The Achilles tendon, the largest ligament in the body, is important. It is attached to the heel bone and serves as a mechanical energy store when walking. This reduces the energy expenditure for locomotion by 20-30 %.

- Anatomy of the joints of the human foot – information:
- Which Doctors Should You See to Evaluate Ankles?
- The architecture of bones
- The bones of the fingers
- tarsus
- tarsus
- Joints and articular cartilage
- ankle
- Structure of the tarsal joints of the human foot
- Subtalar
- Wedge-shaped
- Special treatment
- Conservative technology
- Surgical technique
- costs of the services
- Injuries to the tarsus
- How can you prevent foot diseases?
- Cookie Settings
- Cookie Settings
- The bones of the foot
- Ligaments and muscles
- Diagnosis of dislocated feet
- Treatment of foot sprains
- Rehabilitation after a foot fracture
- Surgery for metatarsal fractures
- Percutaneous fixation with spokes
- Open repositioning of a fracture
- Rehabilitation after a metatarsal fracture
Anatomy of the joints of the human foot – information:
There are four joints in the joint between the tarsal bones, the articulationes intertarseae:
- The subtalar joint.The subtalar joint is formed by the posterior articular surfaces of the talus and calcaneus, which are generally cylindrical segments.
- Talcaneo-cavicular jointTalocalcaneonavicularis, lies anterior to the subtalar joint and consists of the almost spherical head of the talus bone, the associated socket formed by the navicular bone, the articular surface on the sustentaculum of the talus of the calcaneus and the ligament. The joint sac is reinforced by the ligament. calcaneonaviculare plantare, which fills the gap between the sustentaculum and the posterior edge of the navicular bone and contains in its thickness a layer of fibrocartilage, fibrocartilago navicularis. The joint sac is reinforced on the dorsal side by the talonavicular ligament and on the plantar side by the canacaneonaviculare plantare ligament. Between the two joints there is a bony canal, sinus tarsi, in which a strong ligament, ligament talocalcaneum interosseum, runs between the talus and the heel bone.
- Heel bone-cube joint (calcaneocuboid)The calcaneocuboid joint (calcaneocuboid) is formed by the opposing articular surfaces of the heel bone and the calcaneus. It is involved in the movement of the subtalar and patellofemoral joints by increasing their volume. The art. calcaneocuboidea, together with the adjacent art. talonaviculare, is also described under the common name of the transverse tarsal joint, art. tarsi transversa. In addition to the ligaments that separately reinforce the calcaneocuboid artery and the talonavicular artery, there is also a ligament common to both joints in the transverse joint and which is of great practical importance. This ligament bifurcatum is a ligament that arises with its posterior end at the upper edge of the heel bone and then divides into two parts, one of which, the ligament calcaneonaviculare, at the posterolateral edge of the heel bone and the other, the ligament calcaneocuboideum , attaches to the posterior surface of the elbow. This short but strong ligament is the 'key' to the cuneonavicular joint, because only when it is severed can the articular surfaces be widely separated from each other in the said joint during foot disarticulation surgery.
- cuneonavicular jointThe cuneonavicular joint is formed by the interaction of the posterior articular surfaces of the humerus with the three articular surfaces of the distal surface of the navicular bone. As for the movement in intertarseae arthritis, mainly the calcaneus, together with the heel bone and the forefoot, rotates with a 55 ° movement around the sagittal axis (this axis is oblique, it enters and occurs from the dorsal side at the head of the heel bone from the sole of the foot on the lateral surface of the heel bone). Inward rotation of the foot (pronation) raises the lateral edge of the foot and the dorsum of the foot rotates medially; conversely, outward rotation (supination) lifts the medial edge and rotates the back of the foot laterally. In addition, adduction and abduction around the vertical axis is possible here, with the back of the foot deviating medially and laterally from the midline. Finally, pronation and flexion around the front axis can also occur. Movement around the three axes also occurs in the talocalcaneonavicular arthrodesis, which is a complex ball-and-socket joint. All these movements are small and usually combined, so that adduction and slight forefoot flexion occur simultaneously with supination, or vice versa: pronation is accompanied by abduction and extension. In general, the ankle joint, in combination with the intertarsa arthrodesis, allows great freedom of movement of the foot as a multiaxial joint.
Which Doctors Should You See to Evaluate Ankles?
Is there anything that worries you? Would you like to learn more about ankles or have an examination? You can make an appointment with your doctor – Clinic Eurolaboratory is always there for you! The best doctors will examine you, advise you, provide the necessary care and diagnose the problem. You can also doctor at home. clinic Eurolaboratory is open for you around the clock.
