Athletes usually work very hard to develop these particular muscles. Strength training causes these muscles to shorten while increasing their strength and volume. This causes the shoulders in athletic bodybuilders to expand laterally, giving them a somewhat odd appearance. This is because the shoulder joint pronates under heavy loads, which is not a natural position.
- Circular Pronator
- nerve supply
- Clinical Significance
- Neutral pronator
- hypopronator
- development of the flexors
- development of extensor muscles
- rotation and sports
- Arm training and strength training
- differential diagnosis
- Pharmacological treatment
- How to pump the forearm
- Training program for the forearm
- Phase IV (18-24 weeks)
- Criteria for returning to sport
- What is tennis elbow and golfer's elbow?
- Causes and risk factors
- How often should I train my forearms?
- Exercises for the forearm muscles
Circular Pronator
The circular pronator is a muscle (mainly in the forearm) that works with the quadriceps to pronate the forearm (palm-back, considering the anatomical position). It has two insertions, at the medial epicondyle of the humerus and at the ulnar tubercle, and inserts near the middle of the radius bone.
The peripheral pronator has two heads: the humeral and the ulnar.
- The humeral head, which is larger and more superficial, arises from the medial epicondyle crest just above the medial epicondyle of the humerus and from the common flexor tendon. (which originates at the medial epicondyle).
- The head of the ulnar nerve (or ulnar node) is a thin bundle that arises on the medial side of the coronoid process of the ulna and joins its predecessor at an acute angle.
The median nerve enters the forearm between the two heads of the muscle and is separated from the ulnar artery by the head of the ulna.
The muscle runs obliquely through the forearm and terminates in a flat tendon which is driven into a gross indentation in the center of the lateral surface of the shaft of the radial bone, slightly distal to the insertion of the supraspinatus muscle.
The lateral border of the muscle forms the medial border of the triangular epicondyle called the ulnar fossa, located at the front of the elbow.
nerve supply
To stimulate the circadian pronator, the signal begins in the precentral convolution and travels through the inner sac. It continues via the corticospinal pathways through the capsule, midbrain and pons where it reaches the brain pyramids. Upon reaching the pyramids, the corticospinal tracts cross and the signal travels down the lateral corticospinal tract until it reaches the ventral horns of C5, C6, C7, C8, and T1. The signal then travels through the ventral branches and down the root ganglia of C5, C6, C7, C8, and T1 (which together form the brachial plexus). The signal then travels down the median nerve branches of the brachial plexus, stimulating contraction of the round pronator, causing pronation of the arm.
Clinical Significance
Round pronator syndrome is one of the causes of wrist pain. It's a type of neurogenic pain.
- Patients with round pronator syndrome present with median nerve numbness with repeated pronation/elevation of the forearm and not with elbow flexion and extension.
- Premature fatigue of the forearm muscles is evident during repetitive weight-bearing movements, especially during pronation.
- The EMG may show only a slight reduction in conduction velocity.
- Despite the anatomical proximity, patients with round pronator syndrome do not have a higher incidence of AIN
- Other places with compressive changes:
- Strothers' ligament
- Lacertus fibrosis
- FDS of the proximal arch
- Rare causes such as consecutive tendon transfers in radial paralysis
- Positive Tinel's sign in forearm, not wrist
- Negative result of the Phalen maneuver
- Dysesthesia of the triangle of the hand
- Pain on resistance in pronation
- Forearm pain when resisting isolated flexion of the PIP joint of the long and ring finger
In C5 te patients with traplegia or radial nerve palsy, the circular pronator tendon, known as tendon transfer, can be redirected to the short wrist extensor tendon to restore wrist extension.
Neutral pronator
When running, the outer part of the heel is in contact with the ground. The foot rotates inward about 15 % and achieves full ground contact, allowing it to easily support body weight. The flexion of the foot ensures optimal distribution of the impact load on the ground. This is the natural cushioning effect of pronation. Neutral pronators need little support. Towards the end of the cycle, the push-off is even with the entire forefoot.



hypopronator
Contact with the ground is made with the outer part of the heel. However, the inward deviation of the foot is less than 15 %, which means the movement is less than that of runners with a low or normal arch. In this case, the force of the impact is more on the outside of the foot and is not distributed efficiently enough if the shoes are too supportive. In the push-off phase, the little toes on the outside of the foot are loaded. This is the rarest form of pronation. The photos show the athlete's left foot.



