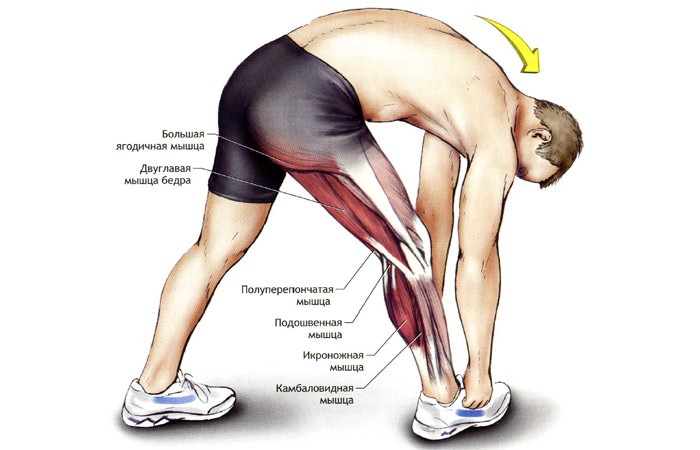
A flat muscle with an elongated shape. It begins at the front and back of the hip bone and ends at the shinbone, twisting and tightening the broad fascia of the thigh along the way. Through engagement of the tibia, the hip bone drives the hip.

- What is foot pronation?
- types of pronation
- hyperpronators
- hypopronators
- Neutral pronation
- Internal
- Iliopsoas
- Lesser lumbar fossa
- Pear shaped
- Internal sphincter
- External
- glutes
- Large
- Middle
- Small
- Twins
- Hip pronation with pelvic rotation
- Stretched legs in a twist
- How do I choose the right running shoes if I know my pronation type?
- pronation of the foot
- types of
- Neutral pronation
- overpronation
- Tension of the ligaments in the hip joint
- Symptoms and treatment
- General information
- Anatomical features of the femoral nerve
- Causes of femoral nerve neuropathy
- Hip flexion
- The contribution of all muscles to hip flexion is not equal:
- Excessive pronation (Excessive pronation).
- Excessive supination
What is foot pronation?
Pronation of the foot is a way of moving the outside of the foot. Pronation is a mechanism that protects not only the joints, but also the internal organs from impacts that can lead to injury. To reduce stress, the arch of the foot flattens as it comes into contact with the ground.
Among the biomechanical processes occurring in a runner's limbs, the most important are pronation and supination of the foot. Pronation can be defined as the ability of the foot to rotate inward during movement. The movement opposite to pronation is called supination. Supination controls the outward rotation of the limbs, while pronation controls the inward rotation. Muscles that rotate externally are called supinators and internally rotate pronators.
Pronation and supination affect both running technique in particular and foot health in general. Correctly determining the type of pronation helps when choosing footwear for sports activities and creating a training plan that will provide maximum benefit. Pronation and supination ensure that the athlete does not lose his balance when pushing off or landing.
Pronation should not be viewed as a single movement. It consists of 3 simultaneous movements:
These concepts are decoded as follows:
Pronation is important when landing on the heel. By observing the movement of the limbs, it is easy to understand a step cycle that consists of 2 phases: transfer and sustain.
types of pronation
There are 3 main groups of people with the following types of pronation:
A foot deviation of more than 4 degrees is considered an anomaly that leads to changes in the function of the musculoskeletal system. The condition poses a risk of injury due to unfavorable load distribution. The affected person is unable to fully utilize his or her physical abilities.
hyperpronators
The foot is characterized by a lowering of the longitudinal arch, which reduces the cushioning effect. Due to the stretched position of the ligaments, the coefficient of free movement is low. Muscle weakness occurs, which contributes to the development of flat feet and increases the load on the spine and knees.
hypopronators
The main characteristic of the foot is a lack of flexion, which leads to inadequate cushioning and results in frequent injuries. During the movement, the following happens: in the first phase of the step, the shin is moved not inward, but inward, and the foot, not resting on the arch, chooses the outer edge as a support. The person is unable to shift their body weight onto the arch of the foot, which is popularly known as 'slouching'.
Neutral pronation
When running, the outer part of the heel is in contact with the ground. The foot rotates about 15 degrees and is in full contact with the surface. This allows the body weight to be supported easily, which is the effect of pronation dampening. Light support is required for neutral pronators. The end of the cycle is marked by an even impression of the forefoot.

Internal
They are also called adductors because they bring the position of the hip bones inwards again.
Iliopsoas
Formed by combining the other two. It is involved in the forward flexion of the body until it rests on the peroneum and rotates outwards. Its functionality can be increased through stretching exercises and squats.
