After all the necessary intra-articular manipulations have been carried out, a competent trauma surgeon or orthopedist carries out a repair (plasty) of the collateral ligament of the lateral knee joint. An autograft (the patient's own tendon) is used to replace the injured ligament. The transplant is prepared in a special way and inserted through the bone canals. This reconstructs the anatomy and restores the function of the knee joint. In the post-surgery period, rehabilitation therapies are undoubtedly important to regain full range of motion and adequate muscle tone. After a period of convalescence, the patient can resume his usual sporting activities with almost no restrictions. In modern surgery, biocompatible and biodegradable fixation devices are used, which improve the quality of the subsequent MRI examination and the quality of the diagnosis (even modern metal fixation devices can be used in MRI examinations, but cause very strong interference with the magnetic tomography Signal).
- fibula
- blood supply
- Development
- function
- Construction
- Vascularization
- Treatment of the collateral ligament in the knee joint
- Surgery for collateral ligament injury
- rehabilitation
- Prognosis and return to sport
- Symptoms of injury
- diagnosis
- Inflammation of ligaments in the knee
- Inflammation of the ligaments of the foot and ankle
- There are two types of ankle cysts:
- Treatment of bone cysts
- Dosage and Administration
- Overdose.
- Levomecol or Vishnevsky ointment. What is better?
- Analogues
- Sources
fibula
The fibula is the leg bone on the side of the shinbone, with which it grows together from above and below. It is the smaller of the two bones and the thinnest of all long bones in relation to its length. Its upper limb is small, located on the back of the tibial head, below the knee joint and is excluded from the formation of this joint. Its lower limb is slightly inclined forward so that it is in the plane anterior to the plane of the upper limb; it projects under the shinbone and forms the lateral part of the ankle joint.
This bone is made up of the following components:
- Lateral ankle joint
- The intercondylar network that connects the fibula to the tibia and forms the syndesmotic joint
- The superior tibiofibular joint (tibiofibular joint) is the joint that connects the lateral condyles of the tibia to the head of the fibula.
- The lower tibiofibular joint (tibiofibular syndesmosis) is formed by a rough convex surface on the medial side of the lower end of the fibula and a rough concave surface on the lateral side of the tibia.
blood supply
The blood supply is important for the free tissue transfer of the planina ng, as the fibula is usually used for the reconstruction of the mandible. The trunk is supplied in the middle third by a large nutrient vessel from the periosteal artery. It also receives blood supply from its periosteum, which receives many small branches from the periosteal artery. The proximal head and epiphysis are supplied by a branch of the anterior tibial artery. When removing bone, the middle third is always removed and the ends are retained (4 cm proximal and 6 cm distal).
Development
Ossification of the fibula occurs from three centers, one for the shaft and one for each end. Ossification begins around the eighth week of intrauterine life and progresses to the limbs. After birth, the extremities are cartilaginous.
function
The fibula does not carry much weight (mass) in the body. It runs behind the lower end of the shinbone and forms the outer part of the ankle joint, providing stability to this joint. It has notches for some ligaments that give them strength and increase muscle strength. It offers starting points for the following muscles:
 Muscle attachment points (front view) Muscle attachment points (front view) | 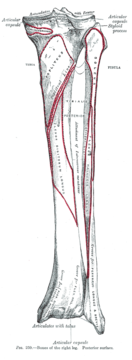 Muscle attachment points (rear view) Muscle attachment points (rear view) |
| muscles | directions | Approach |
| Biceps femoris muscle | Approach | Head of the fibula |
| Biceps muscle of the upper arm (Extensor hallucis longus) | origin | Medial side of the fibula |
| Biceps longus muscle (extensor digitorum longus) | origin | Proximal side Medial side of the fibula |
| Fibularis tertius | origin | Distal part on the medial side of the fibula |
| Fibularis longus | origin | Head and lateral side of the fibula |
| Fibularis brevis | origin | Distal 2/3 of the lateral side of the fibula |
| Simple muscle (soleus) | origin | Proximal 1/3 of the posterior side of the fibula |
| Tibialis posterior muscle | origin | Lateral part of the back part of the fibula |
| Long flexor muscle of the big toe | origin | Posterior part of the fibula |
Construction
The bone is made up of the following components:
- Lateral ankle joint
- Intercondylar ligament that connects the fibula to the tibia and forms the tibial joint (syndesmosis)
- The superior tibiofibular joint is the articulation between the lateral condyle of the tibia and the head of the fibula.
