When Archimedes of Syracuse said: 'Give it a fulcrum and it will turn the earth', he obviously had the Yaroslav orthopedist Maxim Vavilov in mind. He studied the musculoskeletal system and did so at Archimedean speed. Give me 65 doctors, says Vavilov, and I will completely get rid of clubfoot in our country. The fact is that Maxim Alexandrovich was the first in Russia to treat clubfoot using the Ponseti method. This treatment was developed by the famous American orthopedist Ignacio Ponseti in the 1950s. The gist of this is that a serious congenital defect can be treated without major surgery and in just two months, instead of wearing grueling casts for a year. Vavilov managed to catch old Ponseti alive, and he personally learned from the master how to search for bases and rotate the planetarium of the feet. Today, the energetic orthopedist and trauma surgeon from the Constanta Clinic in Yaroslavl is obsessed with finding as many like-minded people as possible and passing on the knowledge of how to get humanity back on its feet.

- Clubfoot treatment according to the Ponseti method
- Causes of Clubfoot
- Causes of anomalies
- What symptoms indicate a problem?
- Invisalign knot in the center of the sole
- Treat the leg, not the diagnosis
- About the rigidity of Russia
- About the danger of ideas
- The Ponseti method compared to known treatment methods
- Ponseti on YouTube
- The Ponseti method
- Important features of the Ponseti method
- overview
- Treatment of clubfoot
- The Ponseti method for the non-surgical treatment of clubfoot
- Clubfoot Surgery
- Braces for clubfoot in children
- plaster technique
- Correction of the deformity with plaster casts
- prognosis of treatment
- Master class on the Ponseti plaster technique in clubfoot treatment by the President of the Russian Association, orthopedic traumatologist Dr. Maxim Alexandrovich Vavilov
Clubfoot treatment according to the Ponseti method
Congenital clubfoot is a developmental anomaly of the musculoskeletal system in which the inner edge of the sole of the foot is arched up and excessively inward, and the toes are turned inward.
To make an appointment for a consultation with an orthopedist, simply make an online request.
Clubfoot is a serious condition that causes the feet to deviate from their normal position. The disease is associated with restricted mobility and severe pain in the hip and knee joints. Clubfoot Ponseti treatment can help relieve symptoms. For more information about orthopedics and other services, see Traumatology and Orthopedics.
Causes of Clubfoot
The main cause of the disease is a genetic predisposition. If a parent has a relative with this disease, the risk that the child will develop the disease increases several times. In addition, the following factors contribute to the development of clubfoot:
- compression of the muscles of the uterus or the presence of tumors in the uterus;
- Abnormal function of the spinal cord
- pressure of amniotic fluid;
- skeletal malformations during prenatal development;
- Development of toxoplasmosis and other infectious diseases in women during the first trimester of pregnancy.
Obstetric diseases can be caused by avitaminosis in the expectant mother. A woman should monitor her body during pregnancy and regularly take vitamin and mineral supplements. Constant stress during the first three months of pregnancy should also be avoided, as this can also cause birth defects in the foetus.
Causes of anomalies
- Genetic – the appearance of abnormalities due to the maturation of organs.
- Mechanical – abnormal positioning of the fetus in the uterus.
- There are also muscular, neuromuscular, and a number of other theories about how the disorder develops.
Today, more and more experts consider the congenital malformation to be a manifestation of a pronounced dysplastic process (involvement of the intrauterine organs) of the whole body, in which the nervous, muscular, vascular and skeletal systems of the lower limbs are equally affected.
What symptoms indicate a problem?
Clubfoot at birth manifests itself externally as a foot deformity. It is not painful, but as it grows, it can cause significant discomfort and limit walking. It does not go away on its own (without treatment). The deformation will only increase, and the child's ability to walk will be severely affected. Symptoms increase as the child gets older. As a result, the child cannot walk, run, play sports, play, etc. Serious problems arise when choosing footwear.
Almost two and a half thousand years ago, Hippocrates attempted to treat children using manual manipulation and splinting. In the 19th century, the use of plaster casts to immobilize the feet was introduced. Today there are many different conservative and surgical methods, but the 'gold standard' is the Ponseti method, developed in the 1950's by Dr. Ignacio Ponseti was proposed. The specialists of our center have a lot of experience with this method and have successfully treated more than a dozen patients.
Invisalign knot in the center of the sole
While we are changing, little Soroka has already fallen asleep on the operating table. There we don't even see the sleeping girl, but her foot: the rest is covered by green disposable diapers. A pressure bandage was placed on the girl's thigh to stop the flow of blood. Vavilov rubs the leg with a large tampon soaked in iodine. The leg turns yellow. The doctor wraps the leg from toes to the knee with an elastic bandage and holds it upright for a minute to bleed completely. After unpacking it, he puts it on the table. The yellowish leg now looks like a silicone trainer.
With the first tiny incision above the heel, the doctor literally cuts through the Achilles tendon in seconds to lengthen it. This microsurgical intervention, the achillotomy, is not very spectacular. For many children with clubfoot, it is performed under local anesthetic in front of the parents.
The doctor then makes two similar bloodless incisions - a longer one along the tip of the foot. He takes a needle with a thick blue thread and begins to literally re-sew the tendons that look like a white braid. As in the rabbit pictures by Dr. ajbolite. He picks up the tendon thread with a needle in an incision and fixes it there with a few stitches, just like you learn in childbirth classes at school. He then pulls the braid under the skin to the second incision and pulls it outward. The foot follows the strand and is immediately correct: at right angles to the shin. The doctor sews up this tendon in its new position. He then pierces the foot with a needle and ties a nasty knot in the middle of the sole with thread. This takes no more than 15 minutes. The incisions are then sewn up with an absorbable thread and the foot is put in plaster for a few months. It's a routine procedure with an evocative name: transfer of the tendon of the distal tibialis anterior muscle to the third sphenoid bone of the left limb.
