Raising the biceps in supination trains additional muscles, stabilizes the forearm and makes it strong. This is especially important in arm wrestling.

- Extensor and supinator muscles
- Muscle group of the forearm
- Pronation and supination: what they mean
- pronation of the foot
- How to do hand strengthening exercises
- Exercises for the hand muscles
- Radial group of superficial forearm muscles
- Ulnar group of superficial forearm muscles
- Development of grip strength
- Development of the pronators and supinators
- What are supination and pronation?
- What is WHP?
- Why is this necessary?
- What should I do?
- Rotation of the shoulders
- What diseases can impaired supination lead to?
- What diseases do pronation disorders lead to?
- What is supination?
- Hyperpronation or excessive pronation of the foot
- Aids of the muscles
- Vessels and nerves in muscle tissue
Extensor and supinator muscles
The flexor and extensor muscles are differentiated according to their function: some bend and stretch the entire hand, others stretch and lengthen the fingers. In addition, there are pronators and supinators, which carry out the corresponding radius movements. All of these muscles can be divided into two groups: the anterior group, which consists of flexors and pronators, and the posterior group, which consists of extensors and supinators.
Each group consists of a superficial layer and a deep layer. The superficial layer of the anterior group originates from the medial epicondyle of the humerus, the same layer of the posterior group originates from the lateral epicondyle. The deep layer of both groups no longer has its main point of attachment at the epicondyle, but rather arises from the bones of the forearm and the interosseous membrane.
The terminal insertions of the flexors and extensors of the hand are at the base of the metacarpals, and the finger muscles insert on the finger bones, with the exception of the long extensor of the thumb, which inserts on the first metacarpal.
The pronator and supinator muscles attach to the radius bone. The forearm muscles consist of fleshy parts near the shoulder, while towards the hand they develop into long tendons, so that the forearm looks like a cone that is flattened from front to back.
Muscle group of the forearm
Superficial layer of the forearm muscles Superficial layer of forearm muscles The forearm consists of the following muscles.
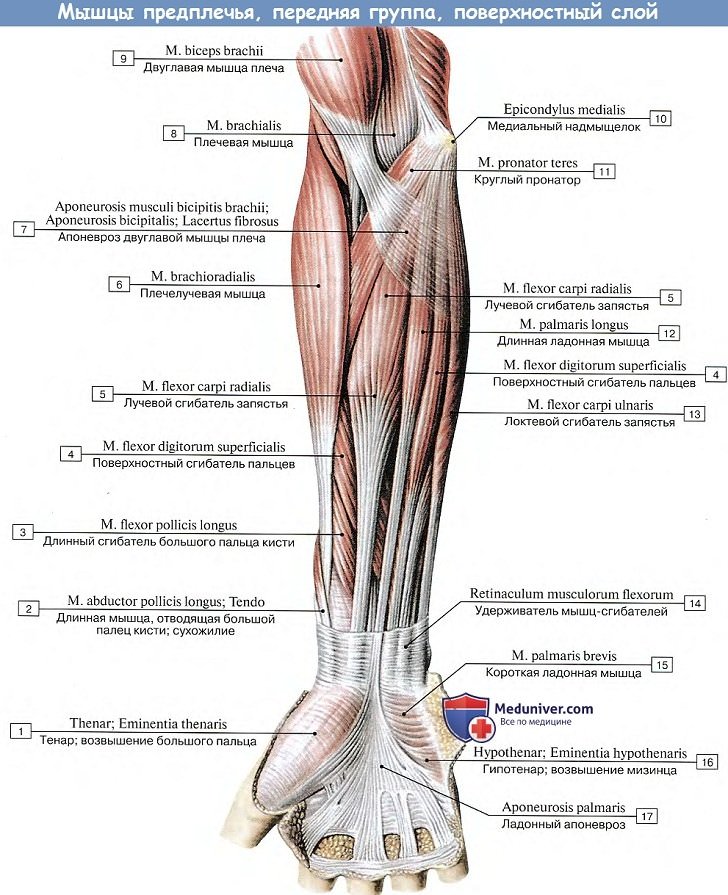
1. M. pronator teres, the round pronator, begins at the medial epicondyle of the humerus and the tuberosity of the ulna and attaches to the lateral surface of the radius just above its middle.