How to contact the clinic:
The telephone number of our clinic in Kiev is (+38 044) 206-20-00 (multichannel). The clinic's reception staff will arrange an appointment for you to see the doctor. You can find our coordinates and directions here. For more information about all of the clinic's services, please visit the clinic's website.
If you have been examined before Be sure to take the results with you to your doctor's office. If you have not yet done any examinations, we will carry out the necessary work in our clinic or with our colleagues in other clinics.
It is important that you take a very close look at your general health. There are many diseases that do not initially make themselves felt in our body, but are unfortunately treated too late. This simply means that you have yourself examined several times a year to be examined by a doctor several times a yearIt is important to get checked several times a year, not only to prevent a serious illness, but also to maintain a healthy body and mind.
If you want to ask your doctor a question, use the online guide, find answers to your questions and read Tips for self care. If you are interested in opinions about clinics and doctors, you will find the information you need in the forum. Also register on the medical portal Eurocoolto stay up to date with the latest ankle news and information automatically delivered to your inbox.
The architecture of bones
The lower limbs consist of bones of different sizes joined together to form a single structure. This allows it to support the weight of the body during movement and is capable of carrying heavy loads.
The bones of the fingers
It consists of fourteen phalanges and the joints that connect them to each other. Each finger consists of three phalanges, except the thumb, which contains two. These are connected via articular cartilage to the parts of the skeleton that form the metatarsals. The function of the toes is to distribute body weight evenly and improve balance.
The foot consists of sesamoid bones. These are small structures with a rounded shape, their number is individual, there are people who do not have them. Their job is to increase the curvature of the transverse arch.
tarsus
It consists of five prismatic long bones. The first is the strongest, the second is the longest and the shortest is used to adapt to a greater load.
A photo of the bones of the human foot shows that the metatarsal bone forms the connections of the foot skeleton on both sides. The toes on the distal side and the tarsus on the proximal side are attached to it. The main role of the tarsus is to maintain the arch of the foot, which allows work to be distributed efficiently throughout the foot.
tarsus
It consists of two asymmetrical parts. The posterior part contains the bones:
- The calcaneus bone – the largest bone formation of the foot, with an elongated shape that is slightly flattened in the lateral projection. The posterior protuberance forms a bulb to which the Achilles tendon attaches.
- Ramus. One of the most important parts of the leg. It acts as a load balancer between the shin and foot. The structure is complex and depends on the functions it fulfills. The crown part is involved in the formation of the ankle joint, the shaft in the transmission of gravity to the nearest joints.
Joints and articular cartilage
The anatomical structure of the human foot includes joints located where the bony surfaces of the foot meet. Their main function is to form movable joints. They are all covered with cartilage. The cartilage acts as a seal between the bony edges. Thanks to its smooth surface and the lubrication provided by the synovial fluid, it maintains mobility under all conditions.
There are many important joints in the lower limbs that play a key role in shaping movement and maintaining balance of the human body.
ankle
It is formed by the shinbones (tibiae and tibiae) and the talus. Their lower parts - the ankles - enclose the ankle bone and form a 'fork'. It allows the foot to flex and extend and has a range of motion of up to 90 degrees on both sides. It is a very strong joint that is reinforced by a complex of powerful ligaments.
Statistically, the ankle is the most susceptible to injury. This is due to the high loads placed on it and its relatively limited range of motion. Fractures of the ankle joint are often associated with high severity, with displacement of fragments and splintering.
Due to these anatomical circumstances, the injured ankle requires a long time to recover. Even after uncomplicated injuries, full rehabilitation can take several years.
Structure of the tarsal joints of the human foot
Their combination makes the tarsal bone a solid structure, which is characterized by low mobility and high strength in all axes of load interaction.
Subtalar
Cylindrical joint located at the posterior end of the heel bone and talus bone. It is characterized by a thin capsule and small, short, very strong ligaments.
Wedge-shaped
Has a complex structure, does not participate in movement and provides additional strength. It is reinforced by the dorsalis pedis tendons.
Special treatment
Conservative technology
One of the most effective treatments for this condition is cortisone and narcotic injections. Practice shows that for many people the symptoms disappear after just a few injections. If this method does not have any effect (even in the short term), the specialist may have doubts about the correctness of the diagnosis.
However, if there is temporary relief and the pain and discomfort later returns, the patient will need surgery.
Surgical technique
In tarsal sinus syndrome, the essence of the operation is the discovery and subsequent removal of its contents (fat pads).
