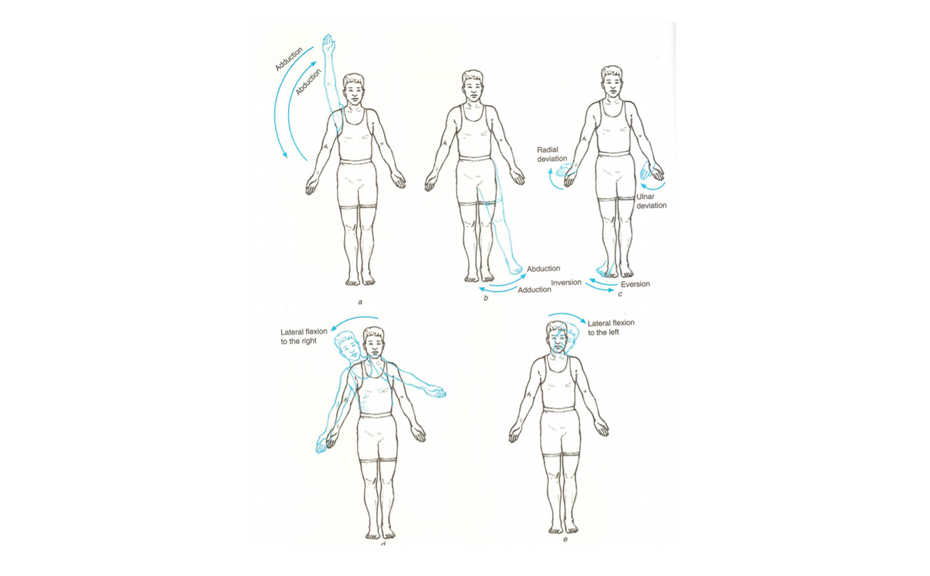
The most important anatomical axes:
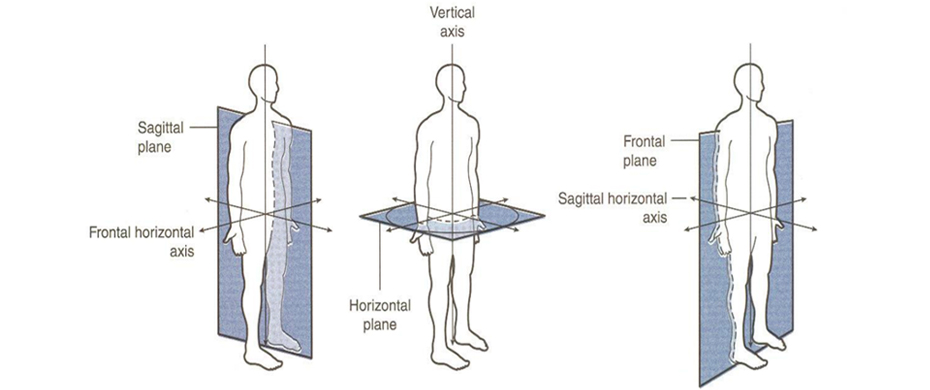
- Vertical axis (Vertical axisThe vertical axis is aligned along the body of a standing person. Example: Rotation in a joint is guaranteed around a vertical axis.
- Longitudinal axis – also aligned along the human body, but independent of its position in space. It runs along a limb (arm, leg) or along an organ whose longitudinal dimensions predominate over others.
- Frontal axisFrontal axisThe frontal axis is identical to the frontal plane. It is also called the transverse axis or horizontal axis. Example: The flexion and extension of a joint takes place around the frontal axis.
- The sagittal axis (Sagittal axisThe sagittal axis is similar to the sagittal plane and is located anteroposteriorly. Example: Abduction and adduction can be specified around the sagittal axis.
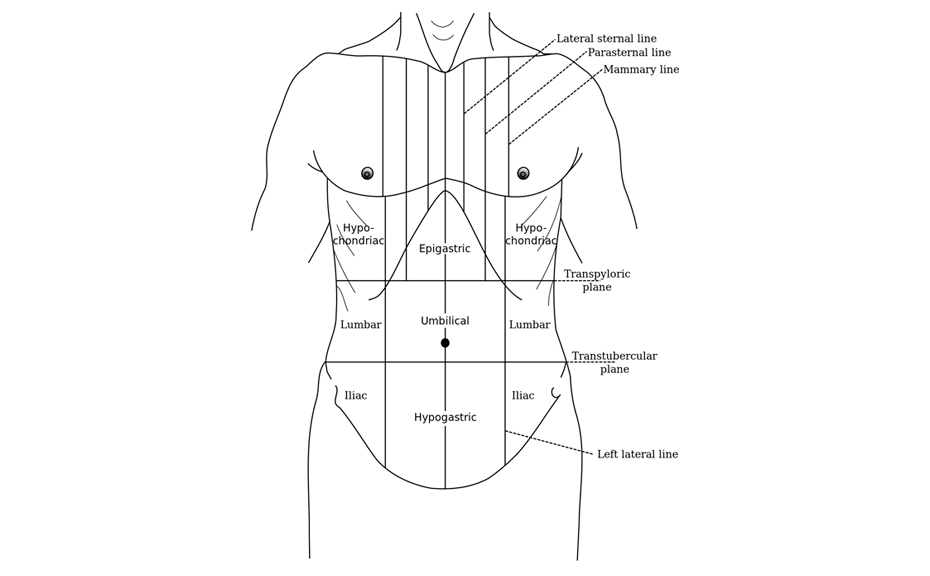
It is used to determine the projection of the organs of the thoracic cavity against the chest wall:
- Median line anterior (Linea mediana anterior) runs from the cervical notch in the middle of the chest through the navel to the pubic fold.
- sternum line (Sternum line (linea sternalis)) is located on the side of the bridge.
- The surrounding line (Sternal line (Linea parasternalis)) runs halfway between the line of the sternum and the midline of the clavicle.
- The midclavicular line (mastoid) (Linea medioclavicularis (mamillaris)) runs through the middle of the collarbone and the nipple.
- The anterior axillary line (anterior axillary line ( linea axillaris anterior) runs along the anterior edge of the armpit.
- The median axillary line (median axillary line (linea achillaris media)) runs through the middle of the armpit.
- The posterior axillary line (posterior line (linea achillarris posterior)) runs through the posterior edge of the armpit.
- The scapular line (Scapular line (Linea scapularis)) runs through the lower edge of the shoulder blade with the thigh lowered.
- The periocular line (thoracic line (linea paravertebralis)) runs midway between the scapular line and the spinous processes of the thoracic spine.
- Posterior median line (Linea mediana posterior) corresponds to the position of the spinous processes of the thoracic spine.
Fitness training courses for trainers.
For fitness trainers looking for courses that will increase their income, make them even cooler and ensure that they never face employment problems, we recommend the following distance learning courses:
Basic personal trainer course – For trainers who want to supplement their knowledge with basic information. An incredible amount of useful material that will take you to the next level.
upgrade – Online course for fitness trainers who want to increase their income and knowledge. Custom Themes.
architecture of the body – Dmytro Gorkovsky's special course with full-day practical and theoretical training for fitness trainers, massage therapists and doctors.
pregnancy – Training techniques for pregnancy courses and postnatal recovery.
Pilates – an online course by Kateryna Vasylenko about the techniques of the Pilates system.
Symptoms of transverse flatfoot
Symptoms of transverse flatfoot
– The most common are: Pains in the feet, Burning, cramps. In the muscles of the lower leg, fatigue Tiredness in the feet at the end of the day. In advanced stages, pain in the knee and hip joints as well as back pain are reported, which can lead to the development of arthritis. arthritis these joints can lead.
The forefoot visually enlarges and a so-called transverse foot is created. The abnormal load distribution caused by flat feet often leads to Deformation of the first toe The first toe is often curved into a valgus position. There is often an exophyte in the area of the first metatarsophalangeal joint of the big toe, which patients refer to as'Bunion' or 'bump''describe on the foot. The 2-3-4 toes, which are heavily stressed, take on a hammer toe shape. As the disease progresses, the changes become permanent in the form of a forefoot deformity, which leads to a disruption in the biomechanics of all parts of the musculoskeletal system involved in walking.
Diagnosing flat feet
Diagnosis of flat feet involves an examination by a specialist podiatrist. An x-ray examination of the feet. And an analysis of the patient's gait. If necessary, the examination can be extended.
Treatment of transverse flatfoot should be carried out by a traumatologist after a thorough diagnosis. Treatment depends on the degree of flat foot. Treatment of transverse flatfoot can be surgical or conservative (without surgery).
Conservative treatment of transverse flatfoot Treatment is complex and includes reducing the load on the foot, fitting orthopedic shoes, using orthopedic devices to normalize biomechanics and reducing excess weight. If there is synovitis or osteoarthritis of the first metatarsophalangeal joint, anti-inflammatory and pain-relieving medications are used to relieve the inflammation. In some cases, immobilization, physical therapy and massage are used to reduce the increased muscle tension and thus the pain. Conservative treatment aims to relieve pain and slow the progression of paraplegic flatfoot.