Function. Forces the movement of the forearm and participates in its flexion. (Inn. CVI-VII. N. medianus.).
2. M. flexor carpi radialis, radial flexor of the wrist. Lies along the medial edge of the pronator circularis. Begins at the medial epicondyle of the humerus and inserts at the base of the 2nd metacarpal bone.
Features. Causes the hand to flex and, in conjunction with other muscles, can also retract it towards the radial side. (Inn. CVI-VII median nerve).
3) M. palmaris longus, the long muscle of the hand, It lies medial to the preceding muscle and attaches to the medial epicondyle of the arm. Its short, spindle-shaped belly merges very high into a thin, long tendon, which passes over the flexor retinaculum into the palmar aponeurosis. This muscle is often not present.
Features. Stretches the palmar aponeurosis and flexes the hand. (Inn. CVII to ThI N. medianus).
4. M. flexor carpi ulndris, ulnar flexor of the wrist, lies on the ulnar edge of the forearm, arises from the medial epicondyle of the humerus and attaches to the navicular bone, which is sesamoid to it, and further to the hamate bone (as Lig. pisohamatum) and to the fifth metacarpal bone (as Lig. pisometacarpeum).
Features. Together with the flexor carpi radialis muscle, flexes the hand and also drives it (together with the extensor carpi ulnaris muscle). (Inn. CVII to ThI. N. ulnaris, sometimes N. medianus).
5. M. flexor digitorum superflcialis, the superficial flexor of the fingers, Located deeper than the four muscles described. It attaches to the medial epicondyle of the humerus, to the styloid process of the ulna and to the upper part of the radius bone.
This muscle divides into four long tendons that run from the forearm through the Carpal canal into the palm of the hand, where they run over the palmar surface of fingers II-V.
At the level of the shaft of the proximal phalanx, each tendon divides into two branches, which diverge and form a gap, the hiatus tendineus, for the passage of the tendon, the deep flexor tendon, with which they cross (Chiasm tendinum), and attaches to the palmar surface of the base of the middle phalanx.
Pronation and supination: what they mean
Let's look at some of the terms used by kinesiologists and their explanations. In kinesiology, rotation, pronation and supination are forms of movement of the limbs and the shoulder joint.
Pronation is an inward twisting motion of the upper or lower limbs. This can involve movement of the hand, forearm, and humerus. It can also involve movement of the foot, shinbone, or hipbone.
Let's take the shoulder as an example. If you pull your hand forward so that your thumb is on top and then rotate it 90 degrees inward so that the hand is horizontal, this is called pronation. This type of rotation is performed by a group of muscles called the pronators.
Supination is performed in the same way by the supinator muscles. Only in this case the side edge is turned outwards in the opposite direction.
pronation of the foot
Let's take a closer look at what foot pronation is all about. Regardless of this, the foot can also be pronated. To do this, it must be rotated by lowering the medial part downwards (inwards, towards the axis of the body). The pronator muscles of the lower limbs are stressed. When the foot pronates, the long and short fibula muscles are stressed.

Supination involves rotating the lateral part of the foot outward (away from the midline of the body) with the lower or upper limbs. The principle is the same as pronation, except that the movement is in the opposite direction. It is performed by the supinator muscle group: the longus extensor of the thumb and the tibialis anterior.
How to do hand strengthening exercises

Well-trained hand and wrist muscles will not significantly change the muscular relief of the hand, but are responsible for the quality and safety of fitness training. Lifting weights, pull-ups on bars, dumbbells and rings, and weight exercises become safer when the muscles responsible for wrist strength and rotation are strengthened.
