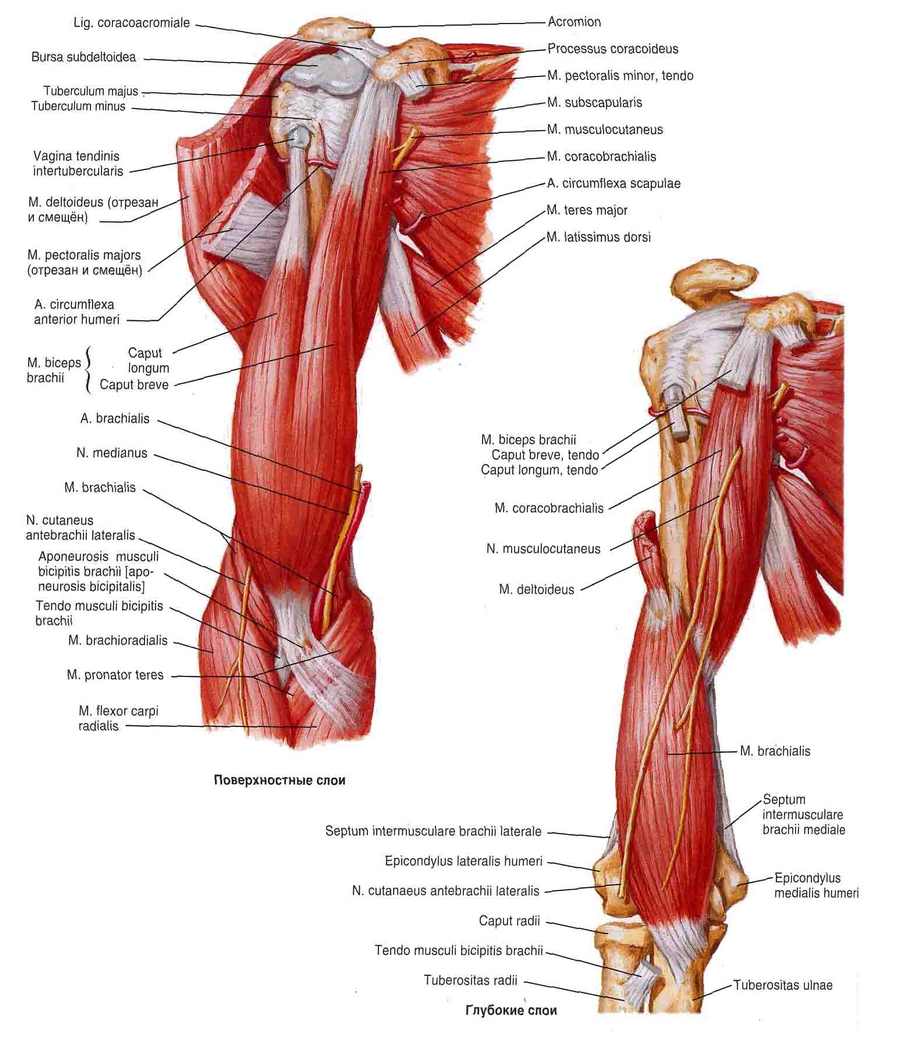
The peripheral pronator overlies the aponeurosis of the biceps and brachioradialis muscles.
At the same time, it partially overlays the radial flexor of the wrist.

- forearm muscles
- deep layer
- length
- Treatment
- circular pronator
- Introduction [edit| edit code ]
- Attachment[ edit ]
- Denervation [ edit edit source ].
- pronation of the forearm. Muscle function tests [ edit edit source ]
- Variations on exercises for the circular pronator.
- Fitness training for trainers.
- forearm muscles. Front group, deep layer
- FOREARM MUSCLES, FRONT GROUP:
- Treatment of median nerve neuropathy
- forearms
- superficial layer
- ribbons
- elbow joint
- muscles of the shoulder girdle
- muscles of the upper limbs
forearm muscles
M. pronator teres (M. pronator teres) (Fig. 111, 115, 116, 117, 125) provides for the pronation of the forearm (he rotates it forward and inward, so that the hand is backward (down) and the thumb inward rotates in the medial plane of the body) and participates in its flexion. Thick and short muscle composed of two heads. The large humeral head (Caput humerale) attaches to the medial epicondyle of the humerus and the intermuscular septum of the medial humeral fascia, the small ulnar head (Caput ulnare) to the processus coronarius of the tuberculum ulnare. The two heads join to form a flattened abdomen. The starting point is in the middle third of the radius bone.
