According to this criterion, a distinction is made between primary and secondary osteoarthritis. Primary osteoarthritis of the shoulder is mainly the result of age-related changes and develops after the age of 50. Sometimes, however, the disease begins at a young age without the cause being identified. In this case one speaks of a primary idiopathic shoulder arthrosis. Hereditary predisposition plays a not insignificant role in its development: someone in the family suffers from a similar disease.

- rotator cuff
- anatomy
- causes
- Factors contributing to shoulder instability
- Treatment
- Causes of rotator cuff injuries
- traumatic injury
- degenerative damage
- symptoms
- General description of the biceps brachii.
- Origins of the upper arm biceps.
- Fitness training for trainers.
- Mobilization for stretching
- Sole post isometric relaxation
- ACTIVE MOTION TEST
- PALPATOR TEST
- TENNIS ELBOW SYNDROME
- DIAGNOSIS
- Causes of osteoarthritis of the shoulder joint
- Symptoms of shoulder osteoarthritis
- Initial Symptoms
- Clear Symptoms.
- Medical treatment of periarticular inflammation consists in prescribing:
- How to prevent the development of periarthritis of the shoulder joint?
rotator cuff
The human shoulder joint has a very complex but elegant structure. Its anatomy allows for a wide range of motion, including complex overhead movements. However, increasing the range of motion of the joint reduces its stability. That does that shoulder joint prone to a range of problems when part of the joint is damaged or not working properly.
The condition of the shoulder rotator cuff is critical to the proper function of the shoulder. The rotator cuff is a unique structure made up of four tendons. These four tendons connect to their respective muscles and help keep the humeral head in the center of the socket, stabilizing it and allowing the arm to move in different directions. The rotator cuff can gradually wear down when the shoulder joint is subjected to heavy physical work over a long period of time.
This type of degenerative damage usually occurs in middle age. However, it can also occur suddenly at any age and in the case of acute trauma. A rotator cuff tear is painful and causes noticeable weakness in the shoulder joint.
anatomy
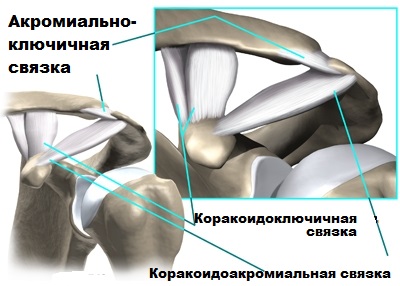
The shoulder joint consists of the humerus, the shoulder blade and the collarbone. The acromion forms the roof of the shoulder joint. The top of the humerus is called the head. The head fits into a small and flat acetabulum.

The acetabulum is part of the shoulder blade. Between the bony structures of the scapula are strong ligaments (the coracoacromial ligament, the acromialoclavicular ligament, and the clublavicular ligament) that provide stability to the joint, but in some cases can also damage the rotator cuff.
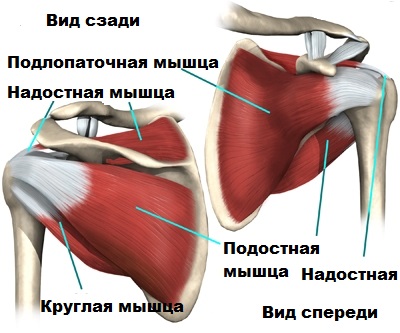
The rotator cuff is made of tough, fibrous tissue. The rotator cuff or rotator cuff surrounds the shoulder joint. The cuff consists of four tendons connected to four muscles (supraspinatus, subscapularis, circularis, scapula). These muscles twist the shoulder inward or outward. Along with the deltoids, they also help lift the shoulder off the body.
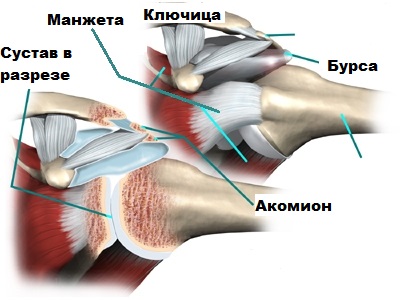
The shoulder rotator cuff slides between the humeral head and the acromion as we raise the arm. There is a special bursa between the rotator cuff and the acromion. The bursa reduces friction between two rubbing surfaces. It lubricates the surface of the cuff and protects it from rubbing against the acromion.
causes
Shoulder instability usually occurs after an injury that causes a partial or total dislocation of the shoulder (e.g., after a fall on the shoulder or outstretched arm, or after a direct blow to the shoulder). These injuries are very common in contact sports such as soccer or rugby. They usually occur from a combination of shoulder abduction and excessive external rotation. Shoulder instability can also develop gradually and is caused by repetitive heavy loading of the shoulder joint during movements that stretch the connective tissue structures of the joint (throwing or swimming). Instability is also caused by poor biomechanics and technique and is most common in athletes who need to move the shoulder overhead (baseball players, javelin throwers, cricketers, tennis players). Shoulder instability can also be caused by congenital weakness of the connective tissue (hypermobility of the joint).