- The inferior tibiofibular joint (tibial syndesmosis) is formed by a rough convex surface on the medial side of the lower end of the fibula and a rough concave surface on the lateral side of the tibia.
Vascularization
Vascularization is important when planning free tissue transfer because the fibula is often used for mandibular reconstruction. In the middle third of the trunk there is a large supply vessel from the periosteal artery. It also receives blood supply from the periosteum, which receives many small branches from the periosteal artery. The proximal head and epiphysis are supplied by a branch of the anterior tibial artery. When harvesting bone, the middle third is always removed and the ends are preserved (4 cm proximal and 6 cm distal).
The fibula is ossified by three Centers ossified, one for the shaft and one for each end. Ossification begins in the body around the eighth week of fetal life and extends to the limbs. After birth, the extremities are cartilaginous.
Ossification begins in the lower extremity in the second year of life and in the upper extremity around the fourth year of life. The lower extremity, ossified for the first time, fuses with the body at the age of twenty; the upper extremity grows together at the age of twenty-five.
Treatment of the collateral ligament in the knee joint

First aid should be administered immediately and consists of strict limitation of weight bearing, elevation of the injured lower extremity, cooling of the injured area and early transport of the injured person to a specialized treatment facility. An orthopedist/traumatologist will examine the injured knee joint, order x-rays, and, if a fracture of the lateral (outer) plateau (condyle) of the tibia is not confirmed, recommend magnetic resonance imaging (MRI) of the knee joint. The quality and speed of the diagnosis have a significant impact on the treatment outcome. Examination and advice on treatment strategies must be carried out by a competent physician with extensive experience, as isolated injuries to the lateral (external) complex are relatively rare and all structures of the knee joint must be carefully examined for possible collateral damage.
The number of damaged structures in the knee joint determines the treatment strategy. A tear of the lateral collateral ligament cannot be treated without surgery, unlike e.g. B. a tear of the medial collateral ligament. This is achieved by moving the collateral ligament away from the soft tissues of the joint and making it more isolated.
Surgery for collateral ligament injury

rehabilitation
How quickly knee joint function can be restored after posterior collateral ligament reconstruction depends on whether or not the cruciate ligaments have been damaged. The injured leg must not bear any weight for four weeks and an orthosis must be worn for at least three months. Active rehabilitation programs that do not involve complete immobilization of the knee joint in the postoperative period are indicated.
Behind the head of the fibula lies the oculomotor nerve, which can be injured during both trauma and surgery. To avoid damaging it, the surgeon must move it out of the way. Chronic pain, instability and weakness of the knee joint may occur.
Prognosis and return to sport
If the ACL injury is repaired immediately after the injury, the prognosis for varus joint stability and return to sport is favorable. In the case of long-term injuries, the prognosis is also favorable if attention is paid to load distribution during reconstruction.
This article is intended only to provide comprehensive information about the disease and its treatment tactics. Remember that self-treatment can harm your health. Get medical advice.
Symptoms of injury
An injury to the internal knee stabilizer is accompanied by a characteristic clicking sound and severe pain. The joint at the point where the ligament attaches swells, mobility is limited and hemarthrosis can develop within a few hours. In the case of an isolated partial tear, there is a small amount of bleeding into the joint area. A complete rupture of the tibial plateau results in massive swelling, a hematoma, and excessive mobility (instability) of the knee.
Long-term (chronic) injuries are characterized by frequent cracking of the joint, pain of varying intensity, stiffness due to flexion contractures, functional blockages and subluxations.
diagnosis
To clarify the nature of the injury and make a final diagnosis, the following examinations are carried out
- medial stress test (detection of ligament insufficiency)
- X-ray in 2 projections (exclusion of an intra-articular fracture)
- COMPUTED TOMOGRAPHY
- MRI
- Aspiration puncture (in case of hemarthrosis)
- diagnostic arthroscopy
MRI is considered the most reliable, safe and informative method. The high-tech imaging procedure not only enables the precise localization of an medial ligament sprain or tear, but also provides an objective assessment of the condition of all surrounding soft tissue structures.