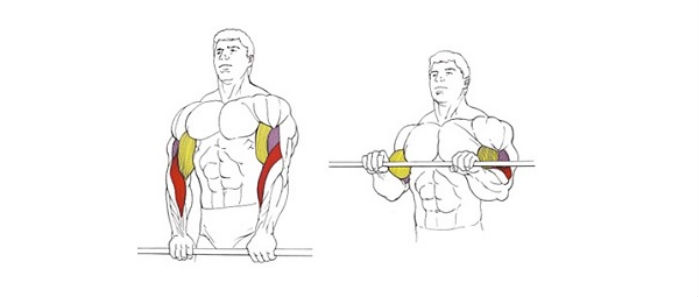
development of the flexors
The flexors are involved in holding a weight, which can be either a gym machine or a simple bag. Since this is very important in everyday life, strengthening the forearms is essential.
The basic exercise for the flexor muscles is the arm flexion with a barbell. This exercise doesn't use heavy weights, although some people can lift over a hundred pounds, but that's pretty much the exception, and that's arm wrestling, but more on that later.
Grab the barbell from below with a narrow grip (about 8 inches), sit down, and rest the backs of your forearms on a bench. The hands holding the barbell should hang off the edge of the bench and be free to move. Perform 8-15 reps while bending your arms with full amplitude. As the bar rolls onto the fingers, the focus shifts to the finger flexors. This can cause painful sensations, so I strongly advise against using heavier weights with this variation! Rolling the barbell on your fingers helps
Strengthens the grip, but to a lesser extent stimulates the forearm muscles at the elbow.
You can also do pull-ups with the dumbbell behind your back. This exercise allows you to lift heavier weights without risking wrist injury and also trains your grip.
Dumbbell curls can also be performed with dumbbells, usually alternating each hand. Dumbbells are easier on the wrists than barbells, but the dumbbells need to be controlled in the hand to keep them from becoming too unbalanced.

development of extensor muscles
The extensor muscles are more demanding than the flexor muscles. These muscles are small in themselves, but still add volume to the forearms. Exercising them is important to keep your wrists healthy.
The largest contributor to the volume of the upper forearm is the brachioradialis muscle. These muscles are engaged in all pull-ups, bicep raises, and extensions. However, to train these muscles, reverse bicep curls and hammer presses must be performed. These exercises use moderate weight, technique is key! Don't rock your elbows back and forth, your upper arm must be locked throughout the exercise. For a change, you can also perform the barbell or hammer raises from the bottom block.
To strengthen your finger extensors, you need wrist extensors with weights. These are performed the same way as the squats, but the grips must be shoulder-width apart, similar to the reverse-grip barbell lift. Bracing your forearms and doing wrist extensions. The weight of the dumbbells should be relatively light, about three times less than the incline. Perform at least 10 repetitions per attempt.
rotation and sports
Pronators and supinators tend to be small muscle groups that many athletes are not aware of. How important are these small muscles in body shaping and also in athletic performance? Are they worth paying attention to during training?
In fact, they are very important muscles. Both beginners and experienced bodybuilders should know them. The rotator muscles are directly involved in almost all movements.
The set of muscles responsible for rotation is therefore important in daily life and can be a factor in a successful athletic career. Supinators and pronators are the antagonists of 'rotation'. They are closely related, although they have opposite functions. Interestingly, the pronator muscles are weaker than the supinator muscles.
It is well known that it is easier to tighten a screw (or bolt) than to loosen it (you have to increase the force by pulling your arm back at the shoulder joint). Without well-trained supinators and pronators of the hand, harmonious development of the forearm muscles, which are difficult to pump and require a lot of work, is impossible.
This allows for effective development and strengthening of the shoulder rotation muscles. It's not uncommon for high-performing athletes of impressive size to fall behind athletes of more modest physique but who perform well with rotational training. The rotational muscle group is particularly impressive in certain physical activities, such as rock climbing, floor climbing, and parkour, which often involve the use of rotating arm harnesses.
Modern armwrestlers take the development of the supinators and pronators very seriously, as the strength of those same muscles is key to their victory. In arm wrestling, as in several other wrestling sports, a lot of time is spent training on elbow expanders and spring machines. A similar picture emerges in running, where the fitness of the supinators and pronators of the legs determines success.