Brachioradialis muscle (M. brachioradialis) (fig. 90, 111, 113, 114, 115, 116, 118, 121, 125) flexes the forearm and is involved in both pronation and supination of the forearm (he rotates it so that the hand forward (upward) and the thumb rotated outward relative to the medial plane of the body) of the radius bone. The muscle is fusiform, inserting at the humerus above the lateral epicondyle and at the intermuscular septum of the lateral fascia of the humerus, and inserting at the base of the body of the radius.
The radial flexor of the hand (M. flexor carpi radialis) (Figs. 90, 115, 121, 125) partially flexes and curves the hand. It is a long, flat, bifid muscle whose proximal part is covered by the aponeurosis of the biceps muscle of the arm. It arises from the medial epicondyle of the humerus and the fascia of the forearm, and its insertion is at the base of the palmar surface of the second metacarpal.
Palmaris longus (m. palmaris longus) (Fig. 115, 125) extends the palmar aponeurosis and is involved in the flexion of the hand.
This muscle is characterized by a short spindle-shaped abdomen and a long tendon. It inserts at the medial epicondyle of the humerus and the fascia of the forearm, inside the radial flexor of the wrist, and inserts at the palmar aponeurosis.
deep layer
Long flexor of the thumb (m. flexor pollicis longus) (Figs. 115, 116, 120) flexes the distal first phalanx (thumb). It is a long, flat, unicompartmental muscle that originates in the upper two-thirds of the anterior surface of the radial bone, the interosseous membrane (Figs. 117, 125) between the radial and ulnar bones and partially the medial epicondyle of the humerus. It starts at the base of the thumb end.
Deep flexors of the fingers (m. flexor digitorum profundus) (Fig. 116, 119, 120, 125) flexes the entire hand and distal phalanges of fingers II-V. It is characterized by a pronounced flat and wide inversion, the point of origin of which is located on the upper two-thirds of the anterior surface of the ulna and the intercondylar membrane. The point of attachment is at the base of the distal phalanges of fingers II-V.
Pronator quadrate (M. pronator quadratus) (Figs. 116, 117, 120, 121) internally rotates the forearm (pronation). This muscle is a thin sheet of quadriceps that lies at the distal ends of the forearm bones. It begins at the medial edge of the ulnar shaft and inserts at the lateral edge and anterior surface of the radius bone.
length
The average width of the muscle is 3.5 cm. [3]
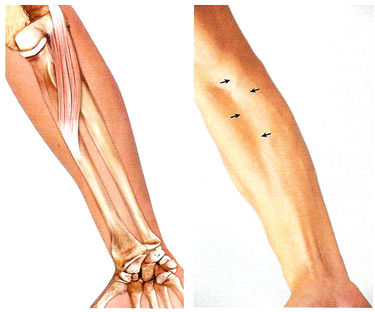
The muscle is neither palpable nor visible as it is the deepest muscle of the forearm. [2]
Muscular Trigger Points (MTT)
The pronator quadratus muscle has two main patterns of reflected MTT pain. Most often, the pain extends distally and proximally to the medial surface of the forearm. In many cases, the pain radiates proximally to the medial epicondyle and distally to the fifth finger. The pain also extends distally to the third and fourth fingers, which is a second common pattern. [7]
To treat pronator spasticity in patients after a stroke, neurolytic agents such as botulinum toxin, phenol or alcohol are injected into the motor point of the pronator quadratus muscle. [2]
Damage to the anterior intercostal nerve (AIN)
The electrophysiological diagnosis of PMN damage uses the pronator quadratus, the key muscle in this diagnostic procedure. [2]
Fracture of the distal part of the radius bone
The most common treatment for this fracture is fixation with a hand plate. A complication of this method is rupture of the flexor tendon, which is prevented by repair of the quadriceps pronator muscle during surgery.[8] Immobilization of the distal radius fracture with preservation of the quadriceps pronator muscle improves pronation, increases radial joint stability, promotes good healing, reduces pain, and thus improves wrist function in the early postoperative period.[9]
Treatment
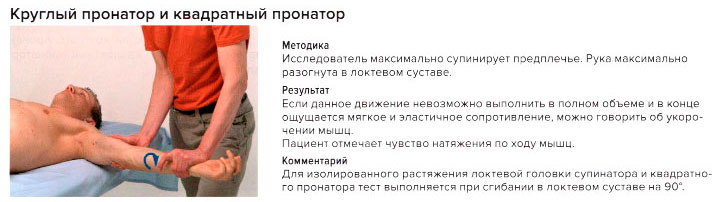
When the quadriceps pronator muscle is overworked, it sometimes resembles carpal tunnel syndrome carpal tunnel syndrome. Many musicians keep the forearm in pronation for long periods of time, which puts stress on this muscle. To stretch the quadratus pronator of the right hand, move the right hand (pinky) toward the sternum, ie, in a supinated position. With the other hand (left hand), press the right hand toward the abdomen to increase wrist flexion and press the right elbow forward to increase supination. Perform flexion and supination movements to stretch.
