Obesity is the cause of many joint problems. It leads to the destruction of cartilage, ligaments and tendons that stabilize the ankle. Therefore, the operation can be postponed for a while until the patient gets rid of excess weight.

- Surgical correction of the flat foot
- Price
- Prostheses after foot amputation - the Triton foot
- The first implants
- Construction of modern products
- PROSTHETICS AFTER AMPUTATIONS IN GERMANY
- product types
- Advantages of thermoplastic flat foot fixators
- period of rehabilitation
- fixation
- Approvals and Certificates
- Main specialties
- When is surgery required?
- Types of nylon prostheses
- properties of the material
- Advantages
Surgical correction of the flat foot
flat feet – is a deformity of the foot caused by a prolapse of the arch of the foot – longitudinal or transverse. In the early stages it is treated conservatively. In advanced stages, there is severe pain and dysfunction of the foot, both in terms of support and elasticity. In this case, only surgical treatment is indicated.
- During the operation, a 3-5 cm long incision is made;
- The operation is performed under spinal anesthesia;
- Choosing a specific implant that will restore the correct alignment of the foot bone;
- Recovery time after surgery averages 7 days;
- After the operation, the patient wears special footwear that transfers the load to the heel;
- Full recovery takes between 3 and 5 weeks.
The patient walks with the implant until the muscles and ligaments have 'accustomed' to the new shape of the foot. After that, the implants are removed.
When are flat feet treated surgically?
Surgical treatment is recommended from stage 2 of flatfoot.
The success rate of surgical treatment of flat feet is as high as 99% %. After surgery, orthoses are recommended.
Price
The cost of surgical treatment of flat feet ranges from 60 to 100 thousand rubles (depending on the category of the planned operation, not including the cost of implants).
| service | Price | Registration at the reception |
|---|---|
| Visit to a traumatologist | 3000 rubles |
| Flatfoot correction | from 30000 RUB |
| residence | from 5000 RUB |
| Preoperative consultation | from 6000 rubles |
| Custom orthotics | from 3500 RUB |

Soyuz Clinic offers you the most effective and efficient method of treating thickening of the big toe (valgus deformity of the big toe). Using modern surgical methods of treatment and conservative treatment programs for speedy recovery and prevention, we restore the beauty and health of women's feet.
Prostheses after foot amputation - the Triton foot
Foot amputations are now performed at more than a dozen different levels, from the removal of a single toe to a complete metatarsal resection. Therefore, there are many different models of foot prostheses today.
By the way, a person who has undergone Lisfranc or Chopard surgery can manage quite well at home without a prosthesis, that is, he can stand and walk unaided, which is very convenient, for example, when taking a shower. These people can move about with a prosthesis and feel more secure.

In Syme and Chopar amputations, the acetabular socket usually begins just below the knee. As a result, the patient may need special footwear that has extra padding under the sole of the sound leg, which is sometimes shorter than the artificial limb in such situations. Precise measurement technology has made it possible in recent years to produce prostheses for Chopar and Lisfranc amputations with open ankles and ankles.
With a good short residual limb at the level of the tarsus, experts recommend an ankle joint-supported prosthesis with tibia bones, while a so-called capsular prosthesis is more justified in the case of poor residual limb conditions. A modified Teufel prosthesis is available as a lighter and better ventilated intermediate version.
As far as the materials are concerned, various plastics are mostly used today for cosmetic and functional prosthetics in the foot area, but above all highly elastic silicone rubber, which ensures even pressure distribution and optimal adhesion to the residual limb. Silicone foot prostheses are easy to care for and require little maintenance, can be individually adjusted in color and size and are usually worn like standard shoes or even 'barefoot'.
The first implants
The first endoprostheses had an imperfect design and were fixed with bone cement. In order to attach them, most of the articular surfaces had to be removed. The remaining bone tissue could not adequately support the prosthesis components, resulting in instability and rapid loosening of the implant.
The proximal component was always attached to the tibia, the distal component could be attached to the calcaneus, calcaneus, or calcaneal block synostosis.
Legacy prosthetic models were constrained and had a single axis of motion. Complications often arose after insertion and the result of the operation was unsatisfactory. Such endoprostheses quickly wore out, which is unacceptable in young and middle-aged people. Fortunately, the modern models no longer have many of the disadvantages of their predecessors. They are more advanced and guarantee much better surgical results.