The following exercises are designed to strengthen the wrists:
You can do them yourself with a folding dumbbell by simply twisting the weight from one end. Squeeze the dumbbell with your hand, take a comfortable sitting position and rotate your wrist first to one side and then to the other. This exercise does not require heavy weights and all movements should be performed at a relaxed pace without jerking or breaking. If done correctly, it will not cause any inconvenience.
It not only strengthens the wrists, but also the chest muscles. It is better to use good quality models and follow some rules: avoid excessive relaxation of the hand at the ends of squeezing and releasing; do not help the other hand; pay attention to correct hand movement.
These look like two pincer handles connected by a spring. The handles are pressed together with the hand; when you release it, the spring returns it to its original position.
Dense rubber rings and balls can also be used for fitness exercises. Such products are primarily used in the medical field when a patient needs to be rehabilitated after a broken hand.
Exercises for the hand muscles

In sports programs there are many different exercises for the arm muscles that target the pronators and supinators in one way or another. A classic example is the Zottman exercise:
- Standing with your back straight, grab a dumbbell in each hand and lower them down with your palms facing inward. Keep your elbows pressed against your torso.
- Inhale and as you exhale, lift the dumbbells. When you reach the highest point, turn your arms towards you and tense your biceps. Hold this position for 1 to 2 seconds.
- Staying at the top point, rotate your arms 180 degrees and slowly bring the dumbbells down to your thighs, only turning them inward at the bottom point.
When doing this exercise for the shoulder muscles, do not use heavy weights at once. Perform all actions smoothly, without delay or interruption. No inertial forces should be used and it is important to maintain muscle control throughout the element.
For the following shoulder exercise you will need a barbell with a W-shaped handle:
- Stand upright and grasp the barbell with a reverse grip. Bring your elbows slightly forward in front of your body, shoulders down.
- Exhale and lift the barbell while bending your elbow joints. Only the forearms are involved in the work; the arms above the elbow remain immobile. Perform the movements at ¾ of full amplitude to activate the muscles.
- Slowly lower the dumbbell, fully extending the elbow joints.
The next exercise is a wrist curl with the dumbbell behind your back:
- Stand up straight with the barbell in your hands behind your back, the insides of your wrists facing back. The feet are shoulder-width apart and the gaze is directed forward.
- As you exhale, slowly lift the barbell with your palms slowly facing the ceiling. Only the wrists work, the arms remain stationary.
- Hold the position for a few seconds and then slowly return your hands to the starting position.
Radial group of superficial forearm muscles
1. M. brachioradialis, the shoulder muscle, lies on the anterolateral surface of the forearm, along its lateral edge.
M. The brachioradialis begins on the side of the humerus, between the brachialis and triceps muscles. Its belly then pulls down in front of the radius and becomes a long tendon in the medial part of the forearm, which attaches to the radius above the styloid process.
Medially, this muscle borders the pronator teres and flexor carpi radialis muscles.
Function. Bends the forearm at the elbow joint and brings the radius into an intermediate position between pronation and supination (this is the position that the forearm and hand normally assume when the arms are lowered freely). (Inn. CV-VIII-N. radialis.).