The muscle can be strengthened with an elastic band, elastic bars, ankle weights, or dumbbells. First, move the arm into supination and grasp the end of the rubber band, then move the forearm into pronation. Adjust the resistance according to the patient's condition.
circular pronator
circular pronator (m.propatotor teres) performs forearm pronation and is slightly involved in forearm flexion.
Introduction [edit| edit code ]
- head of the humerus.: medial epicondyle of the humerus, medial intermetatarsal septum.
- head of the humerusHumeral head : Proximal process of the ulna
Attachment[ edit ]
Denervation [ edit edit source ].
Pronation of the forearm (with the forearm flexed).
*M brachioradialis (from supination to mid-position).
*M flexor carpi radialis (when the forearm is not bent).
*M. extensor carpi radialis longus (when the forearm is flexed).
*M Brachioradialis (from pronation to middle position)
*M extensor carpi radialis longus (with a straight forearm)
pronation of the forearm. Muscle function tests [ edit edit source ]
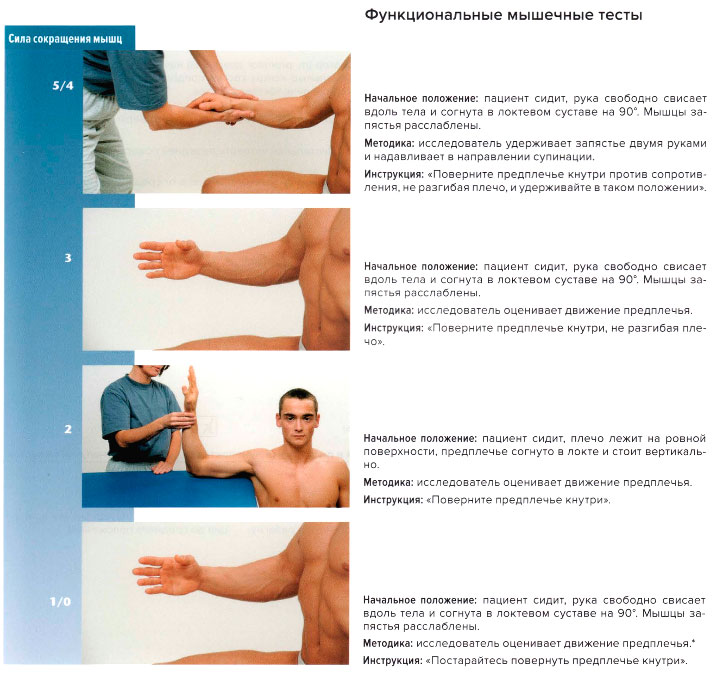
This muscle is deep and obscured by other muscles of the forearm and can only be evaluated when those muscles are paralyzed and atrophied.
Variations on exercises for the circular pronator.
The starting position is standing. The forearm is bent at the elbow joint. Take a rubber band attached at one end to wall bars or other sturdy support, perpendicular to your forearm and parallel to the floor. Then we turn the arm inward, as if wrapping the rubber band around the fist. The circular pronator performs a concentric contraction. Slowly return to the starting position. In this phase, the circular pronator works in an eccentric position.
A similar variation can be done with the block trainer. The starting position is standing. The forearm is strongly flexed at an angle of less than 90 degrees against the humerus. Ideally, the shoulder and elbow should be on a solid surface on the lateral side. For example on the backrest of a standing bench. Locking device on the top and on the side of the working arm. Hold the grip and rotate it evenly while simultaneously bending and pronating your wrist. When returning to the starting position, eccentric work is carried out.