Factors contributing to shoulder instability
There are a number of factors that can contribute to shoulder instability and its associated symptoms. Knowing these factors allows the rehabilitation physician to treat better and avoid recurrence of the instability. These are mainly the following factors:
- A history of episodes of shoulder dislocation (dislocation or subluxation).
- Insufficient rehabilitation after a shoulder dislocation
- Intense exercise or excessive stress on the shoulder
- Muscle weakness (particularly of the rotator cuff muscles)
- muscular imbalance
- Impaired movement biomechanics or sports technique
- Stiffness of the thoracic spine
- shoulder hypermobility
- ligament weakness
- Muscle stiffness due to poor posture
- changes in training
- bad posture
- insufficient warm-up before physical activity
Treatment

The most effective treatment for shoulder imbalances is physical therapy. An exercise program strengthens weak muscles and loosens tight muscles. As an alternative to physical therapy, physiotherapy can also be used to relieve pain. Massage can relieve muscle tension and improve blood circulation in the muscles. An important factor in the treatment of muscle imbalances in the shoulder muscles is changing the working posture, especially if the patient has to sit for a long time at work.
Muscle imbalances are usually treated conservatively. However, in cases where the muscular imbalance is significant and causing complications (e.g., instability), arthroscopic surgery is performed to improve stability of the shoulder joint.
Use of the material is permitted provided that an active hyperlink to the article's permanent page is provided.
Causes of rotator cuff injuries
They can be traumatic or degenerative in nature.
traumatic injury
Acute rotator cuff injury results from various types of trauma. The most common is falling onto your shoulder or suddenly lifting heavy objects. This situation is accompanied by acute pain and functional impairment of the limbs.
Individuals who consistently lift weights, throw, or engage in competitive sports develop permanent micro-injuries to muscles. Since tendons regenerate slowly, such changes sooner or later lead to degenerative changes and tears.
degenerative damage
Age-related changes can also lead to tears in the rotator cuff. This is common in people over the age of 50. Over time, the tendons lose elasticity and are easily injured.
This phenomenon is not uncommon in people whose jobs involve stereotypical movements that involve raising their arms in the air. The process is lengthy and the damage is gradual.
symptoms
An acute injury to the rotator cuff is accompanied by an acute and severe pain syndrome. The pain is localized in the shoulder joint and can radiate to the neck and hand. The pain increases when trying to raise the arm or rotate the shoulder outward. Movement in the shoulder joint is limited or impossible.
In a chronic course, the pain occurs only sporadically at first and is associated with raising the arm upwards. Over time, this unpleasant symptom appears more and more often and intensifies at night. Over time, the pain gets worse and the patient can no longer scratch or undress unaided. If the disease is not treated early, osteoarthritis of the shoulder joint can develop.
General description of the biceps brachii.
The muscle that is considered a symbol of strength around the world is the biceps (biceps brachii – from Latin. Biceps brachii muscle).
Not only is this muscle the focus of many exercising men, but it is also a very important structure that has allowed humans to compare themselves to their counterparts in the animal kingdom.