Preparing for surgery
Transverse flatfoot

surgery
In transverse flatfoot

Possible complications
Due to the loss of cushioning ability, the stress-bearing system experiences shocks when walking, which are transmitted upwards through the skeleton to the brain.
This can lead to various complications:
- altered and difficult gait (clubfoot);
- bad posture;
- pain in the feet and knees;
- foot problems (heel spurs, corns, valgus deformity, ingrown toenails);
- knee joint problems (laxity, menisitis, arthrosis);
- Diseases of the hip joint (coxarthrosis);
- Spinal diseases (radiculitis, scoliosis, osteochondrosis, intervertebral fractures);
- varicose veins;
- Headache.
diagnosis
The orthopedist is able to diagnose flat feet based on a visual examination. If necessary, instrumental diagnostics is carried out. The most commonly used method is plantography - the study of footprints. To determine the degree of pathology, the doctor sends the patient for an X-ray examination.
Complete healing and the correct shape of the foot can only be achieved at a young age, when the bones and musculoskeletal system are not yet fully formed.
In complicated cases, the orthopedic surgeon may recommend surgery.
In adults, therapy can only slow the further progression of the disease, stabilize the condition, relieve pain and strengthen the muscles and ligaments. In most cases, the doctor will recommend insoles to distribute the load on the foot and give it the correct shape and cushioning ability.
Structure of the temporomandibular joint sinus structure
The evolution of the temporomandibular joint collectors is due to their division into two lobes that resemble canals. These channels serve to distribute venous blood from the main human organ, which is then directed to several double vessels located in the neck that carry blood from the brain.
The TMO slats that make up the sine look like tight ropes that do not lose tension. This design allows blood to flow freely from the head and neck without affecting intracranial pressure in any way.
In humans, these variations of temporomandibular joint reservoirs are installed:
- Upper or lower sagittal joint. The former is located longitudinally at the upper edge of the sagittal bone and terminates at a fragment of the occipital bone, while the latter lies longitudinally at the lower edge of the sagittal bone and drains into the straight sinus;
- Straight sine. Located in the longitudinal direction of the fragment where the sickle process merges with the cerebellar nerve vessel;
- Transversal (double). Formed on the transverse process of the skull and runs longitudinally to the posterior edge of the cerebellar sulcus;
- Occipital. Located in the cavity of the cerebellar arch and continues to extend to the occipital bone;
- Sigmoidal. Located in the department in the ventral part of the cerebellum;
- Cavernous (double). Located on the sides of the wedge-shaped formation in the bone body (Turkish saddle);
- Cuneo-parietal sinus (double): Refers to the small border of the sphenoid bone and ends in the cavernous pelvis.
It is located near both edges of the temporal pyramid.
The collectors of the brain layer begin their anastomosis with the venous vessels on the surface of the brain through the venous branches that connect the vascular sinuses of the TMO with the external blood vessels of the head. These sinuses first unite with the diploid processes, which are typically located in the cranial vault, and then merge into the vessels of the head. The blood then travels through the venous plexuses and flows into the TMO vessels.
Types of sinuses
Nature carefully created humans by equipping the dura mater with cavities to supply oxygen and nutrients to the main organ.
Superior sagittal sinus
This cranial cavity is characterized by a large space with a complex structure. The skullcap, the main human organ, makes an important contribution. It is a sickle-shaped leaf. It consists of a hard intracortical layer. The outgrowth arises at the tip of the cortical bone, runs medially backwards and embeds itself in the interhemispheric opening that separates the parts of the brain. The undulating process of the superior sagittal sinus is essentially the base of the sickle bone.
This canal has numerous lacunae on the sides. These are small cavities that are connected to the sagittal laminae via a venous network.
The superior sagittal tubercle has such venous connections:
- The anterior parts refer to the vessels of the labial cavity (near the nose);
- the medial parts refer to the venous canals of the parietal brain fragments.
This collecting system of arteries and veins becomes larger and more extensive as people age. Its posterior fragment projects into the united sinus tract.
Inferior sagittal sinus
This cistern of the cranial cavity is referred to in medical records as the inferior sagittal sinus, so called because it is located in the inferior position of the cerebellar arch. Compared to the upper reservoir, it has a much smaller volume. Due to the large number of venous connections, it is connected to the direct sinus.
Direct sine
This part of the cranial locus is basically the so-called extension of the inferior cistern on the posterior side. It connects the rear parts of the upper and lower cisterns. Together with the superior cistern, a large vessel is integrated into the anterior part of the nondual sinus. The posterior part of the cistern drains into the medial fragment of the double descending canal, formed by the divergence of the cranial TMO, located in the occipital hard tissue groove, extending laterally and connecting inferiorly to the sinus. This fragment is called the sinus tract.
Instructions for use for Bac-Set® Forte