Starting position: standing. The forearm is flexed at about 90 degrees or slightly less. The elbow can rest against the body. The wrist is gripped by a band or strong strap, at the end of which a moderate weight (pancake, dumbbell) is attached. The hand is directed upwards, ie in a supinated position. A penetrating motion is then performed with the hand so that the band wraps around the fist like a fist and the weight is lifted vertically upwards. The pronator is circular and again performs a concentric contraction. After returning under control, he works eccentrically.
The starting position is the forearm, with the entire elbow resting on a horizontal surface (pliobox, bench, table). A small weight can be used as a device by turning it upside down. This can also be a dumbbell with one-sided plates or a barbell. Grasp the handle of an inverted kettlebell, dumbbell, or body bar at one end and stand upright, leaning outward against your full fall. The hand is supinated and the circular pronator is forced to go through the eccentric phase. When the ball returns to its original (vertical) position, the circular pronator contracts concentrically.
This exercise can be performed in a more complicated version, if the device is moved to both sides. In this case, the pronators and supinators work sequentially and alternately
Fitness training for trainers.
For fitness trainers looking for courses that will increase their income, make them even cooler, and allow them to never have trouble getting a job, we recommend the following correspondence courses:
upgrade – Tailor-made topics and targeted income increase.
Fitness Instructor Course – For people who want to become a personal fitness trainer.
architecture of the body – Dmytro Gorkovsky's signature full-day practice and distance theory course for fitness trainers, massage therapists and physicians.
pregnancy – Exercise techniques for pregnant women and those recovering from childbirth.
pilates – Ekaterina Vasilenko's online course on the methods of the Pilates system.
forearm muscles. Front group, deep layer
In this article, we will delve further into the numerous muscles of the forearm. Myology is a branch of anatomy that deals with the structure and location of muscles in the human body. And in all myology there is no area more difficult than the forearm.
That's why I've broken down the muscles of the forearm into several articles - in the last article we looked at the superficial layer of the forearm muscles. In the last article we looked at the superficial layer of the forearm muscles, now we're going to look at the deep layer.
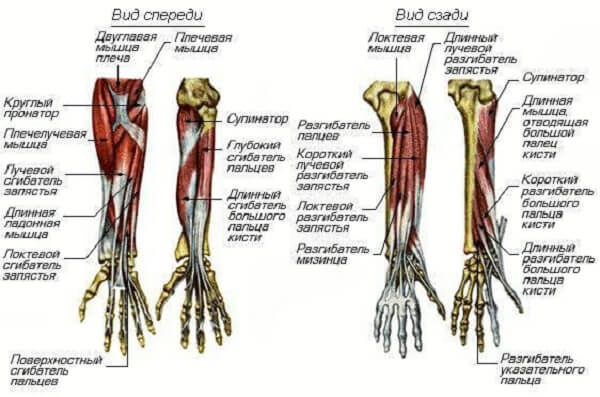
Now recall the physiological position of the forearm so we know where the front and back of the hand are. In this illustration, the hand is in its natural anatomical position, with the front of the hand in front of us. On this side are the muscles we are looking at.
FOREARM MUSCLES, FRONT GROUP:
1.long thumb flexor (Musculus flexor pollicis longus). It is the most lateral of all the muscles in the anterior group of deep muscles. Note the tendon - it is much shorter than the tendon of the similarly located superficial stratus muscle.
This muscle is also remarkable because its tendon runs close to the thumb.
Location: It inserts on the medial epicondyle of the humerus and on the 2/3 anterior surface of the radius bone; it attaches to the distal phalanx of the thumb of the hand;
Function: Flexion of the distal phalanx of the thumb. Here it is enough to know the starting point and the name to get an immediate idea of the function.
2. deep flexor of the thumb (Musculus flexor digitorum profundus). It can be seen that the entire deep muscle layer of the front surface of the forearm consists of two large muscles and one small muscle (see below). One of these two large muscles is the long flexor muscle of the thumb, which we described above. It is located on the lateral half of the forearm. The thumb flexor we are now considering occupies the medial half of the forearm.
Location: It begins on the front surface of the ulna and inserts into the distal phalanges of all the fingers of the hand except the thumb (it is flexed by the preceding muscle).
Function: Flexion of the distal phalanges of all fingers of the hand except the thumb.
