If you go to a regular hospital with these ailments, the prescribed treatment is unlikely to be effective and will not lead to a complete cure, only symptomatic and temporary results. The techniques used in standard orthopedic therapy are not able to eliminate the tension in the iliopsoas muscles. The leg will remain short, the joint will remain locked, and the pelvis will remain twisted.
- What you should know about Blount's disease in children
- Premium care: What modern diapers can do
- What is Blount's disease?
- Infantile Blount's disease
- What types of abbreviations are there?
- Photo gallery of the work
- What are the effects of lower leg lengthening varus?
- diagnosis
- Symptoms of brachydactyly
- Diagnosis of brachydactyly
- Symptoms of shortened limbs ↑.
- How is a leg length discrepancy diagnosed?
- causes and symptoms
- diagnosis
- Normal or sick?
- type of problem.
- Diagnostic methods for the 'short legs syndrome
- How do you treat a short leg?
What you should know about Blount's disease in children

Blount's disease used to be called 'factory leg': it mainly affected children and young people who worked in factories. The disease affects the growth of the bones near the knees and its symptoms are similar to the common leg curvature in children: the limbs look uneven and the child may complain of pain. However, knee joint defects can be serious and permanent.
There are two forms - depending on the age at which the pathology began. The disease in adolescence differs from Blount's disease in childhood. The earlier it is recognized and treated, the better the prognosis. We explain why children today can develop a 'factory foot' and how it is treated.

Premium care: What modern diapers can do
What is Blount's disease?
The bones of the knee have two growth areas. The medial lamella is on the inside of the limb and the lateral lamella is on the outside. In Blount disease (or Erlacher-Blount disease), the growth of the medial, inner lamella slows or stops growing. The lateral (outer) lamella continues to grow, bending the bone. There are two forms of the disease, infantile and juvenile.
Infantile Blount's disease
Crooked, X- and O-shaped feet are common in children under the age of 2, but this curvature usually corrects with growth and movement. However, when a child has infantile Blount's disease, the condition worsens instead of improving. This form only affects the shin (lower leg).
The infantile form is more common than juvenile Blount disease and affects both legs. Infantile Blount disease may resolve spontaneously (but the curve does not correct itself), respond to nonsurgical treatment, or progressively progress.
The threshold age for infantile (also known as early) Blount's disease is 10 years. The most common age for the onset of the process is around 3 years. Knee deformities and other lower limb problems will worsen without treatment, and eventually the child will stop walking.
If the disease is not treated in time, the growth zones grow together, ossify and stop growing. This is called epiphysiodesis, and the process cannot be reversed. Final limb length will be shorter than normal.
Some children with an early onset of Blount's disease may recover without active treatment. However, in most children, the disease progresses, with the relationship to bone deteriorating.
The main risk of exacerbating the disease is overweight and obesity, which develop, among other things, because the child is clumsy in movement.
What types of abbreviations are there?
Congenital shortening occurs in children from a young age and gradually progresses. If parents themselves suspect this problem, then the approximate leg length difference can be determined independently. This is the only thing they can do themselves. The next step is to consult a specialist doctor. Different leg lengths in a child can be a symptom of many different disorders, including serious skeletal disorders. In some cases, urgent medical intervention is required.
The difference in leg length leads to a number of anomalies:
- back pain;
- spinal deformity and pelvic obliquity;
- Deforming arthrosis and aseptic necrosis in the hip region;
- stress fractures;
- impairment of gait and statics;
- Ergonomic disorders, muscular imbalances;
- Accompanying injuries due to a limited ability to compensate.