Based on the officially approved instructions for the use of this medicine and prepared for Vidal's 2023.
Holder of the registration certificate:
| 1 capsule. | AUP*-VDUP** | |
| Probiotic complex (probiotic microorganisms and lactic acid) | 2×10 9 CFU | |
| Lactobacillus casei PXN37 | 5.8×10 8 CFU | 5×10 7 -5×10 9 CFU |
| Lactobacillus plantarum PXN47 | 3.2×10 8 CFU | 5×10 7 -5×10 9 CFU |
| Lactobacillus rhamnosus PXN54 | 3.2×10 8 CFU | 5×10 7 -5×10 9 CFU |
| Lactobacillus acidophilus PXN35 | 1×10 8 CFU | 5×10 7 -5×10 9 CFU |
| Lactobacillus bulgaricus PXN39 | 2×10 7 CFU | 5×10 7 -5×10 9 CFU |
| Lactobacillus helveticus PXN45 | 2×10 7 CFU | 5×10 7 -5×10 9 CFU |
| Lactobacillus salivarius PXN57 | 2×10 7 CFU | 5×10 7 -5×10 9 CFU |
| Lactobacillus fermentum PXN44 | 1×10 7 CFU | 5×10 7 -5×10 9 CFU |
| Bifidobacterium bifidum PXN23 | 1×10 8 CFU | 5×10 8 -5×10 10 COE |
| Bifidobacterium breve PXN25 | 1×10 8 CFU | 5×10 8 -5×10 10 CFU |
| Bifidobacterium longum PXN30 | 1×10 8 CFU | 5×10 8 -5×10 10 CFU |
| Bifidobacterium infantis PXN27 | 2×10 7 CFU | 5×10 8 -5×10 10 CFU |
| Lactococcus lactis ssp. lactis PXN63 | 4×10 7 CFU | 1×10 7 -1×10 9 CFU |
| Streptococcus thermophilus PXN66 | 4×10 7 CFU | 1×10 7 -1×10 9 CFU |
* Adequate intake per day
** Upper permissible intake per day.
ExcipientsMicrocrystalline cellulose, emulsifier (E460), hydroxypropylmethylcellulose, envelope (E464).
Contains no artificial colors, flavors or genetically modified organisms.
10 packs. – Blister packs (1) – Cardboard boxes.
10 pieces. – Blisters (2) – Cardboard boxes.
overdose
In general, overdose does not cause significant toxic effects, even when a high dose is taken. If a large dose of amoxicillin is taken, the patient will experience symptoms of gastrointestinal distress and water-electrolyte imbalance. In patients who suffer from. Renal insufficiencyIn the event of an overdose, the following symptoms may occur Nephrotoxicity i Crystalluria.
Treatment is symptomatic and may include taking medications prescribed by the doctor. In addition, the intake of Activated carbon. Hemodialysis may be performed. Hemodialysis. There is no specific antidote.
interactions
Wikipedia states that the drug has the effectiveness of oral contraceptives..
When taken at the same time as antibacterial antibiotics, one of the following occurs Synergy effectand, when taken concurrently with bacteriostatic antibiotics, antagonism antagonism.
The drug stimulates the indirect effect of anticoagulants, reduces the prothrombin index and vitamin K synthesis.
Reduces the effectiveness of drugs metabolized by PABA.
Duct secretion is reduced by Allopurinoldiuretics, probenecid, PhenylbutazoneNSAIDS. As a result, its concentration in the blood may increase.
Under the influence of Ascorbic acid The absorption of amoxicillin is increased, and when taken simultaneously with glucosamineAntacids, aminoglycosides, laxatives – reduced.
When taking amoxicillin and clavulanic acid at the same time – there is no change in the pharmacokinetics of these drugs.
Penicillinase-producing microorganisms show resistance to the main substance.
In combination with Metronidazole is actively against Helicobacter pylori..
There is cross-resistance between amoxicillin and Ampicillin.
Why do customers choose ortmann-pro insoles?