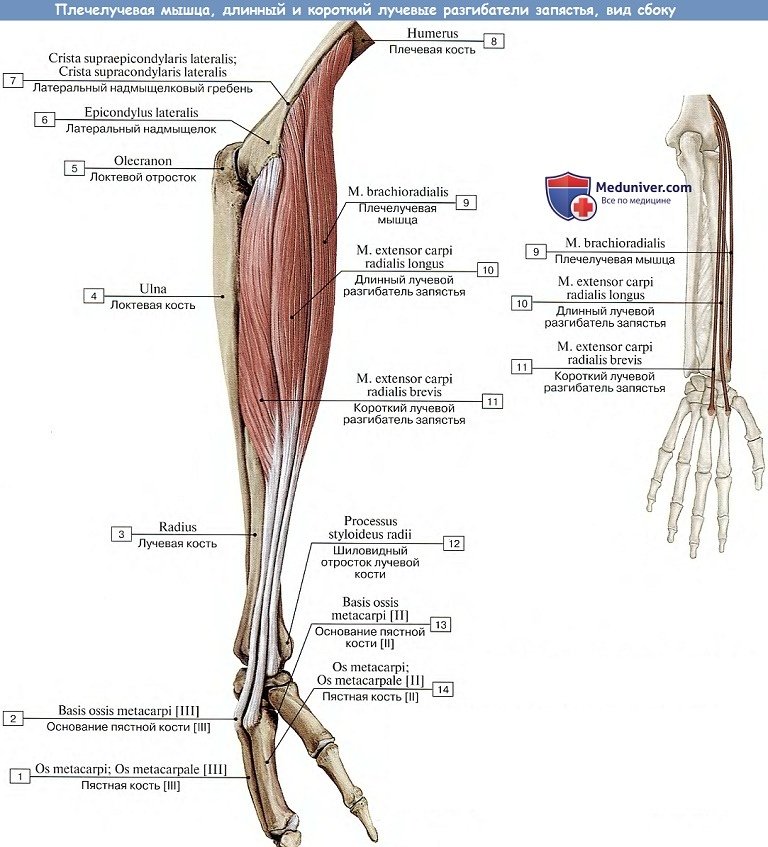
2. m. extensor carpi radialis longus, the long radial extensor muscle of the wrist, lies on the posterolateral surface of the forearm behind the preceding muscle and arises from the lateral edge and lateral epicondyle of the humerus.
In the middle part of the forearm, the muscle passes into a tendon, which runs along the lateral surface of the radius bone, then inserts under the extensor retinaculum and attaches to the dorsal surface of the base of the 2nd bone.
Features. Allows both extension of the hand and abduction (to the radial side) (the latter together with the flexor carpi radialis muscle). (Inn. CV-VIII to N. radialis).
3. M. extensor carpi radialis brevis, the short radial extensor muscle of the wrist, lies behind the long radial extensor of the wrist, begins at the lateral epicondyle of the humerus, goes together with the tendon of the extensor carpi radialis longus, both cross in the distal third of the forearm with the abductor pollicis longus and the extensor pollicis brevis , and in the hand with the tendon of the thumb oblong muscle.
Ulnar group of superficial forearm muscles
4. M. extensor digitorum, the finger extensor, M. The extensor digitorum muscle is located on the entire posterior surface of the forearm and arises together with the extensor carpi radialis brevis muscle on the lateral epicondyle. In the middle part of the forearm, the muscle divides into four bellies, each of which gives rise to a long tendon. The tendons run down to the back of the hand, under the extensor retinaculum through the fourth canal at this point and are then distributed to the four fingers (II-V).
On the back of the hand, near the metatarsophalangeal joints, the tendons are connected to one another by oblique fiber bridges, connexus intertendineus, so that the two middle fingers can only be extended together; the index finger and partly the little finger retain their independence due to the existence of their own extensor muscles.
Each of the common extensor tendons on the dorsal side of a finger merges into a triangular extensor tendon, which is divided into three bundles, the central one attaching to the base of the middle phalanx and the lateral ones to the base of the distal phalanx.
Features. Stretches the fingers II – V and causes the hand to stretch. (Inn. CVI-VIII to N. radialis).
5. M. extensor digiti minimi, extensor muscle of the little finger, It separates from the common tendon of the fingers on the ulnar side. Its long tendon passes through the fifth canal under the extensor retinaculum on the back of the hand to the little finger and unites with the tendon of the common extensor, which leads to this finger.
The function of the comes from the name. (Inn. CVI-VIII is radial nerve).
6. M. extensor carpi ulnaris, the ulnar extensor muscle of the wrist, The tendon, which is adjacent to the common extensor muscle and the extensor muscle of the little finger, begins with these muscles at the lateral epicondyle of the humerus and also at the posterior border of the ulna. The tendon of this muscle runs through the sixth tendon canal under the extensor retinaculum and attaches to the base of the metacarpal bone V (tuberositas ossis metacarpi V).
Development of grip strength
Grip strength is often developed in parallel with the above exercises, but sometimes this is not enough. A strong grip is essential for powerlifters and arm wrestlers, but also for other athletes.