Arthroscopy of the tarsal joint is rightfully considered the most popular method of revision and elimination of the problem, guaranteeing positive results in 92 % of cases. Thanks to modern arthroscopic equipment, specialists can usually perform a wide range of procedures, such as: B. Chondroplasty, debridement, etc.
costs of the services
Initial consultation with the treating specialist
- Getting to know the patient's complaints and clarifying the cause of the illness
- Investigation
- Description of symptoms
- Analysis of data from blood tests, X-rays, CT and MRI scans
- Creating a diagnosis
- Determination of treatment options
- Clarification and detailed review of the findings from the first visit to the treating specialist
- Establishing the diagnosis
- Defining the treatment
' Blockade with glucocorticoids (price of the drug not included)
- Consultation with the attending physician
- taking blood
- Preparation of the platelet-rich plasma
- Injection of the obtained plasma into the patient's area
- Stay in the medical facility
- Preparation of epidural anesthesia
- Arthroscopic surgical intervention
- Consumables (surgical material)
Postoperative visit to the specialist
- Post-operative examination
- Review of CT, MRI and X-ray findings
- Recommendations for recovery
- Injection of a preparation based on hyaluronic acid
- removal of the threads
Injuries to the tarsus
A fracture of the tarsal bone can be caused by the following causes, among others
- acute exposure;
- Heavy load;
- Strong dorsiflexion of the foot;
- Excessive forced flexion of the foot;
- CAR ACCIDENT.

The affected person immediately suffers from pain, hematomas and swelling, which can spread to the lower leg. The pain increases when palpating and moving the leg. If the fracture is complicated by displacement of the fragments, a visual change in the shape of the ankle can be noted.
Treatment of the fracture must initially include immobilization of the limb. The next steps will be determined by the doctor.
It is equally rare for a cubital bone component to fracture due to direct trauma, e.g. B. due to a blow or a fall with a heavy object on the foot.
The symptoms of trauma are visible: pain syndrome, limitation of mobility, increased pain during movement, swelling, bruising. If there is a fracture with displacement of the fragments, a deformity of the foot can be detected. It is not uncommon for a fracture of the elbow bone to be combined with a fracture of the scaphoid bone.
X-rays, which are the main method of diagnosis, show compromised bone integrity, irregular contours and jagged edges.
First aid is similar to that for a fracture of another bone element of the segment - immobilization with a plaster cast. Physiotherapy and physical therapy are recommended after the cast is removed. Wearing orthopedic shoes for one year is recommended.

The recovery period after a tarsal bone fracture includes the following activities:
How can you prevent foot diseases?
Of course, it is better to prevent the development of pathology in time than to spend time on its short-term treatment. If you follow the following rules, you can forever forget about diseases in the foot area: It is necessary to wear suitable footwear, avoiding high heels. The shoes should be made of high-quality material and have a cushioning function. Shoes should be the right size, no more, no less. A healthy diet is essential for good health. Walking barefoot on uneven surfaces, daily exercise and self-massage.
If there is a hereditary predisposition to diseases in the foot area, special attention should be paid to prevention.
Cookie Settings
IMAIOS and some third parties use cookies or similar technologies, in particular to measure visitor numbers. Cookies allow us to analyze and store information such as the characteristics of your device and some personal data (e.g. IP addresses, navigation, usage and location data, unique identifiers). This data is processed for the following purposes: to analyze and improve the user experience and/or our content, products and services, to measure and analyze audience, to interact with social media, to display personalized content, to measure the performance and attractiveness of content . For more information, please see our privacy policy: Privacy Policy.
You can grant, withdraw or revoke your consent at any time using our cookie settings tool. If you do not give your consent to the use of these technologies, this will be treated as an objection to the validity of the cookies stored. To consent to the use of these technologies, please click the 'Accept all cookies' button.
Cookie Settings
When you visit the IMAIOS website, cookies are stored in your browser.
Some of these cookies require your consent. Click on the type of cookie to enable or disable its storage. To maximize the functionality of the IMAIOS website, it is recommended that you accept different types of cookies.
These cookies ensure the proper functioning of the website and allow it to be optimized (detecting problems when navigating the website, logging in to your IMAIOS account, online payments, troubleshooting and website security). The website cannot function properly without these cookies, so their use is not dependent on your consent.
These cookies are used to measure the number of visitors to the website: traffic statistics allow the website to improve its performance.
The bones of the foot
The foot consists of 26 bones and is divided into several parts: the toes, the tarsal bones and the tarsal foot.