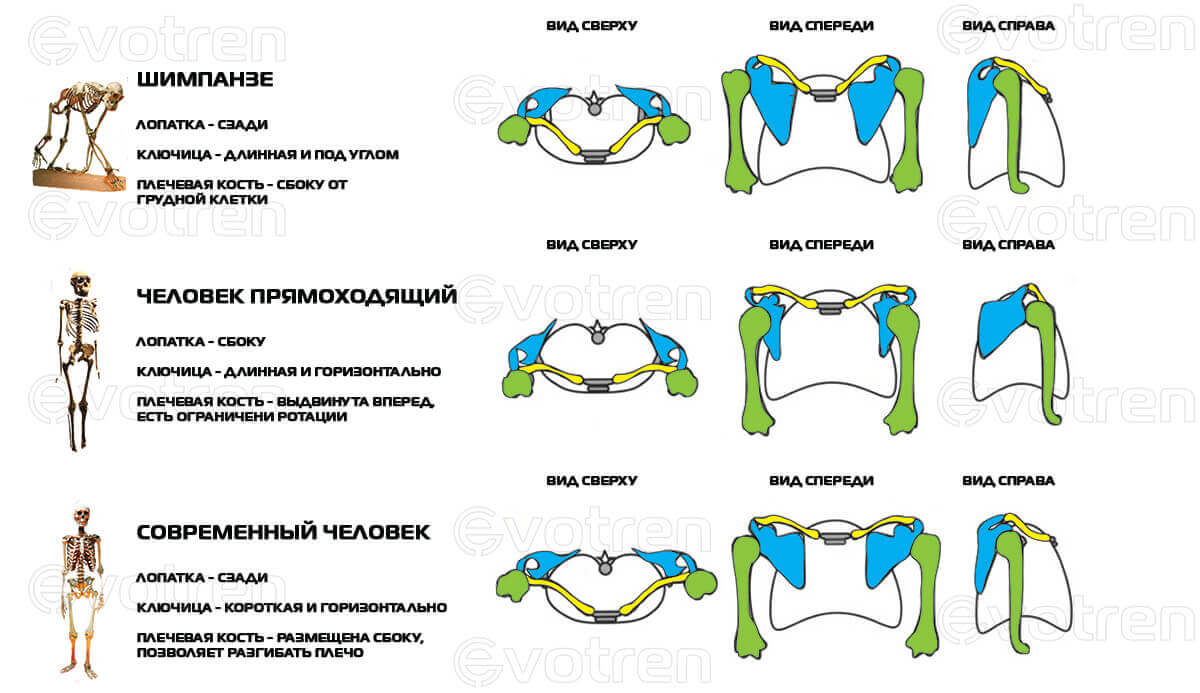
If you look at the structure of this muscle in monkeys, you'll see that they have a stronger but less functional muscle.
It is important to understand that shoulder rearrangement in humans is related to the importance of projection, among other things.
Scientists work with the term 'elastic energy'. The structures of the shoulder act like a kind of slingshot, with the biceps pulling on an 'elastic band'. This allows man to be an excellent thrower, which has greatly facilitated the mastery of nature (javelin throw, stone throw, etc.).

In addition, the biceps brachii is an active aid in eating (it brings food to the mouth) and in the use of tools (it generates a strong rotational force).
The biceps brachii consists of two heads that originate at different points but are joined at the point of attachment.
An important difference from the animal world is the position of the human shoulder blade. These differences partially alter the biomechanics of the movement and give the biceps brachii greater functionality.
Origins of the upper arm biceps.
- Short head (caput breve) – beak process of the shoulder blade (processus coracoideus scapulae)
- Long head (caput longum) – supraglenoid process of the scapula (tuberculum supraglenoide scapulae)
Fitness training for trainers.
For fitness instructors looking for courses that will increase their income, make them even cooler, and allow them to never fight for a job again, we recommend the following correspondence courses:
Personal trainer basic course. – For trainers who want to supplement their knowledge with basic information. An incredible amount of useful material that will take you to the next level.
upgrade – Online course for fitness trainers who want to increase their income and knowledge. Custom Themes.
architecture of the body – Dmytro Gorkovsky's special course with full-day practical and theoretical training for fitness trainers, massage therapists and doctors.
pregnancy – Training techniques for pregnancy courses and postpartum rehabilitation.
Pilates - Ekaterina Vasilenko's online course on the techniques of the Pilates system.
Mobilization for stretching
The practitioner increases the amplitude of the initial hand and forearm shift in smooth, slow, repetitive motions.
1 The exerciser performs passive muscle pre-tensioning, increasing hand pronation with little effort, until a light, elastic, comfortable sensation of tissue tension (elastic barrier) is achieved, which he maintains for 3-5 seconds to contract the muscle to get used to the tension (habituation).
2. The patient looks up, inhales slowly and evenly, holds the breath and attempts to supine the forearm by rotating it outwards for 7-9 seconds with minimal effort against appropriate slight resistance from the physician.
3. The patient exhales slowly and calmly, gently relaxing the muscle and looking down while the therapist performs an additional gentle passive stretch of the muscle, increasing the amplitude of pronation of the hand or forearm with minimal effort until an elastic There is resistance (tension) in the tissue or a slight pain for 5-10 seconds. In this new stretched position, the muscle is held in tension to repeat the isometric work.
4 The technique is repeated 4-6 times without breaking the stretching force between repetitions, gently holding the muscle in the stretched position and not returning to the neutral position.
Sole post isometric relaxation
Performed in the same way while seated. Pressure is applied with the free hand to the posterior surface of the affected arm or the posterior surface of the forearm to isometrically load and then stretch the muscle.