Grip is usually developed with static exercises. The weight is taken in your hand and held for as long as possible. They can be performed without special equipment; it is enough if you find a horizontal bar on the sports field. To make the exercise more difficult, try increasing the diameter of the bar; The easiest way to do this is to wrap a towel around it. When the grip is sufficiently developed, you can try using each hand alternately.
One of the best devices for developing a strong grip is the so-called fat bar. If a traditional bar has a diameter of 28 mm, the diameter of a fat bar is twice as large! I think it goes without saying that it is much more difficult to hold such a rod in your hands. But not all gyms have such a bar. What if you really want to try it, or do you have to buy it? Luckily for your wallet, you don't have to buy one because there are special attachments for standard bars - FAT GRIPZ. These handles are very practical, inexpensive, portable and can be easily carried in a gym bag. You can modify any exercise with them. When you perform deadlifts and pull-ups with these pads, you will definitely improve your forearm strength and are guaranteed to have a new experience!
As a static exercise, I recommend holding the bar at this thickness for as long as possible. An excellent exercise is to hold the bar in the clamp, that is, with your fingers. Thick gummed cakes weighing 15-20 kg are well suited for these purposes.
Development of the pronators and supinators
These muscles work at the moments when we turn our hand, e.g. B. when turning or loosening a screw with a screwdriver. With traditional bodybuilding exercises, these muscles are relatively poorly developed. While lifting dumbbells in supination can relieve the strain on the supinators, the situation is much worse for the pronators. In these cases, arm wrestling exercises can help.
It is called 'pronation with...'. and then we choose the type of weight. This exercise can be done with free weights, with a bottom pulley, or even with an elastic band. The essence of the exercise is as follows: Take one end of a wide strap in your fist and fold it over the top of the outside of your hand. Attach a weight to the other end of the band, e.g. B. Pancakes or a cable for the lower body. The pronator work is very similar to the hammer exercise, but in the starting position the arms should be bent almost at right angles at the elbows. In the starting position, the palm faces upwards, the bar is clenched into a fist. Rotate your hand inward while bending your elbow. The wrist must point towards the athlete's head. The elbow can rest on the side of the body or simply be held in weight, but the arm must always be pressed against the upper body. To complete the repetition, the movement must be performed in reverse order.

What are supination and pronation?
To understand what we are talking about here, you need to know the terms supination and pronation. They are often used in books and articles about training.

supination – is an outward rotational movement of a limb or part of a limb. For example, if we supinate the hand at a 90 degree angle to the elbow, the hand moves from palm down to palm up. This is marked with the number 1 in the figure.
It doesn't matter how much the hand is bent at the elbow. Rotation in the direction indicated by arrow 1 is always supination.
pronation – is the opposite of supination – an inward rotational movement. If you hold a handful of coins in your hand and then decide to spill them, you need to pronate.
The use of the terms pronation and supination in relation to the hand is more or less well known. They are particularly popular on bodybuilding forums for training biceps and forearm muscles.
What is WHP?
IPA stands for 'external rotation of the shoulder'. That is, the supination of the shoulder.
IPA exercises are exercises that develop the muscles that externally rotate the shoulder (shoulder supinators).
Why is this necessary?
At the beginning of this article, I drew your attention to learn about muscles and their functions. Read about the muscles that control the shoulder joints:
Shoulder pronation: 1) scapular muscle, 2) pectoralis major muscle, 3) anterior deltoid muscle, 4) dorsalis major muscle, 5) circularis major muscle
Supination of the arm: 1) Biceps brachii muscle, 2) Biceps brachii muscle, 3) Biceps posterior muscle.
If you look closely at the drawing, a lot will become clear. A - front view, B - rear view.

Notice!!! The pronators of the humerus are the two largest muscles in the body - the pectoralis major muscle and the dorsal broadest muscle! And also the anterior deltoid. In training you do nothing other than develop these muscles in every possible way. And what do we get?