Arm training and strength training
Arm training is an excellent addition to developing the forearm muscles and increasing grip strength, which is important for the qualitative and safe execution of strength exercises with barbells and dumbbells, horizontal bar, dumbbells and rings. Of course, the small 'rotators', the adductors of the thumb and the extensors of the radius are not able to increase the volume of the arms. But their harmonious development has an optical and above all qualitative effect (skill/power reserves, a 'steel' grip).
A fairly simple and effective training for the development of hands can be carried out using a special device. The device is similar to a dumbbell, but with weights on only one end of the bar. If the dumbbell is collapsible, it's easy to get the necessary supports (you can use a dumbbell or a metal bar of the appropriate diameter). Wrap your hand around the bar. Sit comfortably and place your hand (forearm) on a table, bench, or knee. Twist your hand with the clamped weight.
Alternate outward and inward movements. Do not use heavy weights for this exercise. Make the rotation evenly. Avoid sudden jerks and stops. If you rotate properly, you won't feel any discomfort. This is the most effective and safest technique. For better grip training, it is not advisable to use auxiliary belts when working with the deadlift.
The basic exercises used are forearm curls, weights such as dumbbells or dumbbells, and working with different types of resistance bands. Professional Captain of Crush (COC) wrist straps and similar third-party products are ideal for this purpose. Shoulder rotation It is worth noting that the pronators of the shoulder joint are quite large muscles: the pectoralis major, the anterior deltoid and the dorsal broad muscle.
differential diagnosis
- Achilles tendon - posterior impingement, bursitis, rebound pain.
- Patellofemoral Pain Syndrome – Patellofemoral Pain Syndrome.
- Elbow joint – rebound pain, distal nerve involvement.
- Rotator cuff – acromioclavicular joint involvement, shoulder and scapular joint instability, articular labrum injury.
Examination includes checking for muscle atrophy, asymmetry, swelling, and erythema. Muscle atrophy is common in chronic disease and is an important guide in determining the duration of tendinopathy. Swelling, erythema, and asymmetry may also be noted on examination of abnormal tendons. Range of motion testing is often limited on the symptomatic side.
Physical examination should include tendon stress tests to reproduce pain and other stress tests focused on assessing the condition of adjacent structures.
Pharmacological treatment
Corticosteroids have a good short-term effect, but they are not justified in terms of medium or long-term results. There is insufficient evidence to evaluate other injection therapies.
It has been suggested that eccentric training accelerates tendon remodeling by forming connections between fibers. What causes the tendon healing associated with eccentric training is not known for certain, but it is believed that the forces generated by eccentric loading are greater than those generated by concentric training.
It is possible that the eccentric loading not only has a positive mechanical effect on the tendons, but also acts on the pain mediators, reducing their presence in the affected tissues. In any case, the positive effects of eccentric exercise are backed up by studies conducted on athletes and people with sedentary lifestyles.
However, there are many questions about the variables that can affect the outcome of the exercise: whether the exercise should be painful, how long it should last, what method of progression to choose, etc.
So far, three basic principles for eccentric training have been formulated:
- Tendon length - if the tendon is pre-stretched, it will be longer at rest and tension during movement should be less.
- Load - by gradually increasing the load on the tendon, one can expect an increase in its strength.
- Speed - more force is required to increase contraction speed.
However, more research is needed to confirm these conditions.
How to pump the forearm
The forearm is the part of the hand that is between the elbow and the wrist. Characteristic of the forearm is that it consists of a large number of small and medium-sized muscles that facilitate the movement of objects. The muscles of the forearm have the following tasks:
- GIBBEN (anterior muscle group);
- SPREAD the forearm (posterior muscle group);
- CLICK (clench fingers);
- supination of the forearm;
- PRONATION of the forearm.
The structure of the bones of the forearm allows for movements in different directions, therefore providing a wide variety of exercises. Inside the wrist are two bones: the radial and the ulnar, which are connected by ligaments and muscles. This physiology allows the radial bone to move around the ulnar bone in a circular motion, known as supination and pronation. Developing the muscles that perform this function will respond with added size. Also, the muscles of the forearm are close to the surface of the skin, and then directly to the bone.

Big muscles are important to us. Why waste your time on something that's hard to train? And in the case of the forearm, it's even harder because there are so many of these muscles. However, a large part copies the function of leadership or develops something that does not add to the volume. For that reason, let's break down the development of the muscles responsible for enlargement.