Treat the leg, not the diagnosis
In complicated cases, as in the case of the six-year-old ward 'Rusfund Polina Artemova. – are the only operations that cannot be performed. The girl was born in Taganrog with several leg abnormalities, including a clubfoot. She also has, for example, three toes on each foot. All this was discovered in the maternity ward.
– A clubfoot can be visible on the ultrasound as early as the twentieth week of pregnancy, says Vavilov. – In Russia, however, he is a surprise after birth in 90 % of cases. However, it is better for parents to know in advance what kind of problem they are going to face, find specialists and start treatment in the first month of life so that the legs develop properly.
Doctors offered Polina's parents to observe her for six months. But they took the girl to Moscow, where she was plastered using the Ponseti method. At the age of one and a half, the wide-eyed blonde with black eyebrows could already walk independently. She received braces, which she wore day and night until she was five years old. Then her left foot deformed, and not in the usual way, but due to a defect in the ankle. Also, that foot was shorter than her right foot. She had trouble walking. An orthopedic surgeon from the Filatov Hospital recommended her to see Vavilov.
– Ten years ago I treated valgus feet, and then I found out that different people come for valgus feet: with shin, knee and hip problems,' says Vavilov. – Now I prefer to treat the lower limbs – it is more effective. We can treat Polina in stages. For now, just straighten the clubfoot and send her home. In two or three months we can remove the spokes and let her walk for six months so she can go back to the hospital with a short, straight leg. And only then we use an Ilizarov machine to straighten the bone. But we want to do everything in a single anesthesia, so that in six to seven months Polina will be able to walk on her corrected leg with full support. We play with time. Or rather, we try to play with the times.
About the rigidity of Russia
In the beginning I had to fight with everyone here for the knowledge that was imparted to me. Of course I was young and had a lot of energy, but it wasn't easy. The doctors whispered, 'There goes the poncepter,' as if I had something terrible inside me. The system is difficult to break once established. You know, pediatric orthopedics is the most rigid specialty, you just can't change anything here. Fifty years before you, people treated and got seemingly good results. And then you show up and say you're the smartest. No one will believe it until the children you treat are at least five to ten years old. At medical conferences we often had direct arguments with colleagues. They said to me: Why did you bring us here, you Ponseti? We have treated here all our lives and nothing, thank goodness everyone is still alive. The arguments were: shut up and listen.
But time passed, the effects came, the supporters. People started talking about us, Rusfond started helping us, the point was not just to raise money for operations for parents, but actually to popularize the Ponseti method among professionals. And the children treated with this method have been going all over the country for ten years. And here we have the experience of observing them. So we can no longer say that clubfoot treatment abroad is better than here, but we can show what has been done here.
So we're gradually being recognized, there's already talk of a recognition award and so on. In the presentation of our clinic we have a map of Russia where about half of the country is shaded green - the Ponseti method is already practiced here. Now we still have to go to Kaliningrad, we haven't been to Sakhalin, Kamchatka, Yakutsk yet.
Maybe it won't go that fast - we manage to convince and train around ten specialists a year. But it seems that in Russia only some misfortunes happen quickly, while getting rid of them is a long and painful process.
About the danger of ideas
It seems to me that life without new ideas is boring. If you believe in your business, do it while you have the strength. But of course you always have a choice: either you fight for your ideas and sit at home alone, nibble dumplings and drink beer, or you have to live among people and somehow support your family. We had a man here, very good, very intelligent, we taught him, he went to Moscow. In the clinic they said to him: 'OK, we have some cattle, you can treat them, by the way, it's summer now, everyone is on vacation'. Over the summer he healed them all. In the fall the doctors came and asked, 'Where are the deer? He says they're all gone. Then they kicked him out. You fired him. Now he works as an adult traumatologist, but he can't touch childhood, not even with one foot.
You have to remember that and hold back. Or you have a stable family. I married a classmate at the time and now we have four children. It's such a whirlwind. Yesterday I came out of the operating room at 7.20 p.m., then I did homework with the children at home, then I fell down, then I got up at 6 a.m., went to school, to kindergarten and then came here. I guess I just don't have time to decide and hesitate.