Well, here's what we get. Through strength training, the muscles shorten and become noticeably stronger, as well as increasing in size. Have you ever noticed how absurdly long the shoulders of solid bodybuilders are? One reason for this is the penetrating effect of the extended pectorals and broad muscles.
The shoulder joint becomes more and more prone to slight but still noticeable pronation. This is not a natural position and the shoulder joint must be kept in a neutral position, not in supination or support.
Constant pumping of the pronators is the prerequisite for distortion of the normal geometry of the shoulder joints. This can lead to injury. Especially when doing bench presses, deadlifts, pull-ups. One – and a stabbing pain in the shoulder!
What should I do?
1. Include exercises in your training that develop the shoulder supinators. These are EPI type exercises. They primarily work the muscles on the back of the shoulder – the supraspinatus, subscapularis and small circular musculature.
Rotation of the shoulders
In addition to forearm rotation and the biceps muscles, shoulder pronation and supination also play an important role in everyday life and during sports. Why should I pay more attention to the shoulder and its pronators? Because muscle groups such as the pectoralis major and pectoralis major, which are among the largest muscles in our body, serve as pronators of the shoulder and it is these muscles that everyone tries to pump'.
With increased force and volume, these muscles shorten and unwanted shoulder pronation occurs. All this sometimes causes the shoulders of pumped-up athletes to splay to the sides, giving them a very strange appearance. To prevent this, you should also pay a lot of attention to the shoulder followers during your training. These include muscles such as the subscapularis, small circular muscle and posterior deltoid.

What diseases can impaired supination lead to?

Severe hypersupination and especially hyperpronation causes chronic pain in the legs and lower back as well as regular injuries.
Cervical spine problems, headaches and bite problems can arise from the flattening of the foot due to the increased load.
Misalignment of the knee joint relative to the central axis of the body can cause the kneecap to move outward, causing wear and tear of its cartilage.
What diseases do pronation disorders lead to?
A healthy foot is characterized by neutral pronation, a displacement of more than four percent is an anomaly that causes changes in the musculoskeletal system that lead to inadequate load distribution, injuries and, consequently, reduced gait and running performance.
The main function of the muscles and ligaments of the foot is to distribute the load during contact with the ground, provide cushioning and support the bony structure.
Prolonged walking causes pain, and with high flat feet the pain can occur even when standing in one place.
The more pronounced the flat foot, the stronger the impulse that is transmitted to the upper skeleton when walking and running.
The joints, the spine and the base of the skull are put under a lot of strain. To distribute these stresses, the spine is put under greater strain, resulting in weakness and severe wear and tear.
Such changes also lead to nerve entrapment in the spine.
Among other things, the foot can become severely deformed if there is a high degree of flat feet. The consequences can be: reduced gait, leg fatigue, poor blood circulation, swelling and pain in the ankles and changes in the hip and knee joints.
Symptoms of flat feet:
- The inside of the shoes is heavily worn and worn.
- Unusually rapid fatigue of the feet.
- Pain, fatigue, heaviness, cramps, swelling of the feet.
- Swelling of the ankles.
- Difficulty walking in high heels.
- Thickening of the foot.
What is supination?
Supination is a mechanism in the foot that allows it to rotate outward. This compensates for the force of impact on the ground during movement. Supination also serves as a balance aid when pushing off and landing. The supination mechanism provides rigidity to the foot, especially when pushing off, which allows body weight to be distributed.
Pronation is the opposite movement to supination. The outer edge of the foot is raised relative to the support surface by rotating the sole towards the inner arch of the foot.
Pronation and supination occur around the horizontal anterior-posterior axis of the foot.
Download the marathon and half marathon training programs and start training today!
In the normal state of the foot, these two movements complement each other and bring the foot into a neutral position after the movement. However, this is not always possible for every person. In addition to the neutral state described above, both mechanisms can also be present in excess (hyperpronation) and in deficiency (hypopronation, hypersupination). Hypersupination and hyperpronation are causes of chronic foot and lumbar spine problems as well as regular injuries.