The large psoas muscle is attached to the lumbar vertebrae with one end of five vertebrae and to the iliopsoas muscle with the other end. The iliopsoas muscle has its origin in the iliac fossa and fills it with itself, while the other part is an extension of the greater lumbar fossa.
Lesser lumbar fossa
The lumbar spine begins at the level of the thoracic and lumbar vertebrae and ends at the pubic symphysis, where it is connected to the iliopsoas fascia. It is involved in the flexion of the spine and the tension of the iliac fascia. Externally it looks very similar to the large lumbar fascia, but in cross section it is significantly thinner than this.
Interesting!!! This muscle is very important for the movement of four-legged friends, but it is also found in humans. However, it is not that common and is only present 40 % of the time. This is because humans do not need this muscle because they can walk upright.
Pear shaped
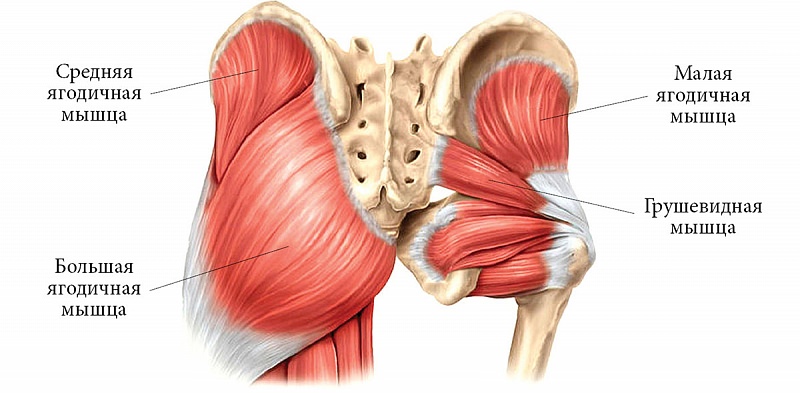
Not pear-shaped, but an equilateral triangle. Its base passes through the ischial foramen and attaches to the sacrum and its narrower part to the trochanter of the thigh. Nearby is the bursa, a slit-shaped cavity that contains fluid.
This muscle is responsible for the external abduction of the hip and the ability to rotate. During a unilateral contraction, only one half of the pelvis rotates inward.
Internal sphincter
Flat shape, with fan-shaped bundles. The wide part attaches to the obturator membrane and the narrow part attaches to the greater trochanteric fossa. It is partially connected to the twin muscles of the outer group. In addition, like most pelvic muscles, it is responsible for supination of the hip in external rotation and for sagittal tilt. At the transition to the pubic bone it forms a locking canal and at the other end it attaches to the trochanteric fossa.
External
The outer group or the outer muscles of the pelvis form the gluteal region.
glutes
They are very large fibrous muscle bundles. They were designed by nature to walk upright on two legs. The task of straightening the hip joint after flexion is not insignificant. The glutes of the pelvis include three muscles.
Large
Very large, at least 2 cm thick. Roughly the shape of a flat rhombus. Consists of several bundles. Has several starting points:
Performs several important tasks and enables:
- to keep the torso upright;
- turning the thigh outwards
- flexion of the leg at the hip;
- to raise the body from lying down.
The size of this muscle has a direct impact on the size of a person's buttocks. It is part of the superficial muscle layer.
Middle
It lies under the covering layer of the vastus muscle. It is slightly weaker but quite thick with bundles in two layers. Looks like an irregularly shaped triangle. The wide part of this triangle borders the crestal part of the iliac crest, and the acute upper angle borders the femur near the greater trochanter.
It is involved in the rotation of the trochanter both inwardly and outwardly. Together with the small and large angles, it is involved in the straightening of the torso.
Small
Externally very similar to the medium and large ones, but much thinner and single-layered. It is attached to the same bones as the middle one and complements its function.
Twins
An upper and a lower twin. The superior epicondyle has the shape of a driving ligament; it begins at the ischium and its end is anchored in the hip socket of the trochanter. It acts as an internal closure and adheres closely to it.
The inferior ligament is similar in appearance to the superior ligament. The inferior ligament attaches to the ischial tuberosities. Like its upper twin, it inserts into the trochlear fossa. In conjunction with the other muscles, they rotate the hips outwards.
Hip pronation with pelvic rotation
Lie flat on your back and rest your arms at your sides. Bend your knees slightly and place your feet wider than your pelvis. Press your back, lower back, and pelvic area into the mat and gently lower your left knee. Point the inside of your left thigh toward the mat. Make sure your lower back does not lift off the floor. Return to the starting position and repeat the exercise with the right leg. This corresponds to one repetition.