The Ponseti method compared to known treatment methods
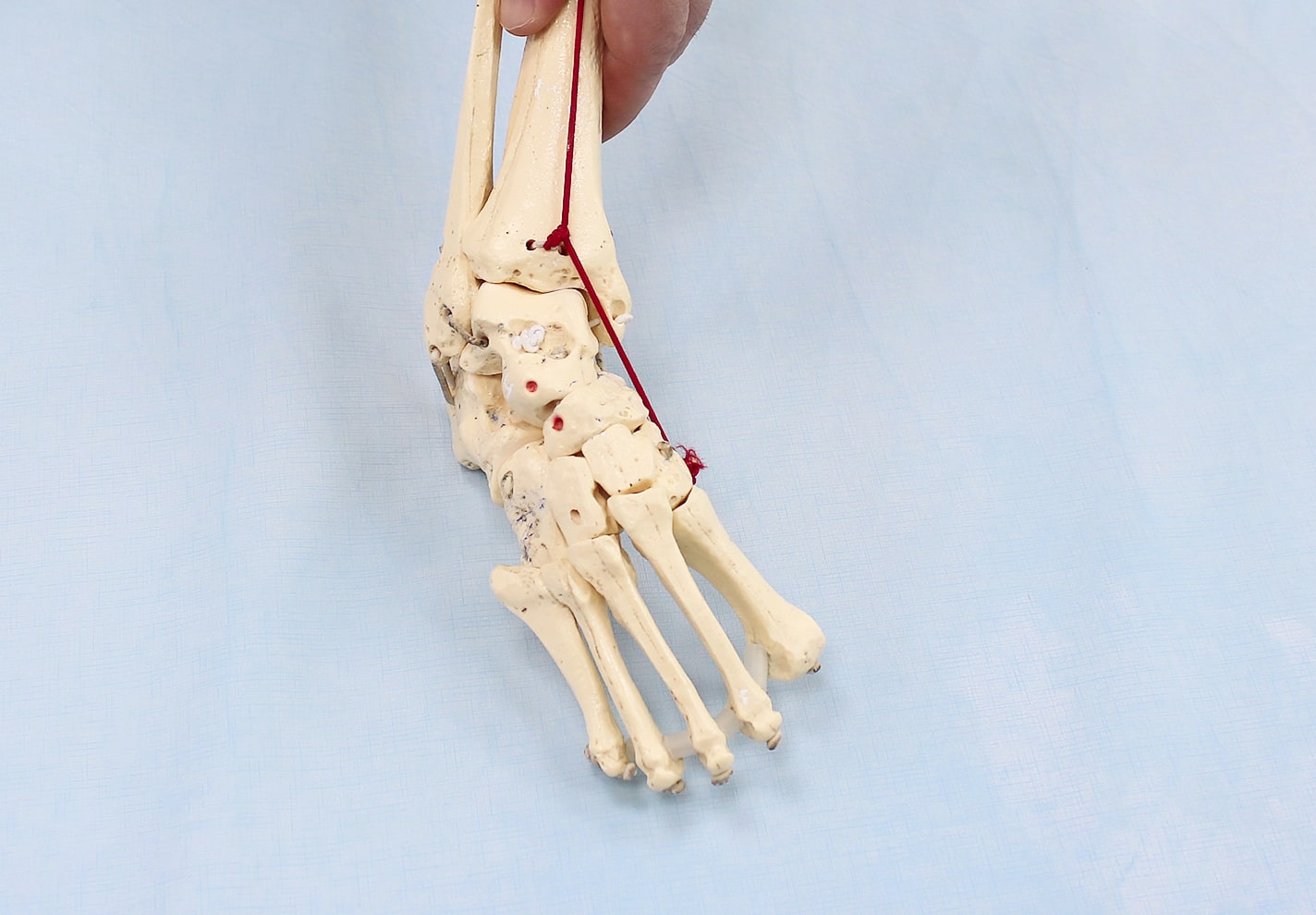
Plastic clubfoot model. The talus and heel bones are in plantar flexion. Heel, scaphoid, and cuboid bones are adducted and inverted. The tubercle of the scaphoid is located near the medial ankle. The tarsal bones are adducted. The first metatarsal is in maximum plantar flexion causing a cavus.
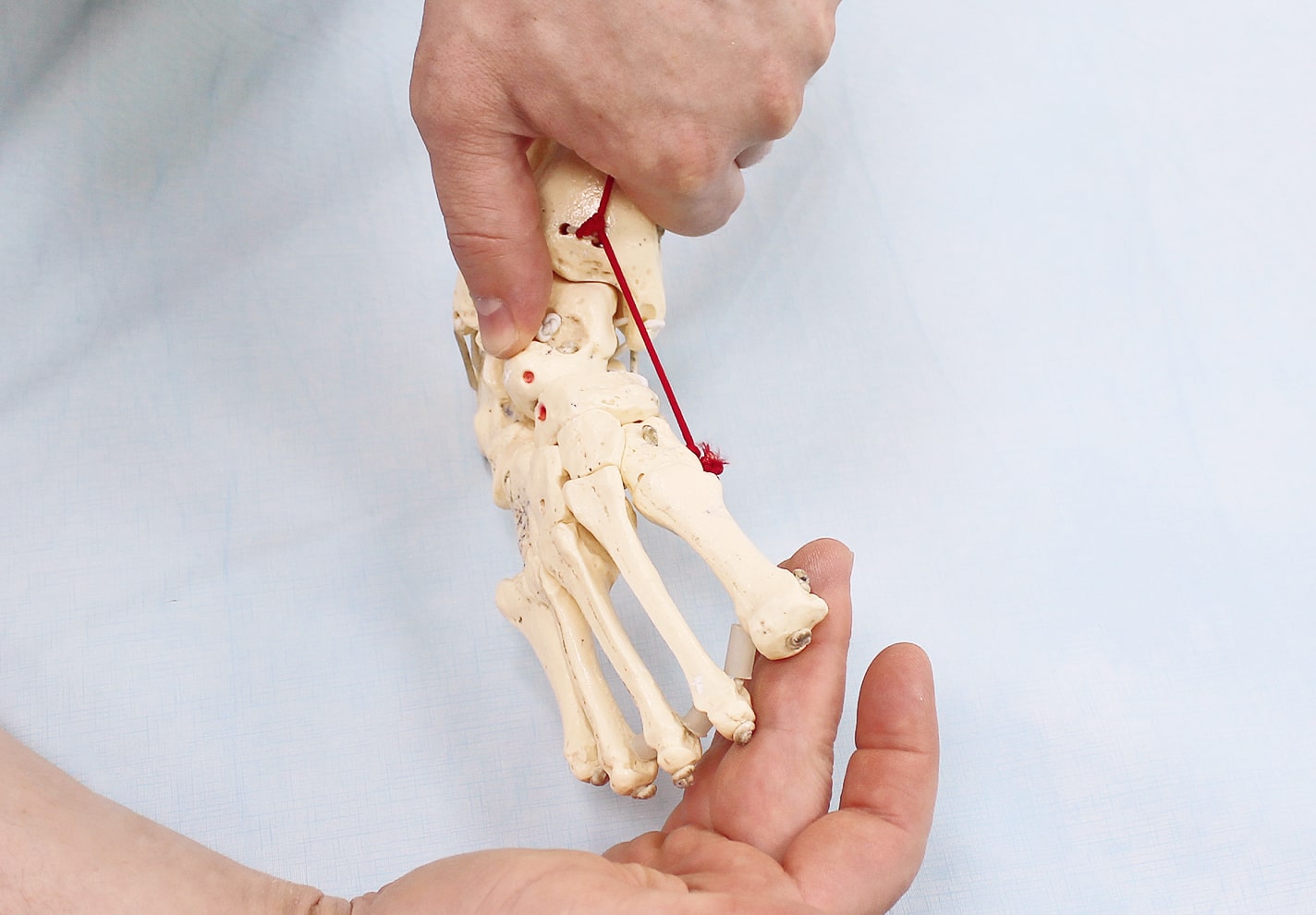
Correction of the cavus by dorsiflexion of the first metatarsal and supination of the forefoot.