3. the pronator quadratus (Musculus pronator quadratus). We've dissected the two large muscles that occupy nearly the entire anterior deep surface of the forearm. Now only the most unusual muscle of the whole layer remains, the pronator quadratus. Unlike the round pronator, which isn't particularly round, the square pronator is quite square.
Treatment of median nerve neuropathy
Depending on the origin of median nerve neuropathy, it is treated by specialists in neurology and related medical fields such as orthopedics and traumatology, endocrinology and surgery. In a first step, the etiological factor is eliminated: the hematoma is drained, the tumor is removed, the dislocation is corrected, the arthrosis is treated, endocrine disorders are corrected and the affected area of the nerve is spared.
In parallel, anti-inflammatory and analgesic treatment is carried out with NSAIDs (orthophen, nimesulide, tclafen, diclofenac) and, in more severe cases, with glucocorticoids (dipropane, prednisolone). If the pain is severe, the carpal tunnel is blocked - a combination of lidocaine and hydrocortisone is injected into the affected area of the nerve. Effective analgesics are phonophoresis with dimethoxyde and electrophoresis. Pharmacological agents that improve nerve nutrition are an important part of treatment: neurometabolites (vitamins B1 and B6, neostigmine, ipidacrine) and vascular agents (xanthinol nicotinate, nicotinic acid). In the recovery period, physical therapy, massage of the affected hand, electromyostimulation, mud treatment and ozokerite are used.
Median nerve neuropathy is an indication for surgical intervention when conservative treatment is ineffective, particularly when the nerve has been traumatically damaged. Depending on the case, nerve suturing, neurolysis with temporary implantation of an electrical stimulator, or nerve transplantation can be performed.
forearms
In order to develop the muscles of the forearm, it is best to first familiarize yourself with the anatomy of this part of the arm. It is important to know the superficial and deep muscles, which are strengthened with special exercises.
Functionally, the muscles of the forearm are divided into extensors and flexors. Some muscles are only responsible for the fingers, others for the whole hand. The radius is powered by the supinators and pronators, which are divided into two groups:
- The anterior group.The front group includes the pronators along with the flexors.
- The posterior group of forearm muscles (posterior group).The posterior group of forearm muscles consists of the supinators and the extensors.
Both groups have both a deep and a superficial layer.
superficial layer
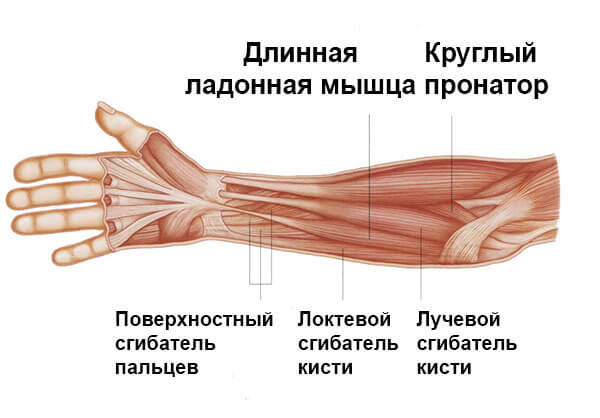
- The pronator ring Performs flexion and pronation of the forearm.
- wrist flexors Performs the flexion of the hand and its extension radially.
- Palmaris longus muscle (Palmus longus)Flexes the hand and stretches the aponeurosis.
- ulnar flexor of the wrist Leads and bends the hand.
- Superficial flexors of the fingers flexes the middle and proximal phalanges and activates the entire hand.
To understand exactly how the muscles of the forearm should be affected as part of training, it is necessary to pay attention to the deep layer.

- Long flexed thumbIt's important to understand which grip is most effective for the forearms. It's important to know which grip is more effective for forearm exercises on machines.
- Deep flexor Aids in flexing the middle and distal phalanxes of the second through fifth fingers, aiding hand movement.
- The square pronator Performs forearm pronation.
- Circular Pronator Performs assisted pronation.

Forearm exercises with dumbbells are a good option for men to develop strong arms and prevent shoulder disproportion that is common.
ribbons
Ligaments are connections of connective tissue, the strength of which is increased by the fact that the fibers that make them up are not parallel, but criss-crossed and inclined. Some bands, such as B. the pelvic thigh ligament and the longitudinal ligament, can withstand tensile loads of several hundred kilograms. (MF Ivanicki). Ligaments are made up of dense connective tissue rich in collagen fibers. Ligaments have a higher elastin content than tendons and are therefore more stretchable. Some ligaments are able to increase their length by 20-40 % when stretched, while tendons can only stretch 2-5 % (Shah et al., 1977).
