If the hollow foot cannot be completely corrected during the operation, the wound is sutured, a plaster cast is applied and the operation is repeated after 3 weeks to complete the correction.
- Base of stability or pivot point (characteristics of the foot)
- types of feet
- etiology
- symptoms
- Etiological factors
- RDN, posture and walking
- The role of the RDN in standing
- The role of the RDN in walking
- Measurement with blocks
- pronation
- Natural running.
- How to tell if you have hyperpronation
- Treatment of hypo- and hyperpronation of the foot
Base of stability or pivot point (characteristics of the foot)
The human skeleton consists of 205 bones, 52 of which belong to the foot. Why so many? What functions does the foot fulfill? How is it structured? Which foot deformities are possible? I will try to answer these and other questions in this article. The human foot is a unique creation of nature. It is difficult to say at what stage of evolution it arose, but among all living animals no other has anything comparable. Both the front and rear limbs of animals have more or less the same function of either supporting or grasping. They are therefore structured similarly. In humans, however, the functions of the lower and upper limbs differ significantly.
Due to the need to completely free the upper limbs. Two diametrically opposed tasks await our feet.
The first is to provide stable support, that is, to be firm, solid and monolithic, like a horse's hoof.
The second is the need for mobility, for agility, for the ability to adapt to the terrain. The solution to this contradiction was the unique design of the vault, in which different zones fulfill different functions.
This is my favorite picture, I always show it to patients with foot pain and deformity.

The main bases A, B, C, the base of the 5th toe and the base of the first toe, respectively. The architectural features of the foot are the internal and external longitudinal and transverse arches AC, AB and CB.
A feature of the architecture of our foot is the different functions of the inner longitudinal arch.
The outer longitudinal vault (load) and the transverse vault mainly have a supporting function. They are reinforced with straps and usually only flatten under heavy loads when carrying something heavy. These arches remain intact under normal loads.
The internal, elastic longitudinal arch is strengthened primarily by the short muscles of the foot and shinbone, allowing it to act as a shock absorber by flattening the arch and rotating the foot inward (pronation). When walking on an average hard surface, the human foot experiences an overload of 18-20 g, the shin absorbs only 6-7 g, that is, a healthy foot absorbs about 70 % of the load, the rest is absorbed by the cartilage of the joints and spine caught, and ultimately the head receives no more than 1 g.
types of feet
Modern man has the worst attitude towards feet, both men and especially women. In nature, human feet were happy and free from all ailments.
The ancient (atavistic) foot (Fig. 91, view of the bones), also called 'pes anticus' by scientists, resembles the feet of prehistoric people with a large gripping toe that has wide contact thanks to the metatarsal bones and the widely spaced toes to the support surface. As civilization encased feet in more or less comfortable footwear, they were forced to adapt. The fashion in the meantime, especially that of women's shoes with pointed and narrow heels, is simply catastrophic (Fig. 92, foot bones in high-heeled shoes). This is where the fact known by the barbaric name 'hallux valgus' (big toe valgus) comes into play:
the first metatarsal bone, distal to the second metatarsal bone (metatarsus varus or adductus), is pushed inward (toward the heel) so that the big toe points obliquely forward and inward a; this leads to an abnormal protrusion of the head of the first metatarsal, at the level of which the shoe rubs, leading to exostosis b and later to callus formation, commonly called 'bunion', which can become inflamed; the second metatarsal bone is significantly longer than the others, so it represents the main load in the final phase of the kick, causing overload and pain at its base; stress fractures occur; the fifth metatarsal is severely protruding, resulting in valgus deformity of the fifth metatarsal. Sam is pushed strongly inwards c (towards the heel) together with the little toe; this imbalance is quickly perpetuated by the shortening of the joint capsular ligament, the lateral displacement of the sesamoid bones d and the flexor tendons e, which reinforces the imbalance; the thumb displaces the intermediate fingers (Fig. 93) and even sits over the second toe. The thumb displaces the middle fingers (Fig. 93) and even sits over the second toe; the fifth toe undergoes a reverse deformity, the 'quintus varus', further reducing the space for the middle toes and increasing their hammer-shaped deformity (Fig. 94), with callus formation on the plantar side of the proximal interphalangeal joints; the clawed middle toes compress the heads of the metatarsal bones and lower them, causing a protrusion of the front arch of the foot - a protrusion of the foot.