Reconstruction of the knee joint: material from the specialists of the RM movement laboratory
Download detailed rehabilitation program
Inflammation of ligaments in the knee
The femur, shinbone and kneecap form the knee joint. The ligament connects and secures the bones and includes the following components
- Collateral (side) ligaments – tibia and fibula;
- Posterior ligaments – tendons, arch ligaments, medial ligaments, collateral ligaments and patellar ligaments;
- intra-articular – the cruciate ligaments and the transverse knee ligament that connects the meniscus.

Any of the components of the knee joint can be affected by ligamentitis. The disease is often accompanied by subcutaneous bleeding with hematoma formation. Post-traumatic ligamentitis often develops as a result of blood accumulating around the ligament apparatus. Knee ligament inflammation is often chronic. Acute cases are much rarer and usually occur in connection with certain infectious diseases.
Inflammation of the collateral ligaments of the knee joint is often found in young people with an active lifestyle and in competitive athletes. Inflammation of the internal collateral ligament of the knee joint is the most common. Injuries result in partial tearing of the connective fibers that make up the ligaments. Injuries can also cause a complete tear. Injuries to one of the inner collateral ligaments of the knee joint are often accompanied by inflammation of the other ligament as the other ligament is increasingly stressed.

The diagnosis is made with the help of an ultrasound examination. While these parts of the ligament system normally have a uniform structure, are thin and smooth, when damaged they thicken, swell and cracks can be observed. With severe trauma, the fibers in the projection of the inflamed collateral ligament lose their clear contours, their echogenicity is reduced, their structure is heterogeneous, only one attachment point on the bone is clearly visible, far from the site of the tear.
Inflammation of the ligaments of the foot and ankle
The ankle joint is a block-shaped, uniaxial connection between the distal ends of the tibia and the talus. Its attachment occurs through the collateral ligaments of the ankle joint, which are grouped into:
- The lateral (outer) group consists of the anterior and posterior ligaments of the talus bone and the calcaneal ligament. These ligaments are damaged in the majority of cases.
- The inner (medial) group consists of the deltoid ligament of the ankle joint and the anterior and posterior parts of the tibial tuberosity.

In addition, the ligamentous system of the ankle joint includes the components that connect the shins to each other. Any component of the ligamentous apparatus can become inflamed, and the frequency of ligamentous apparatus injuries is due to the upright posture. Depending on which group of ligaments is affected, the pain can occur in the side of the foot, the instep, the sole or the ankle. Lateral pain is associated with inflammation of the anterior or posterior talofemoral ligament, while medial pain is associated with the deltoid ligament of the ankle.
The pain can occur with movement or at rest. An ultrasound examination shows exactly which component is affected: The damaged connective fibers are swollen, thickened and have a heterogeneous structure.
The inflammation of the longitudinal ligament, the so-called plantar ligamentitis, is an inflammation of the joint that runs in the middle from the heel bone to the toe bones.

Plantar ligamentitis is accompanied by pain in the arch of the foot when walking and standing, swelling and sometimes numbness in the lower leg. The condition often affects people who spend a lot of time on their feet, such as athletes or salespeople. Uncomfortable shoes and the anatomy of the arch of the foot can also cause inflammation.
There are two types of ankle cysts:
- Simple or solitary. Almost always affects the long bones. More common in boys aged 10-15 years.
- Aneurysm. In contrast to the solitary cyst, the cavity is filled with blood. It is quite rare and occurs most often in girls between the ages of 10 and 20.
The causes of bone cysts are not yet fully understood. It can occur as a result of trauma (sprains, falls, bruises, etc.). People suffering from rheumatoid arthritis, osteoarthritis and chronic gout are also susceptible. Bone cysts increase the risk of bone fractures because the volume of bones decreases after they form and the bones can no longer withstand the load and break easily.