Hypopronation or hypersupination of the foot is rare. With these disorders, the grip is shifted to the outer parts of the feet when landing. As a result of this movement, the longitudinal arch (the cushioning point for the main shock load) is not loaded, but is suppressed by the tissue and ligamentous and muscular system of the outer surface of the foot and the joints above it.
This disorder leads to overloading when running for long periods of time and regularly, which leads to damage and pain to the foot. This is the case in people with a varus axis of the heel bone.
Hyperpronation or excessive pronation of the foot
A much more common phenomenon is overpronation or hyperpronation. In this case, the longitudinal arch of the foot either flattens excessively or is initially flattened. This phenomenon is caused by longitudinal flatfoot or valgus alignment of the heel bone axis.
In this condition, the foot does not return to a neutral position after landing, resulting in inadequate musculoskeletal cushioning. Running in a hyperpronated position causes overloading of the ankles and an inward rotation of the shinbone, which also affects the meniscus and the ligaments of the knee joints.

Aids of the muscles
The muscles have tools that facilitate and improve their function: fascia, synovial capsules and muscle blocks.
Fascia is dense connective tissue membranes that surround individual muscles or muscle groups with a sheath. Fascia separates muscles and allows them to contract independently. At the same time, they serve as an anchoring point for the muscle fibers and facilitate the transfer of muscle forces to the bony arms. Synovial sacs are closed cavities filled with a special fluid. They are located between the muscles and the bones, where the greatest mechanical mobility of the tissue occurs. They allow muscles to slide together when contracting. There are many synovial capsules in the area of the knee and shoulder joints. In the area of the wrists and ankles, synovial sheaths surround numerous tendons and facilitate and guide their movements. Blockages occur where the tendon of the muscle changes direction as it passes through the bone.
Vessels and nerves in muscle tissue
Vessels and nerves usually enter the muscle from the inside, more often in one, less often in several places, the so-called muscle gates. In the muscle, the blood vessels branch into tiny capillaries that wrap tightly around each muscle fiber. The blood carries nutrients and oxygen to the muscle. Because muscles have abundant blood flow and are easily accessible, they are one of the most common routes for drug administration into the human body. Through an intramuscular injection, the drug quickly enters the bloodstream and is distributed throughout the body.
The function of a muscle is viewed from a biomechanical perspective. During contraction, the muscle performs mechanical work, which is defined as the product of muscle force and the distance over which the load is moved. The strength of a muscle depends on its cross-sectional area and the number of muscle fibers involved in the contraction. The larger the cross-sectional area of the muscle, the stronger it is. Remember how spectacularly trained biceps (i.e. the strength of the biceps brachii, from the Latin 'biceps') can be demonstrated. musculus biceps brachii) by flexing the arm at the elbow.
The principle of leverage is used to characterize the individual movements and the muscles involved. A lever of the first type is called a balance lever (e.g. balancing the head against the spine), while a lever of the second type is called a power lever (the foot rising to the toes) or a speed lever (the movement of the arm at the elbow ) referred to as. The muscles constantly work against the earth's gravity. From a biomechanical point of view, any movement of the body in space, as well as the maintenance of its posture, is the result of a complex coordination of the contraction of individual muscles and the coordination of the developed muscle strength with the gravitational forces acting on the body. Knowledge of the laws of biomechanics is particularly important for the study of sports and other professional movements.
As a result of training, the number of muscle fibers increases, which become thicker and contain a large number of myofibrils, which indicates a good development of their contractile apparatus. The structure of the nerve endings improves and the blood supply to the muscle becomes better. Training increases the cross-sectional area of the muscle, which leads to an increase in strength. Special exercises on simulators allow the development of specific muscle groups. In this way, the trainee can change the relief of their body and model it as they wish.
Read more:- Pronator - what does that mean?.
- The pronator is in anatomy.
- Anatomy of the supinator.
- The pronator muscle - what it means.
- pronator to.
- These are the pronator muscles.
- pronation and supination.
- The long section of the big toe.