The function of the ligaments is to strengthen the joints. They are not connected to muscles and therefore do not participate in muscle contraction. Therefore, ligaments cannot be inflated significantly. At the same time, the ligaments increase protein synthesis under the influence of growth hormone (GH). So if we train in a static mode, ie in a mode that promotes maximum GH secretion, we increase the concentration of growth hormone in the blood, and some of the hormone from the general blood flow will also be taken up by the ligamentous tissue. So the ligaments only need normal training without specialization to maintain their condition.
Constant stretching of the ligaments does not train them, but overstretches them. And this process is irreversible. Former athletes—swimmers, rhythmic gymnasts, and other sports that require athletes to be more flexible—often suffer from loose joints and vertebrae after their careers have ended. They have only two choices: undergo surgery to remove part of the ligament, or do strength training for the rest of their lives. Then the muscles take over the task of stabilizing the joints. But as soon as you stop exercising, the muscle tension relaxes and the joints start cracking again.
Wrestlers often have a habit of dislocating their shoulders. Some of them are even used to fixing it themselves. This is nothing but overstretching of the ligaments of the shoulder joint and can only be treated through surgery.
elbow joint
The elbow joint is a fairly strong joint. Stability is provided by the shape of the scapular joint, the annular ligament, the pull of the radial collateral ligament, and the fan-shaped ulnar collateral ligament. In all technical variants of arm wrestling, the main movement is pronation of the shoulder, which is performed in static mode. Therefore, during a fight, there is always a supination force acting on the joint, twisting the bones of the forearm out of the joint. One might think that the limiting role of the joint's medial ligaments should be paramount, but that's not quite the case.
First, the joint is significantly strengthened by the flexor muscles, both the forearm muscles, which attach to the medial epicondyle of the humerus, and the forearm flexors, which exert a force perpendicular to the applied force; however, the intense flexion tension balanced by the opposing partner force helps stabilize the joint and reduces stress on the ligaments in either direction of the applied force. This means that it is not the ligaments but the muscles and tendons, especially those of the forearm, that are primarily stressed.
Therefore, diseases and injuries of the medial ligaments of the forearm are extremely rare, while diseases and injuries of the tendons are much more common. An example is the well-known medial epicondylitis, golfer's elbow. This is an inflammation of the tendons that attach to the medial epicondyle of the humerus of the following muscles: pronator roundis, radial wrist flexor, ulnar wrist flexor, superficial finger flexor.
Which of these muscles do you know? They all play an important role in wrestling, and it is their tension that takes significant stress off the ligaments and cushions the impact on them. Secondly, the strength of the elbow joint is quite high and even if the muscle tension decreases, e.g. if the shoulder goes forward in a dangerous position in the frontal plane of the grip, there is no rupture of the ligaments, only a fracture of the humerus screw - the most common injury in arm wrestling. So, ligament strength is not a limiting factor, unlike tendon strength. Constant arm wrestling in an unsafe position during training does not lead to a fracture, but to overstretching the medial ligaments and subsequent destabilization of the joint, the consequences of which I have already written about.
muscles of the shoulder girdle
Let's look at the muscles that flex the shoulder at the elbow. In a fight, regardless of technique, you must, among other things maintain an optimal angle in the elbow.In addition to exercising lateral pressure during the attack. The effectiveness of this pressure is directly related to the strength of the arm muscles and the fighter's ability to apply it.
When wrestling 'overhead', the muscles of the shoulder girdle and the M. brachioradialis are particularly stressed. The biceps brachioradialis muscle is also involved to a minor degree. During pronation, the sphincter muscle is actively involved in flexing the shoulder joint.
When moving sideways, the strength of the lateral thrust primarily depends on the following factors. the stiffness and length of the collateral ligament (common flexor tendon - attachment point of all forearm flexors) and on the strength of the shoulder and thigh muscles.