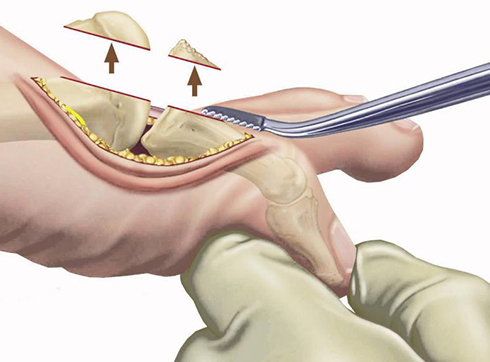
Construction of modern products
Cementless three-part endoprostheses are currently used in clinical practice. They are attached directly to the bone and fused tightly to it so that they remain stable. Only a minimal amount of bone tissue needs to be removed to insert them.
Modern prostheses consist of three parts that form a single mechanism:
- The pelvic component. This is a wear-resistant, arcuate metal component that attaches to the talus.
- tibia component. It is a flat plate of strong alloy that aligns with the shin.
- meniscus insert. Looks like a thin, smooth plate. It is inserted between the two aforementioned parts. Acts like a shock absorber.

Newer models have several axes of movement and enable optimal mobility in the ankle joint. They allow not only flexion and extension of the joint, but also rotation and rotation.
The ankle has complex anatomical-physiological and mechanical properties that are very difficult to replicate. Therefore, ankle replacement still gives less satisfactory results than arthroplasty of other joints (hip, knee). The reason for this is insufficient reproduction of the biomechanics of the joint or incomplete reconstruction of the ligament apparatus. That is why scientists are still developing new, more advanced implant models today.
PROSTHETICS AFTER AMPUTATIONS IN GERMANY
Today, foot amputations are performed at more than a dozen different levels, from the removal of a single toe to the resection of the metatarsal. This is why there are so many different models of prosthetic feet today.
Anyone who has had an operation according to Lisfranc or Chopar can also manage at home without a prosthesis, ie they can stand and walk without outside help, which e.g. B. is very practical when showering. They can also move around with a prosthesis, giving them more confidence.
In Syme and Chopar amputations, the stump stem begins just below the knee. Special footwear may therefore be required, with extra padding under the sole of the sound leg, as the artificial leg is sometimes shorter than the leg in these situations. In recent years, thanks to precise measurement technology, it has become possible to produce prostheses for Chopar and Lisfranc amputations with open ankles and ankles.
In the case of short residual limbs that are well preserved at the level of the tarsus, experts recommend a tibia stump-supported prosthesis, while a cap prosthesis makes more sense in the case of poor residual limb conditions. The modified Teufel prosthesis is offered as a lighter variant for a better ventilated intermediate prosthesis.
Various plastics are used today for cosmetic and functional prostheses in the foot area, but highly elastic silicone rubber is used most frequently, which enables even pressure distribution and optimal adhesion to the residual limb. Silicone prosthetic feet are easy to care for and low-maintenance, individually adjustable in color and size. They are worn with standard footwear and can even be worn barefoot.
product types
A standard footbed consists of two parts:
- The insole is usually an insole supinator that closely follows the curves of the arch of the foot. It supports the entire structure and keeps the foot in an anatomically correct position.
- Splints - firmly enclose the shin and protect the ankle from behind.
These devices can be fitted with additional elements such as straps and other fasteners.
The appearance of the design largely depends on the function that the model is intended to perform. However, it is not advisable to choose the orthosis yourself, as only the doctor can assess the ankle and determine how the orthosis should be worn.
One of the most important criteria for choosing an orthosis is the degree of rigidity, which is determined by the stage of development of the pathology:
- With minor anomalies or for prophylactic purposes, soft constructions are prescribed.
- For moderate foot conditions, semi-rigid orthopedic models can be used.
- After a serious injury to a joint, it should be completely immobilized. This can be achieved through the use of a rigid orthosis.
When choosing an orthosis, the material from which it is made is important. Orthoses are made of elastic fabric, neoprene or silicone, for example.
Among the traditional orthoses for supporting a clubfoot, modern orthoses made of low-temperature plastics are enjoying increasing popularity. They are made from environmentally friendly raw materials, so they are also suitable for people with sensitive skin. They are lightweight and comfortable to wear, extremely durable and aesthetically pleasing.