Get on all fours, place your hands under your shoulders, your knees under your pelvis, your neck parallel to the floor. Gently rotate your tailbone downward, rounding your lower back. Return to the starting position.
Stretched legs in a twist
Lie on your back, bend your knees and press your thighs into your stomach. Place your hands on your shins. Your head and lower back are pressed against the floor. Extend your right leg across the floor while keeping your hands on your left shin. Then gently return to the starting position and stretch your left leg forward. This way you complete one repetition.
Lying on your back, bend your right knee and lift your leg off the floor. Bring the palms of both hands together under your right knee. Press your lower back and the back of your head into the floor. Extend your left leg forward on the mat. Gently extend your right leg upward and extend your heel toward the ceiling. Stay in this position for 10 seconds. Then return to the starting position. This is a repeat. Do 8 reps in each direction.
How do I choose the right running shoes if I know my pronation type?
The greater the shock load, the more the musculoskeletal system suffers, which means the risk of injury increases. You should choose running shoes for your type of pronation or consider a custom insole. A suitable trainer will improve media support and provide a certain level of movement control. This increases stability and provides adequate cushioning.
Hypopronators benefit from a soft trainer. Since supinators are prone to impact injuries such as stress fractures, choose neutral running shoes with excellent cushioning, such as: B., Acics GEL Nimbus.. The additional gel cushioning reduces unnecessary shock loads. And the gel cushioning throughout the shoe distributes the load evenly.
Choose a trainer for people with neutral pronation. Acics GEL Nimbus i Acics GEL Cumulus are ideal for this sneaker. A soft trainer with this pronation promotes a natural running movement.
Hyperpronators need a stable sneaker. You need maximum media support, structural cushioning and stability. Models like this come into question Acic's GEL-Kayano, Acic's GT-2000, Brooks Ravenna, Saucony Guide.
pronation of the foot
Pronation is the natural movement of the foot that occurs when the foot lands while running or walking. It consists of three components of the cardinal plane: subtalar extension, dorsiflexion of the foot and adduction of the forefoot; These three different movements of the foot occur simultaneously during the pronation phase. Pronation is a normal, desirable and necessary part of the gait cycle. Pronation represents the first half of the stance phase, while supination initiates the progression phase when the heel begins to lift off the ground.

Illustration of the pronation and supination of the foot from an anatomy textbook
- 1 types
- 1.1 Neutral pronation
- 1.2 Excessive pronation
- 1.2.1 Causes
- 1.2.2 Consequences
- 1.2.3 Prevention / Treatment
- 1.2.3.1 Orthopedic measures
- 1.2.3.2 Type of footwear
- 1.2.3.3 Tape
- 1.2.3.4 Shoe lacing
- 1.2.3.5 Barefoot Walking
types of
The normal biomechanics of the foot absorb and control events throughout the gait cycle, with the foot being flexible (pronation) and rigid (supination) in the different phases of the gait cycle. When weight is placed on the foot, pronation of the sole, dorsiflexion of the ankle, and adduction of the forefoot occur. Pronation should not occur after the final stages of midfoot alignment as the normal foot must then supinate in preparation for forefoot pronation.
Abnormal pronation occurs when the foot enters supination or pronates excessively during a normal phase of pronation. For correct forward movement of the foot, approximately four degrees of pronation and supination are required. In the neutral position, the foot is neither pronated nor supinated. If the foot pronates or supinates during the support phase of the gait cycle when it should be in the neutral position, there may be a biomechanical problem.
To simplify the selection of corrective shoes, three types of pronation are distinguished: neutral pronation, overpronation and underpronation.
Neutral pronation
Some pronation, also known as eversion, is natural during normal body movements. Neutral pronation occurs when the foot experiences normal, healthy pronation rather than excessive or inadequate pronation. During a healthy movement, a larger area of the toes is involved in the push-off than during an unhealthy movement. In neutral pronation, the weight of the body is distributed relatively evenly across all toes, with slightly greater load being placed on the big toe and second toe, which can carry a greater load.
overpronation

overpronation
People with overpronation tend to push off almost exclusively from the big toe and second toe. As a result, the footprint is not evenly distributed across the entire foot and the ankle has difficulty stabilizing the rest of the body. In addition, an unnatural angle is created between the foot and ankle and the foot protrudes unnaturally. Even people with normal pronation often have an angle between their foot and ankle, although it is not as large as that of people who bend too quickly. When pronation is correct, the weight of the body is distributed evenly across the entire foot.