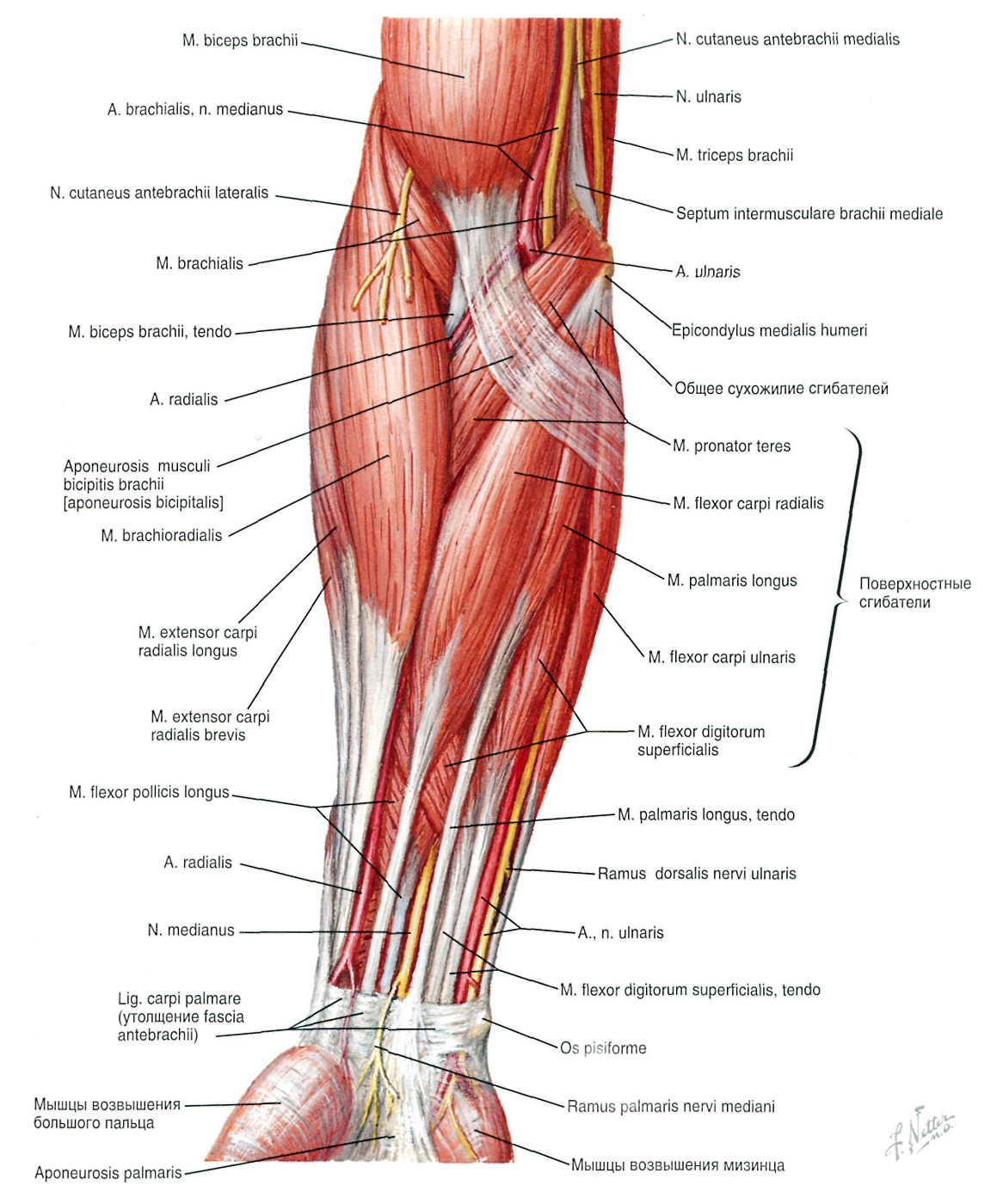
Figure 2.2 Muscles of the forearm (superficial layer): anterior view.
Hook fighting, regardless of the type of hook (lower, middle, upper), involves similar muscles: the delts and biceps. The collateral ligament is also heavily loaded. However, it depends on the type of hook which muscle is responsible for the success of the movement. For example, if a 'bottom hook' is used, the load is almost entirely on the. sideband..
muscles of the upper limbs
With correct technique, in addition to the muscles of the forearm and shoulder, the following muscles are also actively involved Peripheral muscles of the upper limbs. The involvement of these muscles is due to the athlete fixing the arm in a plane with the torso during wrestling. Wrestling takes place with the active participation of the deltoids, deltoids, pectorals, latissimus dorsi and other muscles of the upper limb border.