Advantages of thermoplastic flat foot fixators

The use of low-temperature plastics in orthopedics enables the production of individually designed orthoses. At temperatures between 60 and 100 °C, they become malleable and can be easily attached directly to the patient.
These products are significantly more powerful than standard models. The main advantages of thermoplastic orthotics are
- Multiple mouldability - the material can be repeatedly heated and the shape can then be adapted to new circumstances.
- Accessibility – no special devices are required, which not only makes it easier to work with the orthosis, but also significantly reduces the price of the product.
- LIGHT WEIGHT - The thin and light thermoplastic material is suitable for both adults and children. Particularly suitable for longer wear.
- High durability - after hardening, the material is durable and has increased abrasion resistance.
- Safe - hypoallergenic perforated polyurethane does not cause irritation, allows skin to breathe and does not stick to hair.
Hygienic care of the product does not require special skills or equipment. The orthosis is easy to clean with a simple soap or alcohol solution and, thanks to its resistance to moisture, can also be used for treatments in water.
The low-temperature plastic footbed stabilizes and corrects the foot position. Convenient closure for quick fixation.
period of rehabilitation
After the endoprosthesis has been replaced, the patient stays in the hospital for a few days so that the medical staff can quickly identify any complications and initiate immediate treatment. Regular instrumental controls (usually radiological) of the ankle are performed to visualize the surgical site. Painkillers such as analgesics, nonsteroidal anti-inflammatory drugs, muscle relaxants, and glucocorticosteroids are part of the therapy regimen. The wound is drained to remove exudate and irrigated with antiseptic solutions. The operated ankle is immobilized with a splint or a rigid orthosis.

After 2-3 days the patient can sit, and after another day he can move around the hospital room. The patient is discharged from the hospital if there are no adverse consequences of the procedure. In the next 2 weeks, the ankle will be therapeutically stressed under medical supervision.
During the recovery phase, the patient is treated gently without putting heavy strain on the operated joint. Painkillers, physiotherapy and massages are indicated. The movement therapist will compile an individual complex of exercises to eliminate the stiffness of the ankle.
Report 'Non-surgical treatment of osteoarthritis of the ankle' by Dmitry Karateev (Moscow, Russia).
fixation
A fully removable maxillary denture covers the palate and the jaw itself, while a mandibular denture covers only the lower jaw. These structures are usually attached with suction cups. There are special products that strengthen the seat. They make wearing the prosthesis easier and more comfortable, protect the gums from damage and allow almost any food to be eaten. As a rule, these are creams with hypoallergenic ingredients.
Dentures should be removed from the mouth and cleaned regularly. It is best to do this every time after meals, but if not, they can be washed in the morning and evening. A removable full denture can be left in the mouth overnight, but it is better to take it out to allow the gums to recover. In this case, the prosthesis should be thoroughly cleaned - rinsed with boiled water, treated with an antiseptic solution or brushed with a toothbrush before placing it in a special box. It is recommended to have the prosthesis professionally cleaned twice a year.
It's a common misconception that dentures should be stored in water or a special solution. That's not true - this method used to work well for rubber prostheses, but modern technology has made it possible to move away from it. It is enough to wrap the artificial limb in a cotton cloth and store it in a special box, where it will be protected from the sun, mechanical damage, heat and chemical influences.
Approvals and Certificates
| Designation | OT price |
|---|---|
| Specialist medical advice (included in the execution price when ordering a prosthesis) | 500 р. |
| Cost of a complete removable prosthesis for both jaws | 60000 р. |
In our price list you will find the costs for our services, including advice, diagnosis and the manufacture of removable dentures.
The cost of the services is determined individually for each patient, since the individual characteristics of the patient's mouth play an important role in the manufacture of the dentures. Factors such as the anatomical structure of the jaw apparatus, the type of construction chosen, the material and methods of attachment as well as the shape and color of the artificial teeth are taken into account.
The dental laboratory 'Denta Labor' manufactures removable full dentures of excellent quality. Our laboratory offers all the prerequisites for the production of high-quality and durable prostheses. For prices of removable dentures, please contact us by phone. +7 (495) 162-08-25.
Special offer!!! When you prepay for a full denture, you pay up to 2,000 less.