etiology
The exact cause of this phenomenon is not known; it is often due to weakness or hypertonicity of the musculoskeletal system.
- meningitis;
- Poliomyelitis;
- Charcot-Marie-Tooth syndrome;
- Spinal dysraphism (a musculoskeletal malformation characterized by partial incongruence of the tissues along the spine);
- CEREBRAL PALSY;
- Friedreich's disease;
- muscular dystrophy;
- polyneuropathy;
- New growths in the spinal canal.
Curiosities.
There are known cases in which burns or fractures have been identified as the cause of a hollow foot.

In medicine, several types of foot lesions are distinguished:
- Posterior – failure of the muscle (triceps) occurs, causing a lesion in the back of the arch of the foot. The work of the ankle flexors causes the foot to flex, causing the heel to sink below the anterior compartment;
- The intermediate form is a rare form of pathology arising from contractures of the soleus muscles. It often develops when shoes with soles that are too stiff are worn regularly;
- Forefoot - the foot is forced into flexion and the support during movement is distributed to the phalanges of the toes, the heel is higher than the forefoot. As the disease progresses, the heel bone is rotated inward, resulting in severe deformity of the foot.
All deformities are characterized by a redistribution of load to the heel and metatarsals. The ICD-10 code is Q66.7.
symptoms
The first symptoms of hollow foot are fatigue after walking for a long time, pain in the ankle and foot. Patients report difficulty choosing comfortable shoes and the inability to walk in high-heeled models.
- Deformation of the phalanges of the toes in the form of hammertoes;
- calluses and corns on thumb and little finger;
- Severe pain in the ankle joint;
- High arched foot on visual inspection;
- Stiffness of the foot.
With polio deformity, the patient has difficulty walking, a wobbly gait, and visual examination of the leg reveals muscle weakness and unilateral paresis.
In cerebral lesions, the clinical picture is reversed: the muscles are tense and tendon function is increased. The pathology is characterized by a unilateral lesion, while in congenital malformations the deformity develops bilaterally and progresses rapidly in childhood during the growth period.
In Friedreich's disease, cavus foot in adults is characterized by a tendency to progression and affects both limbs. On examination, ataxia and decreased tenderness are noted, and gait is altered.
Specialist opinion!!!
If symptoms are mild, it is difficult to determine the cause. A child's hollow foot is often influenced by external factors and genetic predisposition. The children refuse to stand on the affected foot and avoid long walks.
Etiological factors
- Idiopathic developmental anomalies.
- fractures.
- Trauma to the epiphyseal endplate before skeletal maturity.
- degenerative diseases.
- Legg-Calve-Perthes disease.
- Tumors or neoplastic lesions.
- infections.
- Shortening of the soft tissues.
- contractures of the joints.
- weakness of the ligaments.
- axial curvatures.
- Biomechanics of the foot (e.g. excessive pronation).
RDN, posture and walking
The role of the RDN in standing
Check whether the patient uses specific compensation to compensate for height differences.
- If the leg is left uncompensated, the anterior and posterior hip bone axes may be lower on the side of the shortened leg, which can result in pelvic tilt and/or scoliosis.
- Increased muscle activity in multiple muscle groups.