Tension of the ligaments in the hip joint
Excessive strain on the hip ligaments is one of the main causes of hyperextension. Severe overstretching of the hip joint ligaments can be caused by sudden jumps, flexions, or extensions. People with a sedentary lifestyle are more prone to these injuries because the ligaments lose their elasticity.
Children, elderly patients and people suffering from obesity, diabetes and high blood pressure are at risk. Postural curvature and unhealthy habits can also play a role.
Other possible causes of hip dislocations include:
- sports or home injuries;
- Prolonged walking on uneven ground;
- training without preparation;
- Improperly performed physical exercises;
- deformities of the hip and lower leg;
- Incorrect positioning of the foot during movement.
It is much easier to prevent ligament injuries than to treat them after the fact, so be aware of situations that can lead to injury. However, if it cannot be avoided, it is important to act quickly to avoid complications.
Symptoms and treatment
In order to recognize the injury in time and initiate treatment, it is important to know the most important symptoms:
- Pain in the gluteal region, lower back, and groin: It sometimes occurs immediately after the event, but more commonly occurs with repetitive exertion (walking or squatting);
- slight stiffness of movement caused by a reflex spasm;
- Discomfort when sitting or walking: numbness or tingling;
- difficulty moving the hips from side to side;
- Cracking or grinding noises when turning a bent limb - accompanied by pain.
If all of these symptoms occur together, a trauma surgeon should be consulted immediately to recommend treatment.
First and foremost, the damaging effect on the ligaments should be eliminated. For this purpose, orthoses selected by the doctor are indicated. The duration of use (usually two weeks) depends on his recommendations. This period of time is just enough for the joint to heal. You should also protect your back more. To limit mobility, an elastic bandage (spike bandage) can be placed on the thigh.
For a mild sprain (first degree), cold compresses may be applied the first day after the injury to reduce swelling and pain. The next day, warming compresses, UHF and other physiotherapeutic methods to improve blood circulation can be used. Special ointments and nonsteroidal anti-inflammatory drugs (NSAIDs) are also used to relieve pain and swelling, but it should be borne in mind that these drugs have many side effects. You can start exercising a week later.
If first aid is provided in a timely manner and rehabilitation is monitored by a doctor, conservative treatment will allow the ligaments to return to normal function even with a second degree sprain. However, this requires a lot of time (about two months) and effort. The specialist may prescribe muscle relaxants, painkillers, calcium supplements, etc. In some cases, surgery may be necessary.
General information
Femoral neuropathy was first described in 1822 as 'inflammation of the anterior sacral nerve'. Today it is one of the most common variants of mononeuropathy of the lower limbs. Although femoral neuropathy has been studied for nearly 200 years and is quite common, in some ways it is still an unknown condition. Lack of awareness among both general practitioners and some neurologists means that femoral neuropathy is often treated as a vertebrobasilar pathology (root syndrome, myelopathy, etc.) or as a manifestation of polyneuropathy. This is facilitated by a variety of symptoms, ranging from purely sensory disturbances to predominantly motor dysfunction, depending on the location of the lesion.
Anatomical features of the femoral nerve
The femoral nerve (N. femoralis) arises from the three lumbar vertebral roots L2, L3 and L4, which unite to form a single nerve trunk. This runs between the iliopsoas major muscle and descends to the inguinal ligament, under which it exits at the front of the thigh, where it divides into a cutaneous (sensory) and a muscular (motor) branch as well as a popliteal nerve. In the iliopsoas segment, the femoral nerve innervates the muscles between which it runs. Their function is the flexion and supination of the hip joint and, when the hip is fixed, the flexion of the lumbar spine, allowing the body to bend forward.
Muscular branches arising from the femoral nerve after passing under the inguinal ligament innervate the muscles responsible for hip flexion and knee extension. The cutaneous branches provide sensation to the anterior and slightly inner surface of the thigh. The saphenous nerve separates from the femoral nerve near the inguinal ligament, runs anteriorly along the thigh, then takes a medial direction and enters Gunter's adductor canal, from where it runs along the medial side of the knee joint, where it forms a popliteal branch that innervates the anterior surface of the patella. The saphenous nerve then runs along the medial edge of the tibia and foot, reaching the base of the big toe. It provides sensitivity to the shin skin on the front and middle surfaces and the skin on the medial edge of the foot.