Main specialties
Reconstructive foot surgery can help with the following problems
- restoration of tendon function;
- reconstruction of defects after amputation;
- repair damaged nerves;
- elimination of skin defects;
- endoprosthetics.
Reconstructive surgery of the foot is often performed after trauma. It can also be part of a complex treatment of bone, muscle, nerve or tendon diseases of the limbs.
When is surgery required?
Correction of the foot is required when the foot is deformed by trauma or congenital factors. Choosing the appropriate surgical option depends on the complexity of the defect. For example, in the early stages of a flat foot or valgus deformity, surgery is not required. Correction of the foot can be done using special orthoses and therapeutic exercises. However, if the deformity is irreversible, only reconstructive surgery can solve the problem. Whether surgical intervention is advisable is decided by the doctor after an individual examination of the patient.
Reconstructive surgery is required for poorly healed fractures. It is required for grade 3 and 4 flat feet.
Types of nylon prostheses
The flexible orthopedic systems are divided into:
- Classic systems dental nylon.
- constructions polyurethane – Russian analogues, which are no worse in terms of quality and convenience, but cheaper than imported systems.
- QuattroTi – Bust (bow) systems made from the monomer-free material DENTAL D. Stronger, more elastic than dental nylon, less abrasive, can withstand high chewing loads.
Depending on the type, nylon dentures are divided into partial and full dentures:
- partial dentures They are cemented to the supporting teeth on either side of the cavity. The attachments are identical to the color of the gums and do not affect the aesthetics. A nylon partial denture is indicated to replace 1 or more tooth units.
- Full denture made of nylon used in case of an edentulous jaw. It sticks in the mouth through a vacuum effect - through natural suction on the gums. Upper jaw prostheses have a small plate (palate support) for suction on the palate. In addition, adhesive pastes and gels are used to more securely attach the complete mandibular denture made of nylon.
No metal is used to manufacture the prosthesis system. This ensures quick adjustment, high wearing comfort and prevents the formation of electroplating. They are easy to remove and insert without damaging the mucous membrane and enamel. Removable nylon dentures for the upper jaw are provided with a palatal flap, which provides better fixation in the mouth.
- missing one or more teeth in a row;
- complete toothlessness;
- Incomerte, endodontic defects;
- bruxism; early stages of periodontal disease;
- inability to place a fixed restoration;
- allergies to plastic, metal;
- Temporary solution before implantation;
- in case of loss of a milk tooth (to avoid displacement of the dentition to make room for the eruption of the permanent tooth).
properties of the material
Thermoplastic nylon is a soft, flexible material that contains no monomers (methyl methacrylate) in its structure. It is a type of plastic, so in addition to its high elasticity, the polymer also has a sufficient safety margin. Light caproic structures are often referred to as 'invisible'. The translucent base literally merges with the gingival mucosa and ensures good aesthetics. This applies to both the base of the restoration and the fasteners. With careful and quality care, it will retain its original appearance throughout its lifetime.
The polymer, which is heated to body temperature, is resistant to moderate chewing loads. The softness and elasticity of the material ensure comfort and a short adjustment time. Reproduces the anatomical shape of the jaw without putting undue pressure on the gingiva. However, unlike acrylic or non-acrylic equivalents, the flexible frame is unable to distribute chewing pressure evenly throughout the jaw. The soft base flexes in the chewing area, which means the chewing pressure is concentrated in a specific zone instead of being distributed over the entire row. This causes discomfort when chewing, accelerates jawbone loss beneath the restoration, and the restoration quickly collapses.
Due to their softness, nylon constructions accelerate the atrophy process – bone volume decreases by 1 mm per year. If the tissue yields 2-3 mm, it becomes difficult to use and the restoration must be replaced with one designed with new parameters. Nylon prostheses therefore need to be adjusted regularly and replaced frequently. The exception is the light but very robust QuattroTi system.
Advantages
- lightness, flexibility;
- ductility
- relative strength;
- Aesthetics;
- biocompatibility;
- easy installation, easy maintenance;
- secure fixation;
- Hygiene.
- How much does a prosthetic foot cost?.
- Schopar'sche joint.
- Schopar and Lisfranca joints are.
- Modern leg prostheses.
- The reamputation is.
- prosthetic leg.
- Leg prosthesis below the knee.
- prosthetic legs.