Reduces the feeling of fatigue, stiffness and pain in the foot. Suitable for almost all shoes with a maximum heel height of 4 cm.



How orthopedic technicians make ORTMANN-PRO insoles
During individual production, prefabricated insoles are produced in different sizes, shapes and degrees of hardness. The upper shell can be made of different materials, depending on the individual characteristics of the foot. The basis of the semi-finished product is a special thermoplastic material.

Ortmann Pro leather insoles from ₽9,590 ₽ The LEATHER PRO insoles, made from genuine leather, reliably and comfortably support the transverse and longitudinal arch of the foot and prevent the development and progression of flat feet.

Leather custom-made insoles Ortmann Pro from 6,990 ₽ LEATHER SHORT PRO leather custom-made insoles are designed for model, office and summer shoes with a heel of up to 6 cm. A special feature of LEATHER SHORT PRO is the genuine leather cover, which does not take up any space in the toe area of the shoe.

Ortmann Pro Individual Ultra Soft Leather Insoles from ₽ 9,990 ₽ LEATHER SOFT PRO Individual Ultra Soft Leather Insoles for Closed Shoes for Men and Women. The special feature of LEATHER SOFT PRO is a layer of polyurethane foam that effectively reduces discomfort, pain and burning in the forefoot area.

Ortmann Pro Custom Leather Kids insoles from 5,990 ₽ The special feature of Leather Soft Kids PRO is that the top of the insoles is made of vegetable-tanned, natural calf leather and underneath there is a soft polyurethane foam cushioning layer for additional comfort for the feet.
Read more:- Sursil Ortho made-to-measure insoles.
- The long section of the big toe.
- Custom insoles.
- Which ligaments strengthen the transverse arch of the foot?.
- Longitudinal and transverse arches of the foot.
- The Ligamentum Treitz, where it is located.
- Insoles for valgus in adults.
- Clubfoot insoles for adults.