Gradual abduction (5-10 degrees) of the supinated foot while applying pressure to the prominent head of the talus. Manual correction of the heel bone is not required.

Gradual abduction (5-10 degrees) of the supinated foot while applying pressure to the prominent head of the talus.
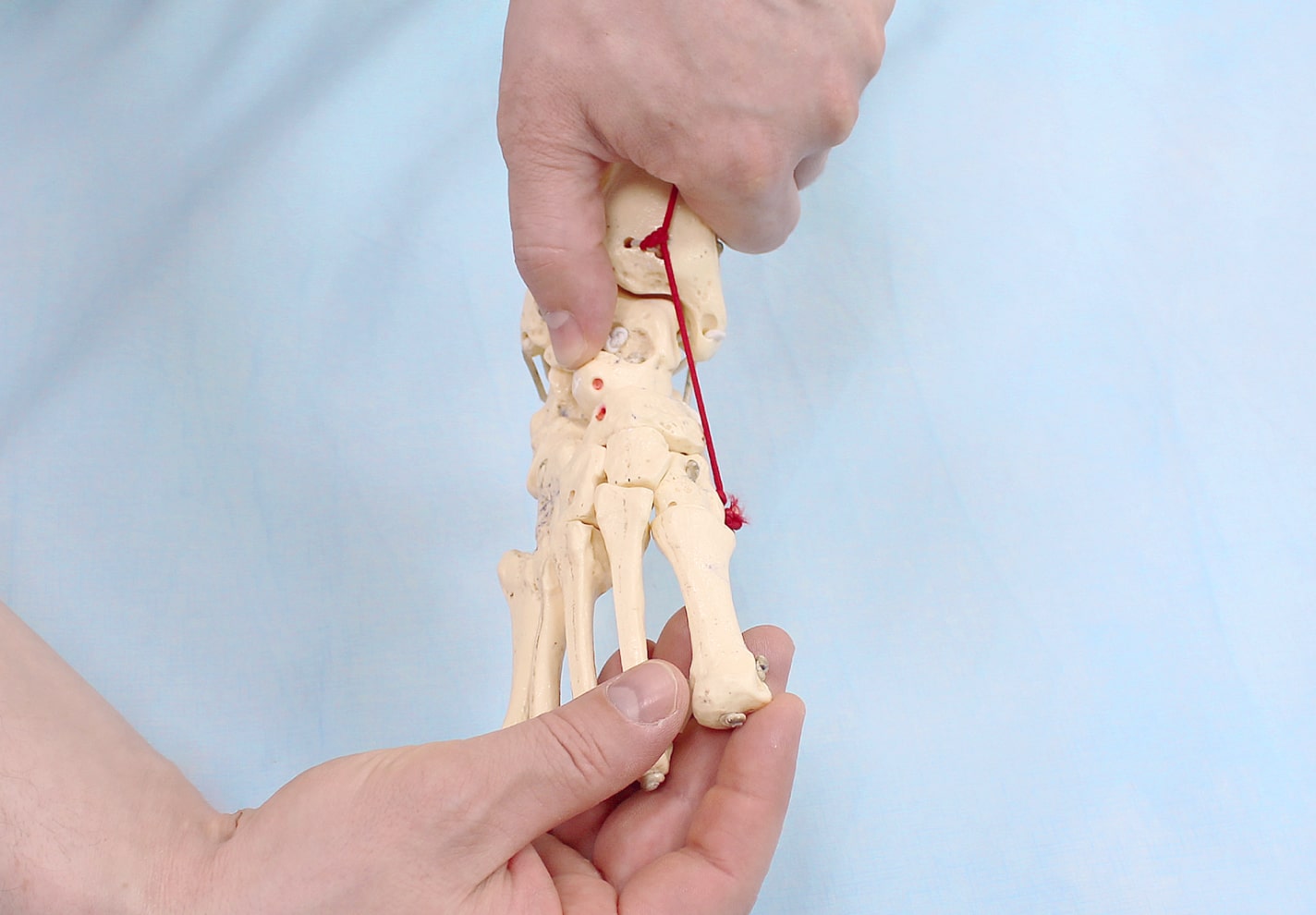
Gradual abduction (5-10 degrees) of the supinated foot while applying pressure to the prominent head of the heel bone.