Radial arm muscle (brachioradialis) – The main muscle that flexes the forearm. It is also involved in the pronation and supination of the forearm. The second most important exercise for reverse-grip arm flexion.
Main Exercises: Biceps raises with hammer and reverse gripWrist flexors (radial and ulnar) These are located on the inside of the forearm and are responsible for the lateral movement of the arm. An additional task is the pronation of the hand (outward rotation).
Most important exercises: Forearm flexion with a straight grip or reverse grip with a barbell (dumbbells, used by trainers).Training program for the forearm
Perform the above exercises at the end of your workout or after the 'biceps'. Do the reverse grip as you do this, as it works well for both the biceps and forearm. Then do forearm flexes and wrist flexes.
- Reverse Biceps Barbell Press 3-4 X 6-12
- Bend forearms with a barbell on a bench 3-4 X 10-20
- Forearm extension with a barbell or dumbbell on one side 3-4 X 10-20
Phase IV (18-24 weeks)
Continue program to maintain or increase strength and/or endurance until full return to activity. This program should be continued until the patient has full unrestricted strength and is able to return to his or her previous activity.
Increase resistance by using heavier dumbbells, thicker expanders, or more provocative positions like overhead movements, overhead movements away from the body.
Increase the speed and/or resistance of the exercises as needed to increase strength during the workout.
Incorporate more functional movement tasks (e.g. using a real hammer or saw). All exercises are performed in a slow progression from 50 % to 75 % to 100 %.
Start with 25 reps, then increase to three sets of 25 reps at each intensity level.
Criteria for returning to sport
What is tennis elbow and golfer's elbow?
However, the pathology can also appear in other groups of people whose work requires regular, monotonous activity with their hands. The disease affects men and women equally and is most common between the ages of 40 and 60.
Tennis elbow occurs with regular, monotonous, stereotyped hand movements. The constant strain and overexertion damages the tendon. The most common injury associated with tennis elbow involves the lateral (outer) epicondyle of the humerus. It is also known as lateral epicondylitis.
Golfer's elbow is very similar to tennis elbow. However, it is associated with damage to the inner (medial) epicondyle of the humerus. Another name for this condition is medial epicondylitis.
Causes and risk factors
Tennis elbow is caused by regular micro-trauma to muscles and tendons. Due to the frequent trauma, the local immunity is not able to trigger regeneration processes in time, and inflammation occurs at the abrasion sites. The symptoms of the disease are aggravated by regular pathological influences.
Particular attention should be paid to tendon health in people with diseases of the musculoskeletal system and metabolic disorders. These people are more likely to develop inflammatory joint disease.
Medial epicondylitis, while less common, affects men of working age. It is most common between the ages of 35 and 50 in athletes and workers whose activities require constant arm flexion and/or rotation. Groups of people who are particularly susceptible to the disease:
In women, medial epicondylitis is diagnosed much less often due to the nature of the activity.
The cause of the condition is constant tendon injury caused by the same type of activity.
How often should I train my forearms?

There is a common belief that the forearm muscle group is the hardest of all muscles and is therefore rather difficult to train. One can disagree with this opinion, since the forearms are not subjected to intense loads during training. A simple weight load is necessary for the development of this group. It has already been mentioned above that the muscles of this group are inferior to the others in terms of size. This has a positive effect on their recovery speed.
That's the theory, but in practice no professional athlete pays more attention to the forearm than other muscle groups. Consequently, it doesn't make sense for any other bodybuilder to do it either. However, the number of repetitions should be increased. That's because the range of motion of the forearm is quite small and the loading time for the muscles is very important. Usually 10 to 20 repetitions are sufficient for a full workout.
Exercises for the forearm muscles

We are now talking about an exercise program to increase muscle mass of the forearm. To increase the strength parameters, which are of great importance in arm wrestling, we need a different program. As already written above, forearm training should be started after the biceps muscles, that is, in the last phase of training.
- Reverse grip raises primarily train the biceps muscles, but also engage some of the forearm muscles.
- Pronator - what does that mean?.
- pronator and supinator muscles.
- The pronator is in anatomy.
- These are the pronator muscles.
- The pronator muscle - what it means.
- Exercises for the triceps tibialis muscle.
- How to determine the type of pronation.
- pronation and supination.