A high load on the shoulder can lead to various types of damage and degenerative changes. Repeated stress on the shoulder joint can lead to loss of stability and dysfunction. A more serious problem is a partial or complete tear of the rotator cuff at this joint. Such an injury requires urgent medical attention, and often surgical treatment.

Brief anatomy of the hemorrhoids

Hemorrhoids – is a condition associated with a range of symptoms caused by abnormal enlargement of the hemorrhoids. The main components of this symptomatic syndrome are:
- intermittent bleeding from the anus;
- prolapse of hemorrhoids outside the anal canal;
- frequent inflammation of the hemorrhoids.
Hemorrhoids are one of the most common human diseases and the most common coloproctological disease in western civilization. About 140 people per 1,000 adults will experience some form of symptoms associated with abnormally enlarged hemorrhoids. It has been found that 70 % of people over 30 years of age who see a coloproctologist have symptoms of hemorrhoids, with men and women having the same incidence of the mentioned symptoms. In the structure of coloproctological diseases, hemorrhoids account for about 40 %.
Structure of the anal canal
The anal canal is considered to be an extremely complex anatomical structure. It is one of the few boundary structures in the human body that is made up of all three embryonic layers: endoderm, mesoderm and ectoderm. Its formation occurs between the 5th and 8th week of intrauterine development. This complex process consists of the following phases:
- Formation of the anal fossa by the dipping of the ectoderm towards the posterior segment of the intestine;
- deepening of the anal fossa towards the terminal segment of the posterior intestine;
- Formation of the anal membrane as the transition between the anal canal and the posterior segment of the intestine (followed by the dentate line);
- Perforation of the anal membrane leading to a connection between the rectum and the anal canal.
It is important to distinguish between the 'anatomical' and 'surgical' anal canal (Table 1).
Table 1: Features of the anatomical and surgical anal canal
| characteristics | Anatomical anal canal | Surgical anal canal |
| upper edge | tooth line | Anorectal ring |
| bottom edge | Linea anocutanea | Linea anocutanea |
| length | 1.5 - 3.0 cm | 2.0 - 5.0 cm |
The anatomical anal canal runs from the dentate line (linea dentata), also known as the scale line (linea pectinea), to the outer anal edge, the Hilton line (linea anocutanea, linea alba). The latter is located where the anoderm meets the perianal skin and is characteristically pale in color.
The surgical anal canal is located between the top edge of the muscular anorectal ring and the outer edge of the anus.
description of the disease
shoulder rotator cuff – The front, outer part of the shoulder joint capsule. Includes the supraspinatus tendons, subscapularis tendon, and sphincter minor. Despite their different functions, this anatomically close attachment point has allowed traumatologists to distinguish these muscles in a common group (the rotator cuff of the shoulder).
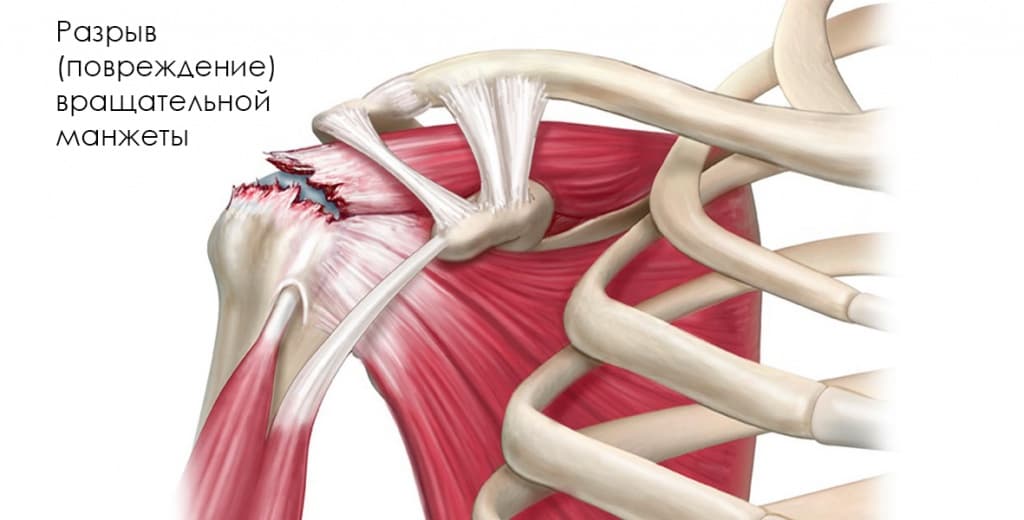
A tear in one or more of the tendons that make up the rotator cuff may be referred to as a rotator cuff injury. It is most often caused by trauma, dislocation, or previous chronic inflammation.