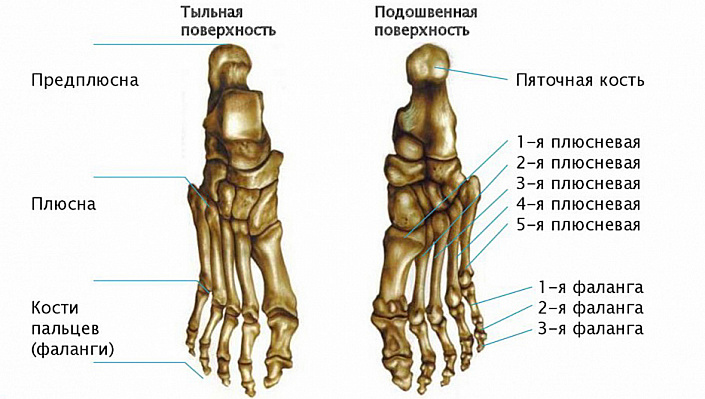
The tarsal bones The tarsus consists of five bones and is divided into two compartments. The middle compartment includes the large bones (talus and calcaneus) and two bones (sphenoid, scaphoid, and tarsal bones).
The pelvic bone It is the largest and connects the foot to the lower leg. This bone has five joints covered by cartilage but no muscles. The ankle bone allows the foot to rotate up to 90 degrees and is used to raise and lower the foot. Since the mobility of the foot to the left and right is very limited, ankle sprains or strains are the most common form of injury.
heel bone The heel bone has six joints and is supported by many ligaments, including the Achilles tendon.
The so-called instep bone of the foot is formed from the the scaphoid (scaphoid). The scaphoid, cuboid and sphenoid bones are strongly connected to each other by tendons and form a very stiff joint.
tarsus The tarsal bones consist of five bones, of which the first is the strongest and the second is the longest. They look like tubes with three sides and rounded ends. The tarsal bone at the junction of the thumb phalanx often suffers from salt deposits.
Phalanges of the toes The fingers have 14 bones (the thumb has two bones instead of three) and are not as long as the hands. But like the hands, there are no muscles in the fingers, only ligaments, so the bones can be easily felt. Often the second and third phalanges of the little finger are fused, which does not affect health and functionality in any way.
Sometimes a person has two extra bones that cause problems for the wearer. The first is the meniscus bone (outer tibia), which occurs in one in ten people and lies in the tendon of the meniscus bone. It occurs twice as often in women as in men. If the navicular bone is large, the back of the foot is high and the shoe rubs against the back of the foot.
Ligaments and muscles
When an adult runs, the load on the foot increases to four times its weight, which is why the tendons in the foot are very strong. The ankle joints are tightly wrapped with tendons that transfer the weight to the ankle bone and also protect the joint from misalignment. The ligaments between the metatarsal bones, which run from the heel to the metatarsal bone, cushion the two arches of the foot. When they are weakened, flat feet develop.
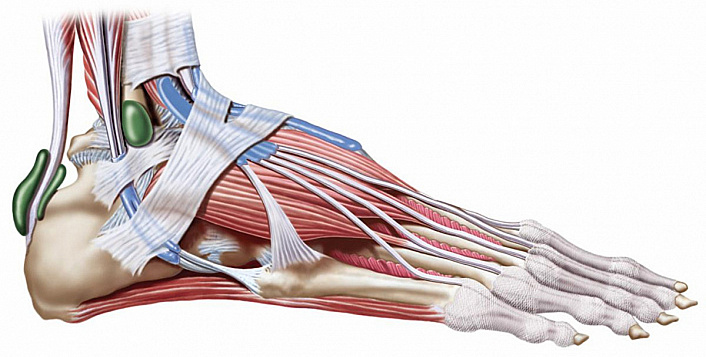
The muscles also help support the weight of the body. The short extensor muscles are responsible for extending the toes, while the short flexor muscles under the metatarsals are responsible for flexion. The flexor muscles are much stronger than the extensor muscles because they help support weight and maintain balance. When walking, half of the body weight rests on the toes while the heel is lifted. The soleus flexus muscle, which includes the above-mentioned flexors, is responsible for maintaining the arch of the foot, extends from the heel to the metatarsal bone and can be felt by palpation. Interestingly, toddlers and teenagers find it easier to raise their foot, while adults with strong calf muscles find it easier to lower their foot.