With complete subluxation of the bones and the popliteal joints, the midfoot and forefoot must be retracted by 70°.
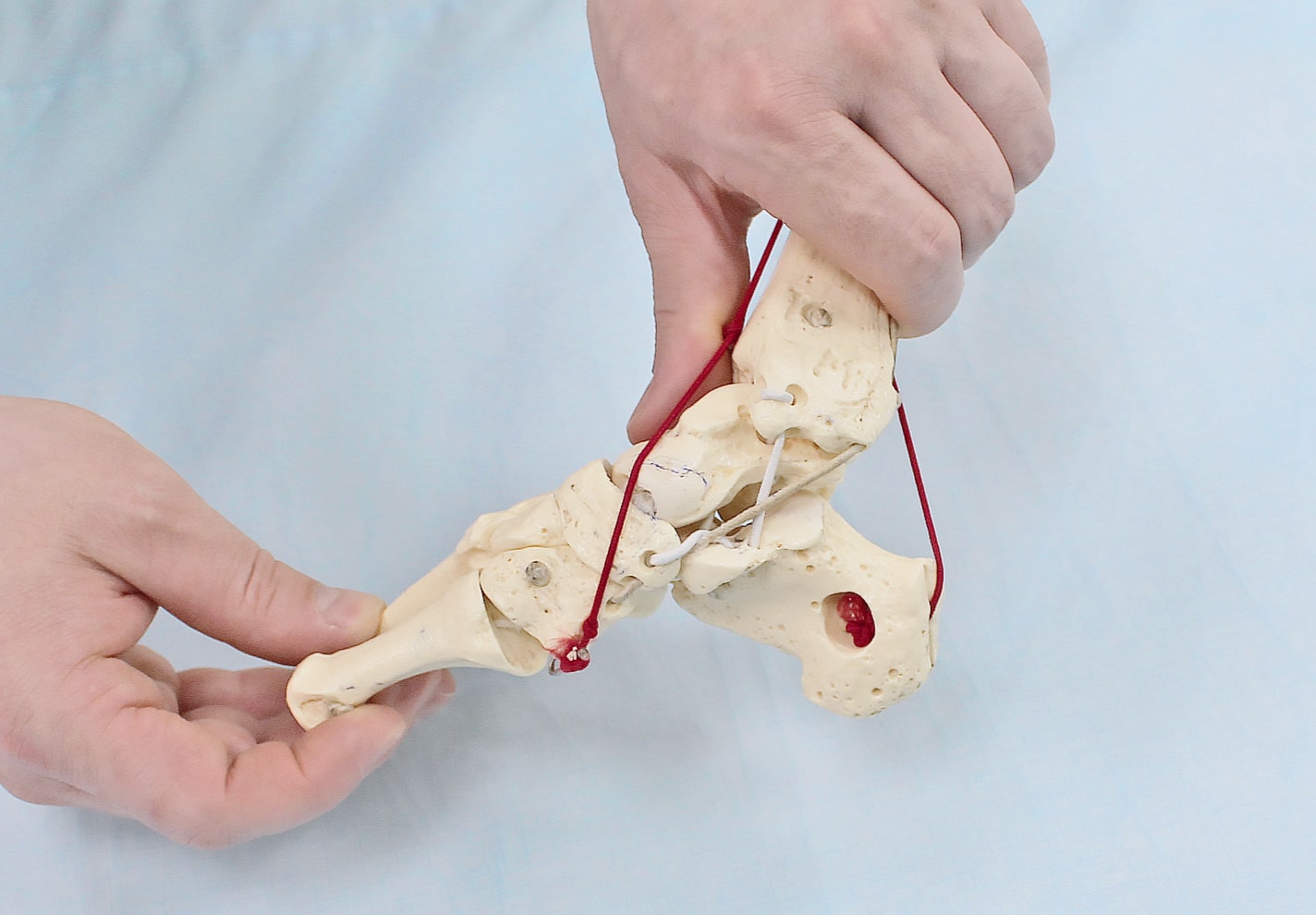
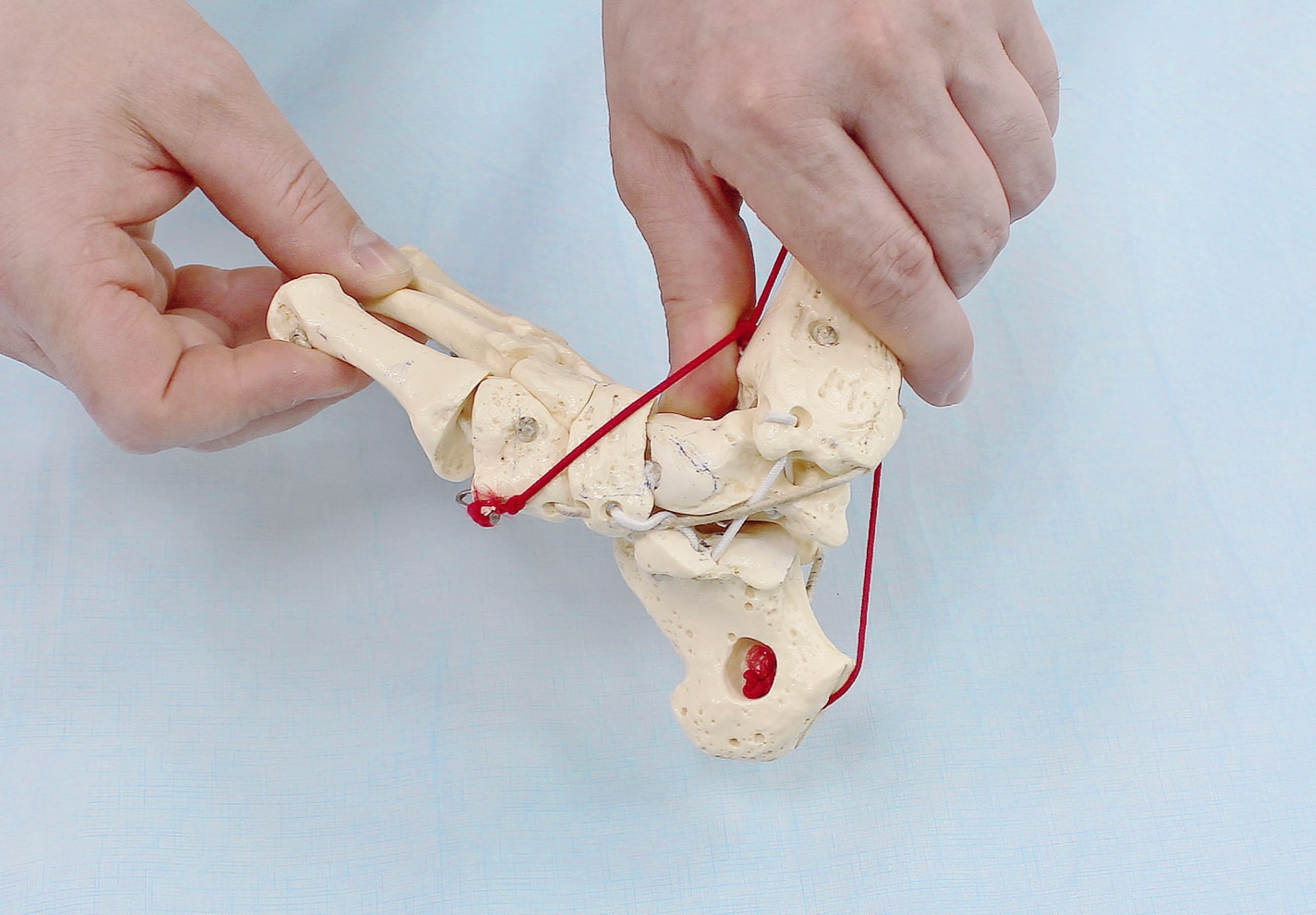