The role of the RDN in walking
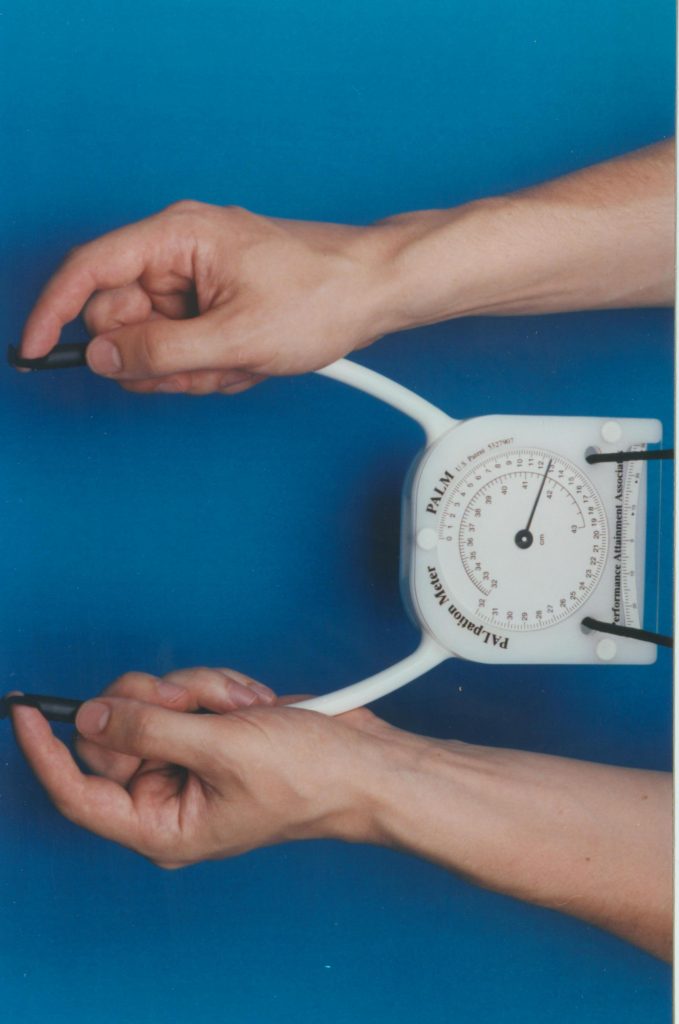
The PALM is a reliable and reliable instrument for measuring height differences in the pelvic area. It is convenient, cost-effective and a good alternative to radiological measurements!
Measurement with blocks
The patient stands with 10 cm between the feet, the knees are extended and the body weight is evenly distributed between the legs. The clinician places his hands on the anatomical structures on two sides: the posterior superior iliac spine (PIA), the PVPO or the iliac crests on the right and left sides. The clinician now visually assesses whether there is a difference in length and, if necessary, places a 0.5 cm long wooden board under the shorter leg. This should be done until these anatomical structures are at the same level (with the total thickness of the boards corresponding to the RDN).
Although the reliability of this approach is highly dependent on accurate measurements by the clinician, this method has demonstrated excellent results in terms of consistency of results between well-trained clinicians and medical students. Confounding variables reported in the literature include pelvic asymmetry, abnormal leg alignment, obesity, joint contractures, scoliosis, and inaccurate measurements.
pronation
To choose the right running shoes, you simply need to know what pronation is and what type of pronation you have.
Pronation is the biomechanical movement of the foot during walking and running: When the foot contacts a surface, the arch of the foot absorbs the shock load by gradually flattening (like a spring in a car). At the same time, the foot turns slightly inwards, also to absorb the load and give additional momentum to the next step. Depending on the walking position of the foot, several types of pronator can be distinguished. For this purpose, manufacturers produce different models and series of running shoes.
There are some pretty simple ways to determine what type of pronation you have. The first is to see where the sole of your running shoe rubs as you run, and the second is what's called the 'wet test'. This test involves wetting the foot and placing it on a clean, dry piece of paper (preferably a dark color) for a few seconds. The wet impression you leave will tell you what type of pronation you have.