The toenails are thicker and grow slower than on the hands. With age, they become even thicker because metabolism deteriorates and the nail plate does not have time to grow beyond its growth zone. On the big toe, the nail often grows into the soft tissue, which is not uncommon. In most cases, the cause is shoes that are too tight or the foot overheating in closed shoes on hot days. Poor pedicures, fungal infections, big toe injuries, and flat feet can also lead to ingrown nails. In the latter case, uncomfortable footwear is again the cause. An ingrown nail is treated both orthopedically and (in advanced cases) surgically.
Blood reaches the foot via the superior gluteal artery, the posterior tibial artery, and the dorsal artery, which divide into smaller tubes in the knee and into a network of smaller vessels in the foot. The vein that ensures blood drainage (great saphenous vein) begins at the big toe. Since the feet are the lowest part of the body, they are often under-supplied due to poor blood circulation. All feet are affected, but in the absence of obvious disease, a person may simply suffer from ice foot syndrome. In this case, the cardiovascular system should be checked, or the body should simply move more.
Diagnosis of dislocated feet
During the visit, the podiatrist first examines the injured foot and performs a palpation. Based on the characteristic symptoms, the doctor can guess the nature of the injury, but a visual diagnosis is required for confirmation. An x-ray is usually taken. It shows the position of bones and joints and allows the visualization of sprains, fractures and fractures.
In complicated cases, a CT or MRI scan may be necessary. These examinations can assess the condition of the soft tissues and diagnose injuries to muscles, ligaments and tendons.
Treatment of foot sprains
Treating a sprain involves several steps. First, the doctor must adjust the joint and restore the proper position of the bones. Once the injury is closed, reduction can be performed conservatively. If there is an open wound and torn ligaments and tendons, surgery may be necessary.
Once the dislocation is resolved, a cast or other restraining bandage is placed around the leg to immobilize it (immobility necessary for normal healing). Depending on the type of injury, this must be worn for several weeks to months.
Your doctor may also prescribe medication during this time. Painkillers and anti-inflammatory medications are used.
Rehabilitation after a foot fracture
After the fixation bandage is removed, swelling and pain may remain for a long time.
To speed up recovery, the patient needs:
- Stretching massage of the foot and lower leg.
- Increased physical activity with mandatory physiotherapy. The exercises should be performed daily without skipping classes.
- Physical therapy.
- Wearing supinators. This condition is mandatory. If all the above measures are completed after three months, the person will have to wear supinators for at least 12 months, sometimes even longer.
Another common recommendation from trauma surgeons is to wear special orthopedic shoes. After the cast is removed, it is recommended to wear these shoes for six months.
Surgery for metatarsal fractures
Fractures of the metatarsal bone that are displaced by more than half the width of the bone represent an indication for surgery.
Percutaneous fixation with spokes
It has been popular for many years and remains one of the most commonly used techniques worldwide.
First, the doctor closes the fracture displacement and then the spokes are drilled through the fracture in specific directions (determined by the type of fracture).

Advantages: Low trauma, quick, easy, inexpensive, no incision and therefore no postoperative scarring.
Disadvantages: The ends of the spokes remain above the skin so that the spokes can be removed after the fracture has healed; risk of wound infection and infection penetration into the fracture area; prolonged wearing of a plaster cast for 1 month; inconveniences in daily life.
Open repositioning of a fracture

Open repositioning of a metatarsal fracture, osteosynthesis of the bone with a plate and screws. The operation consists of a surgical incision, access to the fractured metatarsal bone by carefully pulling out tendons, vessels and nerves, mobilizing the bone fragments, eliminating the dislocation and fixing it in the correct position.

No plaster immobilization is performed because the metal structure immobilizes the bony fragments.
Walking with heel support is allowed for one month.
Rehabilitation after a metatarsal fracture
Once your metatarsal fracture has healed and the pain has subsided, your doctor will allow you to put weight on your foot, gradually increasing the load.
Do not self-medicate!
Only your doctor can make a diagnosis and prescribe appropriate treatment. If you have any questions, you can call or ask a question via email.
| Treatment of foot fractures | Price, RUB |
| Manual repositioning | from 2,500 |
| plaster cast | from 1,500 |
| Osteosynthesis (without metal work) | from 38,000 |
| local anesthesia | from 700 |
| regional anesthesia | from 3,000 |
| Bandages, suture removal | from 500 |
- Anatomy of the Lisfranc joint.
- metatarsal bones.
- tarsal and metatarsal joints.
- Orthopedic insole junior.
- tarsus.
- The tarsal and metatarsal bones.
- full leg orthosis.
- The tarsal of the foot.