Causes of femoral nerve neuropathy
The pathology of the femoral nerve at the level of the ilium is often caused by compression of the femoral nerve as a result of muscle spasm or bleeding from the lumbar muscle as a result of overload or trauma. Less commonly, neuropathy of the femoral nerve is caused by retroperitoneal hematomas or tumors (sarcomas, lymphomas). Hematomas can occur in hemophilia, thrombocytopathies and thrombocytopenia; as a complication of anticoagulant treatment in thromboembolic diseases, especially in patients with an abdominal aortic aneurysm. Cases of femoral neuropathy secondary to nerve damage following appendectomy, ureteral and renal surgery, as well as bursitis and iliopsoas abscesses have been described.
Compression of the femoral nerve near the inguinal ligament can be caused by lymphogranulomatosis of the groin, an inguinal hernia, compression of the nerve by the inguinal ligament during prolonged forced standing on the thigh (including during surgery). Nerve damage can occur during hip replacement surgery, surgical treatment of a hernia, etc.
The occurrence of femoral neuropathy at the level of Gunter's canal is observed when the adductors of the thigh, which form the canal, are overstretched during professional or sports activities. Less commonly, a muscle strain occurs as a result of instability or abnormality of the knee joint. Iatrogenic neuropathy can develop as a complication of knee surgery.
Isolated neuropathy of the subscapular branch of the femoral nerve is often idiopathic but may also be associated with thrombophlebitis, varicose veins, and repeated minor trauma to the knee.
Hip flexion
The muscles that cause flexion of the hip joint include:
1. Iliopsoas muscle–The iliopsoas muscle Consists of three parts: M. greatus, M. iliopsoas and M. scapularis.
- He bends and extends his hips.
- When the hip is fixed, it flexes the spine and pelvis in relation to the hip.
- The small psoas muscle stretches the pelvic fascia.
2. the Portia muscle – The longest muscle in the human body.
3. Muscle-нbroad fascia muscle The muscle begins at the anterior superior iliac spine and runs downward and backward between the two lobes of the broad fascia to which it is attached. A continuation of the tendon of this muscle is the so-called iliotibial insertion, which forms the thickened part of the broad fascia of the thigh and attaches to the lateral condyle of the tibia.
4. the M. crestis muscle It is located on the front of the thigh.
5. rectus muscle of the thigh (M. rectus femoris) Is one of the heads of the quadriceps muscle (Quadriceps femoris).
The contribution of all muscles to hip flexion is not equal:
- The iliopsoas muscle plays an important role in this movement. Due to its attachment point being far away from the joint and its relatively close attachment point, even a slight tension causes a flexion with a large amplitude.
- The effect of the rectus femoris and hamstring muscles can be observed when the point of application of force is on the shinbone and the shinbone is stationary.
- The flexor function of the parietal muscle is more pronounced when its adductor function is blocked by the tension of the adductors.
- Human anatomy (with basics of dynamic and athletic morphology): A textbook for physical education. – 14th ed. / Edited by BA Nikityuk, AA. Gladysheva, VF Sudzilovsky. – Moscow: Sport, 2018 – 624 p., ill.
Excessive pronation (Excessive pronation).
Excessive pronation overpronation ) causes the foot to continue rotating after hitting the ground instead of initiating the push-off phase. This creates excessive tension in the foot, shin, and knee and can cause pain in these areas. Those who run this way experience excessive wear on the inside of the shoe, which leans inward when standing on a flat surface. Knee joints and flat feet can be the cause of this problem.
What can be done to correct excessive pronation? It is advisable to wear shoes that are straight or have a slightly emphasized curve. Special shoes that have a high level of running stability, a high-density sole and other anti-pronation properties are ideal. The wear level of the shoe should be checked to see if progress is being made. Since this abnormal parameter causes muscle tension and stiffness, stretching exercises should be performed.
Excessive supination
Excessive supination (i Sweating) causes insufficient rotation of the foot after impact with the ground. This creates excessive tension in the foot and can cause iliopsoas syndrome, Achilles tendonitis, and plantar fasciitis.
Runners with very pronounced foot curvature and heavily strained Achilles tendons are prone to this problem. The shoes are increasingly worn outwards; when standing on a flat surface, they tilt outward.
To correct problems caused by excessive supination, you should wear shoes that are appropriate to the problem, perhaps in a way that allows the foot more freedom of movement. The flexibility of the inner midsole area of the shoe is also important. Runners with this condition should perform targeted stretching exercises for their calves, hamstrings, quadriceps, and lumbar spine.
- pronation and supination.
- How to determine the type of pronation.
- What is pronation and supination?.
- pronation.
- Pronation and supination in anatomy.
- Syndrome of the tibial nerve.
- These are the pronator muscles.
- Sneakers with hyperpronation.