There are three types of pronation:
– Neutral pronation (normal pronation)
Normal pronation is the normal cushioning of the foot in which the load is distributed primarily on the middle part of the foot. For neutral pronation, it is advisable to choose 'Cushioning' sneakers, which is the English term for 'Normal'. For long training runs (15+km) there is the option of choosing 'support and stabilization' shoes, which support the foot towards the end of the run.
– Hypopronation (underpronation)
With underpronation, the sole area of the foot is subjected to stress on the outside, which leads to less cushioning of the foot and increased stress on the joints and knees. The 'Normal Cushioning' running shoe category is also recommended for athletes with poor calf cushioning. Look for models with a sole made from a single molded unit (e.g. Asics FuzeX) rather than a composite with different levels of cushioning.
Natural running.
Natural Running shoes are lightweight running shoes that do not limit your movements with corrective and supportive technologies, but do not help you in any way. They usually have very flexible and thin soles with minimal cushioning. We recommend these shoes for short runs on soft surfaces (dirt, grass, etc.) to strengthen the ankle and for competitions.
How to tell if you have hyperpronation
Before determining whether you or a loved one is suffering from hyperpronation, you should choose a method to determine it. The simplest and most accessible method is to examine old shoes that the patient has worn for at least a month. It is worth taking a look at the sole and you will notice how the foot stands when walking. The most stubborn and trampled areas are the footprints. If they are on the inner edge, hyperpronation occurs. If the main footprint is on the outer edge, the patient has hypopronation.
The second method is the wet footprint. Take a piece of paper without the footprint and wet the foot. Stand on the piece of paper and trace the wet footprint with a pencil while it is still there. This allows you to assess the uniformity of weight distribution on the surface of the sole.
The third method is that the knee joints move horizontally when a person squats. If the knees converge inward, hyperpronation is present; if they diverge outward, hypopronation is diagnosed. With normal pronation, the knees maintain their position when doing a deep squat.
It is important to know that only an experienced orthopedic surgeon can diagnose hypo- or hyperpronation if it is minimal, using special measuring devices. In domestic conditions, only an excessive deviation from the norm can be detected, which can be seen with the naked eye. It is therefore highly advisable to visit an orthopedist at least once a year and have your foot diagnosed. Early detection of abnormalities and their correction leads to a lower risk of osteoarthritis of the large joints of the lower limbs.
Treatment of hypo- and hyperpronation of the foot
Before hypo- or hyperpronation can be corrected, the possible cause of these pathological conditions must be determined. Once all pathogenic factors are eliminated, correction can begin.
Treatment of hyperpronation is carried out using conservative methods. These can include therapeutic exercises, electromyostimulation, laser correction, osteopathy and massage. For severe muscle fiber disorders, acupuncture, physical therapy, etc. may be indicated.
Treatment of hyperpronation of the foot with a special therapeutic gymnastics complex in combination with massage sessions gives positive results. However, it is necessary to develop an individual program of physical exercises. During the examination, the doctor must determine which muscles are weakened and which need rest. Based on these findings, a treatment plan is created.
Hypopronation of the foot is treated in the same way. First, a complete diagnosis is made, and then the doctor gives recommendations for eliminating the pathogenic factors. This includes completely replacing the shoes you wear every day. Wearing favorite shoes or boots that are already comfortable will inevitably cause the foot to assume an abnormal position when worn. In this case, treatment of hypopronation or hyperpronation will not bring positive results.
It is important that you follow all of your doctor's recommendations. Book your free initial appointment with an orthopedist at our chiropractic clinic now. During your visit you will receive all individual recommendations for your further treatment.
Doctor of medicine, chief physician of the clinic
Read more:- How to determine the type of pronation.
- pronation.
- pronation and supination.
- What is pronation and supination?.
- Sneakers with hyperpronation.
- What is a neutral pronation?.
- Pronation and supination in anatomy.
- These are the pronator muscles.