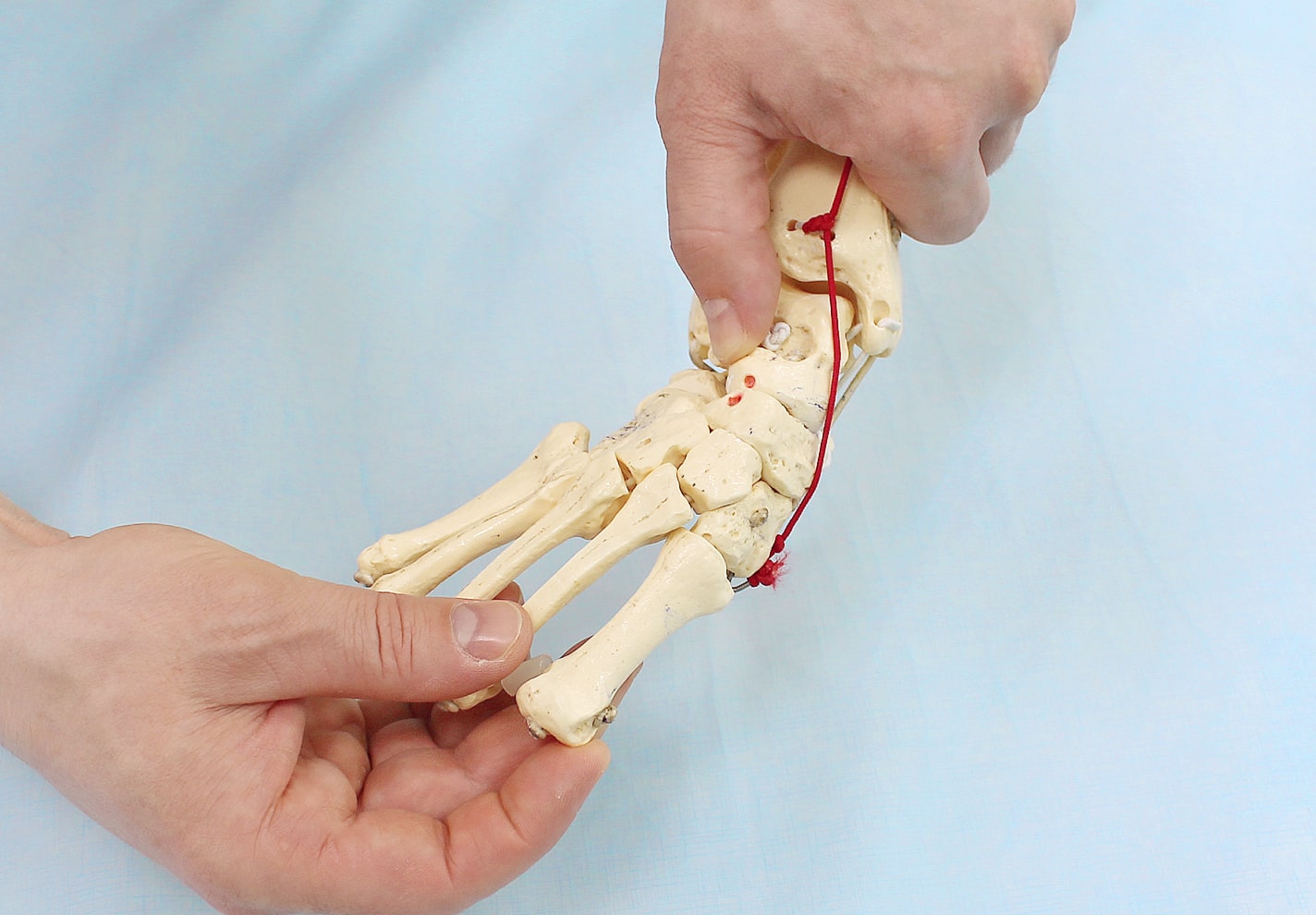
Posterior view of foot with valgus foot: varus of heel is evident, heel, scaphoid, and cuboid are adducted and inverted.