Note: With effective treatment, the elbow can be hyperextended, which was previously not possible, and the arm can be flexed without restriction. Tapping on the outer epicondyle becomes painless. If tenderness persists after treatment, the nearby muscles, most commonly the ulnar or triceps brachii, are suspected.
Forearm Supination - Supination Pronation Exercises - Seated Position.
Patient: sits with arm on armrest or special support, light dumbbell in hand.
Execution: The patient performs a supination and pronation of the wrist. Note: The weight of the dumbbell increases as the muscle strengthens.
Start this exercise when the elbow pain has subsided.
ACTIVE MOTION TEST
Procedure: The patient performs dorsiflexion, supination, active finger extension, or a combination of these movements against the physician's resistance. Evaluation of Outcome: Hypertonicity of the extensor and supinator muscles of the forearm causes or increases pain in the upper third of the external surface of the forearm and elbow.
H. Kopell, W. Thompson test. The patient attempts to straighten the third finger flexed at the wrist against the operator's resistance while straightening the hand at the elbow. Evaluation: Hypertonia of the radial extensor causes or exacerbates pain in the elbow and upper forearm.
Supinator syndrome, Froese arch syndrome, Thompson-Copell syndrome. Compression of the posterior branch of the radial nerve may occur 2 cm below the elbow joint as it passes through the fibular ring (Froese's arcade) and subsequent muscular tunnel between the superficial and deep supinator bundles. The supinator, along with the nerve, wraps around the radial bone during pronation (which stretches the nerve) and arises during supination of the forearm. With supinator syndrome, there is pain in the outer parts of the elbow and on the posterior surface of the forearm, but no sensory disturbances are noted.
PALPATOR TEST
Pain occurs when pressure is applied to the forearm in the anterolateral aspect of the forearm, approximately two fingertips below the external epicondyle of the humerus. Treatment consists of injecting glucocorticoids into the area. motor test. The pain is associated with hyperextension of the elbow joint and pronation of the forearm.
TENNIS ELBOW SYNDROME
Travell JG and Simons DG described the syndrome from the perspective of a myofascial lesion. Overstretching of the extensor muscles is referred to in the literature as tennis elbow syndrome or epicondylitis. All variants of 'tennis elbow' can be explained by a myofascial lesion. Cervicothoracic sciatica can produce muscle damage leading to a muscular (as a major variant) manifestation of tennis elbow syndrome. Osteoarthritis can occur in any part of the elbow joint, but the external epicondyle is rarely the source of the pain. Pain in the epicondyle is most often caused by the nearby muscles and is rarely neurogenic in origin. In cases of doubt, a radiological examination is indicated.
DIAGNOSIS
Forearm Supinator - Non-specific handshake test. A firm handshake becomes painful due to simultaneous damage to the extensor muscles of the wrist and fingers.
Supination of the forearm - palpation (according to Travell JG and Simons DG). Shock and palpation of the external epicondyle. Impact or pressure on the area of the external epicondyle causes severe pain that often radiates to the base of the thumb. The movement of the thumb is usually unrestricted and painless.
Painful areas may be visible:
A. Near the insertion of the superficial muscle layer on the ventral surface of the radial bone, slightly outward and distal to the tendon of the biceps muscle. For palpation, the arm is slightly flexed at the elbow (15-30°) with the brachioradialis muscle relaxed and allowed to move outward, the hand is fully supinated. In this position, the muscle thickening is just above the radius, under the skin, between the biceps tendon and the brachioradialis. The contours of both muscles are clearly visible when the patient is asked to flex the forearm under tension.
B. At the muscle insertion where the outer edge of the joint capsule touches the ulna. By palpating deeply below the long extensor wrist, 4-5 cm distal to the external epicondyle and 1-2 cm distal to the head of the radial bone (the presence of the latter point is usually associated with compression of the deep branch of the radial nerve).
Causes of osteoarthritis of the shoulder joint
- Consequences of acute trauma - dislocations, subluxations, intra-articular fractures, bruises;
- long-lasting micro-injuries related to work or sport;
- acute and chronic inflammatory and autoimmune processes in the shoulder joint – acute purulent arthritis, chronic rheumatoid, psoriatic and other arthritis;
- chronic inflammatory processes in periarticular tissues – inflammation of the shoulder joint and cartilaginous joint, leading to impaired blood supply and cartilage nutrition;
- Metabolic (metabolic) disorders of the joints – gouty arthritis;
- endocrine disorders;
- congenital malformations (dysplasia) – e.g. B. on the joint surfaces of the shoulder joints.