What are the causes of a rotator cuff injury in the shoulder joint?
As previously mentioned, the most common cause of rotator cuff injuries is trauma. Tears are most common in older people, but young people can also suffer a tear as a result of a serious injury, such as a fracture of part of the humerus or a dislocation.
- A common cause of rotator cuff injuries are Permanent tendon injury.A common cause of rotator cuff injuries is permanent tendon injuries that are chronic in nature. This is especially true for people in physically demanding jobs. The stress and strain on joints that accompanies repetitive physical activity leads to chronic inflammation and pain.
- A spontaneous tear or damage to tendons is usually preceded by the following, among others. a period of degenerative and dystrophic changes. Lack of blood supply is the main cause of tissue degeneration or tendinopathy. Another possible cause of degeneration is genetic predisposition.
- Another possible cause is. individual anatomy. Insufficient clearance between the humeral head and the top of the scapula can sometimes lead to rubbing and rotator cuff tendon injuries. In addition, there is the anatomically determined hook-like shape of the acromion and the presence of an additional bone at the tip of the shoulder blade, which damages the tendons.
What is happening inside during this time?
The diaphragm (Figure 1) is the muscle that separates the thoracic cavity from the abdominal cavity. Its main function is inhalation. When you breathe in, the diaphragm contracts and moves down, creating an area of low pressure in the chest cavity and higher pressure in the abdominal cavity. As we all know, any body has a tendency to move from an area of higher pressure to an area of lower pressure. Therefore, the stomach tends to move up through the esophageal opening of the diaphragm with each inhalation. This is prevented by the size of the esophageal opening itself.
A few words about the structure of the diaphragm itself: a flat, thin, dome-shaped muscle. The diaphragm has three openings through which pass the aorta, inferior vena cava, and esophagus. The esophagus runs through the tendon layer of the diaphragm.
When the diaphragm contracts, the muscle fibers that contract stretch the opening of the esophagus, which is near the center of the dome.
Since the opening is now stretched, the stomach pushes under the pressure of the abdomen into the upper part of the chest cavity (Figure 2). The sphincter (valve) that closes the entrance to the stomach can no longer function properly. The stomach no longer closes tightly enough, so that the stomach contents are thrown under pressure into the esophagus. The lining of the esophagus is not adapted to withstand aggressive substances such as stomach acid, which causes a burning sensation and eventually ulcers in the esophagus.
In addition, the secretory function of the stomach and its mobility are impaired. Due to the disturbed motility, the passage of digested food into the intestine is impaired. This leads to a feeling of heaviness and congestion in the stomach (even with a small amount of food ingested). All this leads to impaired breakdown of proteins.
At the level of the esophagus there are ligaments with muscle fibers (Ligamentum Treitz). This ligament holds the duodenum away from the diaphragm. Irregular contraction of the diaphragm changes the shape of the esophageal opening and irritates this ligament. At the same time, both the duodenum and jejunum become irritated and constricted, making it difficult for food to pass through the duodenal-small bowel junction. Digestion of food in the small intestine is impaired due to impaired flow of small intestine and pancreatic enzymes, as well as bile from the gallbladder. This impairs the absorption of unsaturated fatty acids, which are important for building cell membranes, and of carbohydrates. Allergies to natural foods, dysbiosis
Causes of Diaphragm Spasms:
One of the main causes is a disturbance of the innervation. The diaphragm muscle is innervated from the cervical spine by the phrenic nerves. Compression of the cervical spine or dislocation of the vertebrae results in pinching of the phrenic nerve on one side or the other, resulting in dysfunction of the left or right side of the dome.
The next equally important and common cause is stress. Modern people in particular are exposed to stress almost every day. Our body reacts to a stressful situation primarily with breathing. The nervous system sends out confusing signals that cause the diaphragm muscle to contract.
Read more:- The pubic ligament where it is located Photo.
- Transverse arch of the foot Latin.
- shoulder supinators.
- The hock in which the person is located.
- The hock in which the person is located.
- The bone where the ankle is located.
- How much does shoulder surgery cost?.
- Injury to the navicular semilunar ligament.