Ponseti on YouTube












The Ponseti method
This method of clubfoot correction takes into account the functional anatomy and the type of foot deformity. The correction takes place in several steps.
In the first phase, the deformity is corrected with plaster casts. About once a week, the foot is moved from the deformity to the normal side.
The degree of shift should not exceed 10-15 degrees. Even in the most severe cases, no more than 5-6 cast changes are required.
It is true that the first cast leaves the foot in normal plantar flexion and only corrects adduction and cavus (high arch).
In small children, the cavus is always mobile, so that supination is sufficient.
The second phase is called an achillotomy. Clubfoot is almost always accompanied by a shortened Achilles tendon that needs to be lengthened.
This method is usually a minimally traumatic, closed procedure in which the tendon is severed.
A cast is then applied again, this time a final cast. This must be worn for about a month. Overall, the cast is worn for a maximum of two months.
In the third and last phase of the Ponseti clubfoot correction, special splints, so-called brackets, are applied.
They help prevent the possible return of the deformity. The doctor creates an individual plan for the use of the splint, which must be strictly followed.
Even after the clubfoot diagnosis has been eliminated, the child should be examined annually by an orthopedist up to the age of five.
Important features of the Ponseti method
Clubfoot Ponseti treatment should be started as early as one week after birth.
If correction is not delayed more than 9 months, all clubfoot deformities can be corrected by the Ponseti method.
The maximum age at which a deformity can still be corrected is 28 months.
Most deformities are corrected within 6 weeks. If there is no change after this time, the treatment is considered wrong.
Late treatment can also be recommended according to the Ponseti method. She starts putting on plaster casts. Surgery is likely to be required afterwards, but usually on a smaller scale.
It is important to remember that clubfoot can be hereditary: if one parent has this musculoskeletal pathology, the child will suffer 4 % of the cases, but if two parents have it, the probability increases to 30 %.
In this way, the problem can be identified in good time. It is also possible to find out about joint problems. Knee arthroplasty - an important thing in orthopedics.
overview
Clubfoot is a congenital malformation of the foot and/or ankle. Early intervention can significantly correct the position and function of the foot.

In clubfoot, the infant's foot is turned down and inward. While this does not cause discomfort, without treatment it prevents normal walking and causes pain as the child gets older. Clubfoot is relatively common. Bilateral clubfeet account for about half of all cases.
The cause of clubfoot is unclear in most cases, but sometimes genetic changes that are inherited lead to deformities in the feet and other ankles. If a child in a family is born with clubfoot, there is a 1 in 35 chance that the other child will also have it. If a parent had clubfoot as a child, there is a 1 in 30 chance that the child will also have clubfoot. If both parents had clubfoot, the odds increase to about 1 in 3. Less commonly, clubfoot is caused by some serious diseases that affect a child's development, such as: B. Spina bifida – incomplete closure of the spinal canal.
Clubfoot is usually diagnosed soon after birth, but sometimes it can be detected with an ultrasound at 18 to 21 weeks. It's not possible to start treatment before birth, but early diagnosis gives doctors time to to discuss the condition in detail and discuss the next steps after the birth of the child. Additional tests for other diseases and abnormalities may be required during pregnancy.
Treatment of clubfoot
Treatment is best started in the first week or two after birth, but can be done later. There are now both non-surgical methods of treating clubfoot and methods of surgically correcting the shape of the foot.
The Ponseti method for the non-surgical treatment of clubfoot
The Ponseti method is the mainstay of clubfoot treatment as it is more effective and efficient compared to surgery.
With this method, the orthopedist slightly corrects the child's foot position by hand once a week. The foot is fixed in this position with a plaster cast. After a week, the procedure is repeated and the doctor corrects the position of the foot a little more. The cast is changed once a week, and each time the position of the foot approaches a little closer to normal. Usually 5-6 bandages are required, sometimes a little more or less depending on the severity of the clubfoot.
The procedure is painless and the doctor works very carefully. Children often cry during the procedure, but usually not because they are in pain.
Clubfoot Surgery
If the Ponseti Method has not completely corrected the alignment of the foot, the doctor may recommend minor surgery to cut the Achilles tendon (located above the heel). This happens when the forefoot has already been trained but the ankle is not yet in the correct position.