Each of these causes (sometimes several at the same time) disrupts the composition and volume of the synovial fluid that nourishes the cartilage in the joint. Cartilage gradually decreases in volume, breaks down and loses its cushioning properties. This leads to trauma to the bone, its hypertrophy at the edges of the articular surfaces, deformation of the joint and reduced function. Synovitis – inflammation of the joint sometimes develops in the joint cavity. Because of the synovitis, the osteoarthritis is referred to as osteoarthritis or osteoarthritis - depending on which process predominates (inflammatory or metabolic-dystrophic). As a result of inflammation and necrosis, small tissue fragments—sequestra or joint mice—detach from the bone.
- From micro-injuries – blacksmiths, miners, tennis players, weight lifters, discus throwers;
- with acute injuries – gymnasts, track and field athletes, circus performers;
- people with an unfavorable history;
- People suffering from chronic joint disease.
Symptoms of shoulder osteoarthritis
Gradual onset of the disease. The rate of progression depends on the cause, the patient's general condition and heredity.
Initial Symptoms
The initial symptoms of shoulder osteoarthritis can be overlooked, especially when they occur in conjunction with an existing shoulder problem. These include mild intermittent discomfort and frequent pain, especially after physical exertion. Pain in the left shoulder can be mistaken for heart pain. They pass quickly, but they are worth paying attention to.
If these symptoms appear again, it is better to consult a doctor immediately, since any disease is easier to treat in the initial stages.
Clear Symptoms.
The pain intensifies and does not go away immediately after exercise. The pain occurs at night and when the weather changes. Movements in the shoulder are painful and are accompanied by a characteristic crunch. Stiffness occurs in the morning or when standing in a certain position for a long time, and you have to move to relax it. The pain can be localized not only in the shoulder, but also radiate to the shoulder, neck and upper back.

From time to time the joint swells, the skin over the joint turns slightly red, and the pain increases and is constant. There may also be a slight increase in body temperature. This is a symptom of synovitis - an aseptic (without infection) synovitis. If there are foci of infection in the body (cavities, ENT diseases, etc.), then they can penetrate the joint through the blood and lymphatic vessels and cause a purulent inflammatory process. This can lead to a high fever, headache and a sudden change in general condition.
The combination of degenerative-dystrophic and inflammatory processes in the joint gradually leads to a permanent loss of function of the limbs and constant pain.
Medical treatment of periarticular inflammation consists in prescribing:
- Non-steroidal anti-inflammatory drugs;
- chondroprotectors;
- Anti-inflammatory and warming ointments;
- biostimulants.
If the progression of the disease could not be stopped and a subsequent examination reveals osteoarthritis, it is more difficult, if not impossible, to solve the problem with conservative methods. In such cases, intra-articular injections of Noltrex can be used to restore synovial fluid viscosity and normal mobility of the shoulder joint - every 1-2 years depending on disease progression.
Has the disease already progressed to osteoarthritis? Ask your doctor about treatment with Noltrex for intra-articular injections.
How to prevent the development of periarthritis of the shoulder joint?
The absence of pain does not mean that you can experiment with your health. It's important to take care of it before worrisome symptoms appear.
- Pay special attention to your upper limb joints when exercising in the morning.
- Make sure you eat a balanced and healthy diet.
- If you already have extra pounds, work with your nutritionist to find the best approach to solving the problem.
- Avoid excessive cold because it is bad for the joints, the muscles and the viscosity of the synovial fluid.
- If possible, avoid lying on one side at night so as not to impair blood circulation in the upper limbs.
- Watch your posture. Poor posture leads to osteochondrosis, shoulder and shoulder joint arthrosis and arthrosis.
- When you lift weights, you shouldn't put too much strain on your shoulder muscles.
- Don't ignore internal diseases because any inflammation in the body, even chronic, can cause osteoarthritis.
Osteoarthritis in the shoulder is one of the diseases that can still be treated. The most important thing is to notice shoulder problems quickly and sound the alarm before osteophytes form in the joints. If your orthopedic rheumatologist insists on treating your shoulder osteoarthritis, do not despair: the intra-articular injection of Noltrex will give you back the joy of movement quickly enough and for a long time!
Read more:- Pronator - what does that mean?.
- Pronation and supination of the shoulder.
- The pronator is in anatomy.
- pronator and supinator muscles.
- How much does shoulder surgery cost?.
- tearing of the joint capsule.
- Pronation of the shoulders - what is it?.
- How much does shoulder dislocation surgery cost?.