In wrestling, regardless of technique, the athlete can perform the following movements:
1. withdrawing upon oneself;
2. Lateral pressure at a constant angle on the elbow.
Figure 3.1 Muscles of the upper border of the limb
Of course, these movements cannot be separated from each other. Typically, the wrestler performs a combination of these moves.
Pulling puts a strain on you the broadest back muscles.. It also includes the posterior deltoid bundle, trapezius muscles, obturator major and minor, quadriceps, posterior obturator major and minor, and triceps.
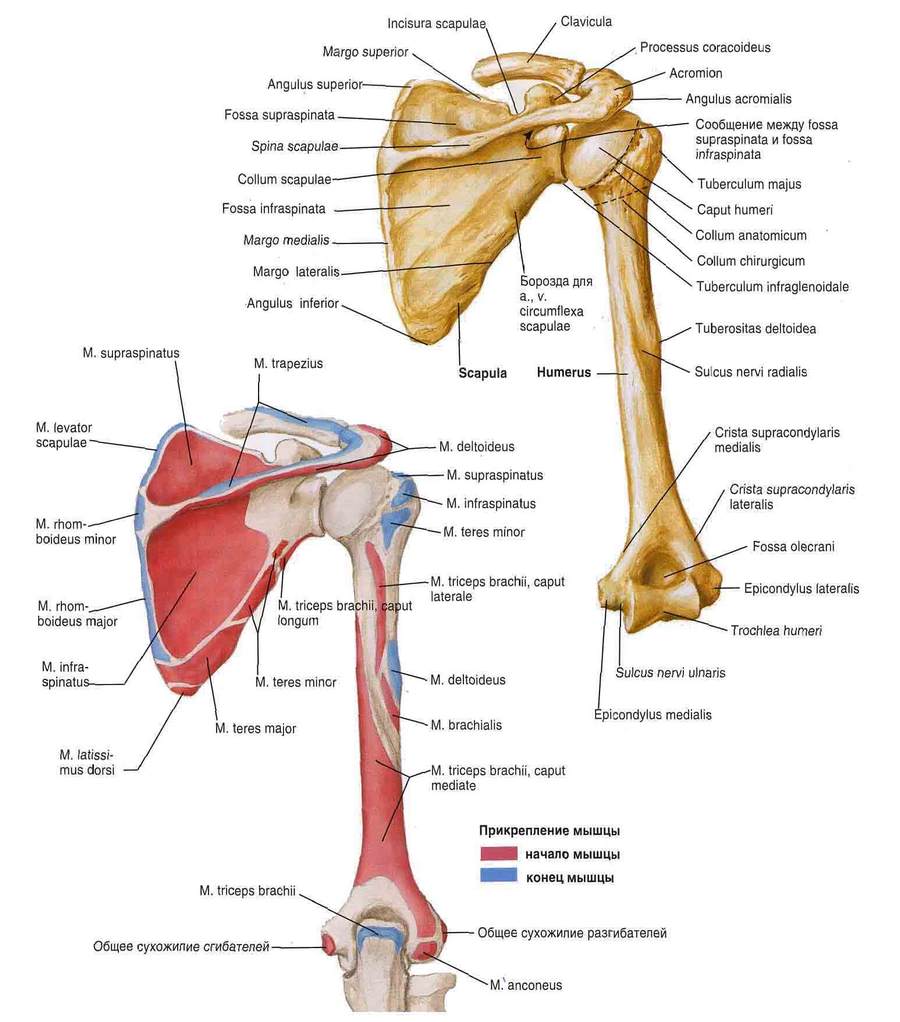
Figure 3.2 Origin and muscle insertions of the scapula and humerus: posterior view.
The side thrust engages the scapular, upper, and to a lesser extent the middle portion of the pectoralis major. The minor pectoralis, anterior deltoid, supraspinatus, scapularis, and piriformis muscles are also involved.
The video (1:34; 5:14) clearly shows how an athlete with a pectoralis muscle delay was unable to take advantage of his arm strength advantage.
Read more:- Pronator - what does that mean?.
- pronator and supinator muscles.
- These are the pronator muscles.
- pronator to.
- The long section of the big toe.
- The pronator muscle - what it means.
- pronation and supination.
- Square soleus muscle.