The disease may be asymptomatic for a long time and may be discovered accidentally during a fracture or during an X-ray examination for another reason. Sometimes a bone cyst can cause swelling and pain.
Treatment of bone cysts
Conservative treatment includes therapeutic punctures (two needles are inserted into the body of the cyst to suck out fluid and inject drugs that reduce destruction of the bone), a plaster cast (if there is a fracture), physiotherapy and a set of physiotherapy exercises. If conservative treatment is ineffective, the patient is treated surgically.
Advanced disease progression and lack of adequate treatment can lead to bone destruction and necrosis, which may result in complete removal of the damaged fragment.
Aseptic bone necrosis – Necrosis is a condition that leads to the death (necrosis) of bone parts and bones in general, due to the interruption or complete cessation of blood flow in a certain area of the bone. Idiopathic aseptic necrosis develops spontaneously without any specific cause. There are complete and partial necrosis of the bone, with a distinction being made between superficial and deep necrosis depending on the location in the bone. The disease progresses in several stages.
Dosage and Administration
For multi-joint diseases and osteochondrosis, the drug is administered intramuscularly (intramuscularly) – 1 ml per day, the duration of treatment is 20 injections (1 injection per day for 20 days) or 2 ml per day, the duration of treatment is 10 injections (1 injection per day for 20 days).
With predominant lesions in large joints — 1-2 ml in each joint at intervals of 3-4 days, intra-articularly. In total on the course – 5-6 injections in each joint.
A combination of intra-articular and intra-articular injection methods is possible.
It is advisable to repeat the treatment in 6 months after consulting the doctor.
Overdose.
In the event of an overdose, the dose-dependent side effects of the drug increase.
If there is an individual intolerance to seafood (sea fish), the risk of allergic reactions increases.
Effects on driving ability and mechanisms. Taking the drug does not affect the ability to perform potentially dangerous activities that require high concentration and rapid psychomotor reactions (driving a car, operating moving mechanical equipment, work of a dispatcher and operator).
Levomecol or Vishnevsky ointment. What is better?
First of all, Vishnevsky ointment and Levomecol, although they are used in similar cases, have a different spectrum of action. Therefore, Vishnevsky ointment is effective when the wound is in the regeneration phase. Therefore, it cannot be used if the wound is abscessed or severely inflamed. Although it contains an antiseptic, the concentration is not sufficient to achieve a bacteria-killing effect. In addition, tar and castor oil stimulate blood circulation in the affected area, making the situation worse.
For this reason, Vishnevsky's ointment is not so effective, since Levomecol, thanks to its antibiotic content, has a stronger antimicrobial effect and accelerates the outflow of pus from the wound. The following distinguishing features are also important, which determine the superiority of Levomecol ointment:
- absence of unpleasant odor;
- higher reparative properties;
- no irritation at the treatment site;
- When treating boils, Levomecol triggers the abscess more quickly and opens the pustule with subsequent wound healing.
But if the patient is helped by Vishnevsky ointment, there is little point in changing it.
Analogues
Analogues of Levomekol ointment have a bactericidal and healing effect. However, the difference lies in the active ingredient of the drug. Analogues include, for example, Fugentin, Levosin (which also has an analgesic effect), Protegentin, Fastin-1, salicylic-zinc paste.
Netran and Levomethil can be considered synonyms, that is, drugs that contain the same substance (but in a higher concentration) as Levomecol ointment. Substitute drugs can only be prescribed by a doctor.
Sources
- Samaeva Ekaterina Valentinovna // Comparative characterization of the features of the course of regeneration processes during transplantation of cultured dermal autofibroblasts and treatment with Levomecol ointment // Universe: Medicine and Pharmacology;
- Cicolia EM, Ivashev MN // PHARMACODINAMICS OF LEVOMECOL // International Journal of Experimental Education // 2016.
Levomecol ointment – an inexpensive and effective drug
The information is provided for informational purposes and does not constitute medical advice or treatment guidance by uteka.ru.
Read more:- Femoral collateral ligament.
- Rupture of the medial collateral ligament.
- Long fibula muscle.
- Long primer.
- The intercondylar joint.
- Collateral ligament rupture.
- How much does knee surgery cost?.
- fibula.