The procedure is performed under local anesthetic on an outpatient basis, ie an overnight stay in the hospital is not necessary. In some cases, the doctor may recommend general anesthesia, where the child sleeps during the procedure. The surgeon makes a small incision in the Achilles tendon so the foot can return to its natural position. The child's leg is then put in a cast for three weeks. In rare cases, the tendon at the front of the ankle needs to be re-operated after a few years to allow the leg to function better.
Braces for clubfoot in children
After the treatment, the child must wear a splint with a shoe attached. This fixes the feet in a slightly shoulder-width position. This serves to stabilize the treatment and prevent clubfoot recurrence.
plaster technique
The Ponseti plaster technique requires care and attention to the timing of fixation. During the rehabilitation period, a long-term orthosis is used to consolidate the results achieved. This treatment method is the standard of conservative treatment in Europe and the USA.
The effectiveness of treatment depends on the quality of cooperation between doctor and parents. Having a foot in a cast can be very uncomfortable, but if you allow yourself to feel that way, the child's condition can deteriorate to the point of disability. The orthopedist must maintain a clear schedule for treating dislocations and notify parents of any changes in the cast and orthotic regimen.
Correction of the deformity with plaster casts
At this stage, the foot deformity is corrected with plaster casts. Six to seven plaster casts are needed every five to seven days. The foot is brought out of the curve to a normal position. The angle of limb change is 10-15 degrees at 1 plaster cast. The cast should hold the knee joint in place and cover the upper third of the thigh.
The procedure is performed by the doctor and his assistant. The nurse holds the limb while the orthopedist applies the cast.
- The first cast corrects the cavus – the internal rotation of the forefoot. Dorsiflexion in the ankle is restricted.
- The second through fourth casts aim to correct the pronation of the foot and toes - the varus. In children in the first year of life, the cavus is characterized by flexibility and mobility. Supination—rotation of part of the limbs outward—of the forefoot to correct the longitudinal arch of the foot is required.
- Correction of the deformity is carried out. The talar head remains stationary and the foot is withdrawn. The position of the talus is then stabilized.
- Four to five plaster casts are sufficient to correct the deformity of the foot. If the foot is difficult to correct, the number of treatments must be increased.
- There is an improvement with each cast change episode. However, complete normalization of the cavus, rotation of the foot to a physiological position, varus and partial correction of the equinus are not enough. In rare cases of excessive tendon elasticity, correction of the equinus with a cast is possible. In the second stage, surgical correction or an achillotomy is performed.
prognosis of treatment
Recurrences occur in 1 to 2 out of 10 patients, which can be traced back to non-compliance with orthotic wearing or cast regimen. After treatment with the Ponseti method, in 90% of the cases the child can walk at a normal pace and later play sports like other children.
After treatment, unilateral clubfoot may have one foot slightly smaller than the other. This does not affect the child's movement, but the child may tire more quickly than other children of the same age.
dr EO Komarovsky does not comment on this method of treating clubfoot. The orthopedist should deal with the congenital pathology, and the pediatrician should help parents find a clinic that works according to the Ponseti method.
In different countries there are orthopedic societies that should provide a list of doctors and medical institutions upon request of the pediatrician or parents.
Clubfoot correction is a long, gradual, daily job for the child, family and doctors. How well everyone is doing depends on whether the child can walk and become a full member of society.

The plaster cast begins at the age of two weeks with the correction of the hollow foot (cavus). Thereafter, valgus, inversion and adduction are corrected simultaneously since the tarsal joints are closely related and can only be corrected together, with the foot rotating around the head of the heel bone. Varus (supination) and adduction (forefoot adduction) are usually corrected after 5-6 casts.

Master class on the Ponseti plaster technique in clubfoot treatment by the President of the Russian Association, orthopedic traumatologist Dr. Maxim Alexandrovich Vavilov

Once the cast is in place, the child must wear an orthosis that allows 75 degrees of rotation for the corrected foot and 45 degrees for the healthy foot. The orthosis is a splint with a shoe attached to it, which is positioned shoulder-width apart and at the head angle mentioned above. The splint is an essential part of clubfoot treatment and the way the splint is worn is important. In the first three months after putting on the cast, the child has to wear the splint 23 hours a day, after that the time decreases to 14-16 hours a day, and then only for nighttime sleep. The orthosis must be worn until the child is 3-4 years old, even up to 5 years according to some sources. The main purpose of the orthotics is to stretch the muscles and prevent them from reoccurring. According to Ponseti's Clubfoot article, only 6 % of children whose parents wear a splint relapse.

The method is used in America, Europe and Asia.
The first doctor in Russia to use the Ponseti method since 2002 is Guram Mikhailovich Khochiev from the Vladimir Regional Hospital.
The second practitioner using the Ponseti method in Russia is Maxim Alexandrovich Vavilov, who works at the Yaroslavl Children's Hospital. He was trained in America and has been practicing the method since fall 2006.
Today Maxim is one of the leading specialists in this field of medicine.
There are now many orthopedic podiatrists operating in all parts of Russia. For a non-exhaustive list, see the Contacts of Russian Podiatrists section.
If you can't find one in your area, please give us a call. We will do our best to find the nearest qualified doctor.
Read more:- Ponseti breeches.
- 1 year old child with clubfoot.
- Congenital clubfoot.
- Clubfoot in 7-year-old children.
- clubfoot.
- What is clubfoot?.
- Clubfoot in children therapeutic exercises 7 years old.
- baby splashing.