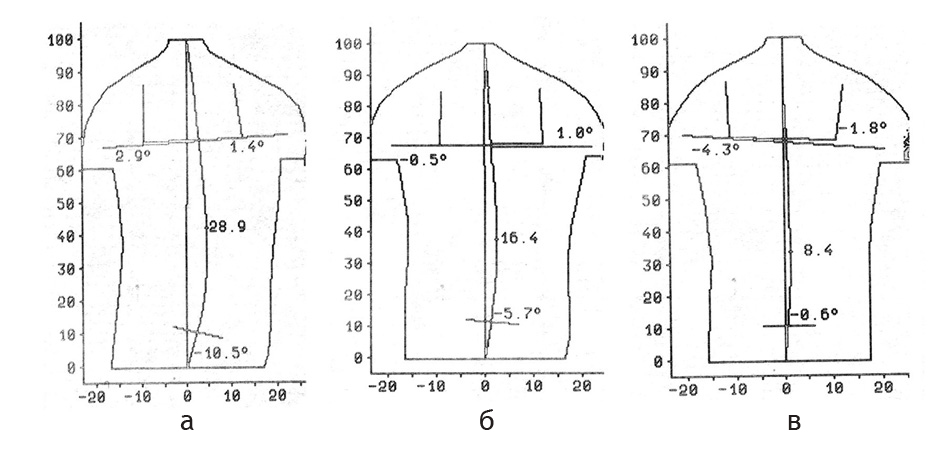
Pelvic insufficiency and spinal deviation at different leg lengths of 6 cm. a – without compensation; b – with compensation of 3 cm; with compensation of 6 cm.
The same difference in leg length affects the child's body more adversely than the adult's body. This is due to the different width of the pelvis. In children, the pelvis is narrower, so the centers of the femoral heads are close to each other, so the pelvic angle and spinal deviation are larger.
The syndrome of abnormalities that develop due to leg length discrepancy is referred to by some authors as 'unequal leg length syndrome'. Left untreated, leg length discrepancy can result in many compensatory functional adjustments (eg, spinal deformities) turning into irreversible permanent deformities (scoliosis).
Photo gallery of the work
14 year old girl. Extension of the right lower limb by 6 cm. Lengthening of the lower limb.
boy, 15 years old. Shortening of the right thigh by 6 cm after trauma. Lengthening of the thigh with an Ilizarov apparatus.
Patient 44 years old. Shortening of the right hip by 5 cm and external rotation - secondary to hematogenous osteitis. Extending the hips and adjusting the axis to the correct position.
The boy is 3 years old. Congenital shortening and valgus deformity of the left hip. Hip lengthening and deformity correction.
Male, 39 years old. Shortening of the right hip by 6 cm after fracture and failed surgery.
What are the effects of lower leg lengthening varus?
The different leg lengths caused by asymmetrical posture lead to the development of adaptive scoliosis, pelvic obliquity, altered spinal alignment and chronic overload of the joints of the lower limbs. This leads to a large number of clinical symptoms such as back and joint pain, headaches and dizziness through to dysfunction of the internal organs.
It is very important to know the type of varicocele diagnosed, since on the basis of this a strictly defined method of treatment is chosen.
- Real (anatomical) - on one of the legs at theactually shorter than the other. This can either be caused by a previous illness (polio, osteoarthritis, etc.) or by trauma - a fracture that has not healed properly. Often there is static scoliosis, which is caused by the different lengths of the legs. The leg length discrepancy in this case is significant – it can be more than 1.5 cm, it is easily recognizable and difficult and time-consuming to correct surgically or mechanically with a pad under the foot.
- Functional (reversible) – a condition in which the actual length of the bones of the lower limbs is the same, but due to anatomical and nervous abnormalities in certain areas of the body, the muscles of the pelvis and lumbar spine contract, pulling the femur up with the leg . This leads to a shortening of the leg length compared to the opposite leg, usually by no more than 1 cm. This change can be corrected with correctly performed osteopathic treatment.
According to the observations of the doctors of our clinic, leg shortening is most often due to chronic reflex muscle tension associated with pelvic obliquity, the tension itself often resulting from changes in position and mobility of areas that, at first glance, have no connection with the pelvis and the pelvis have lower extremities.
Examples of this are the shortening of the leg as a result of a malposition of the lower jaw at the jaw joint after a visit to the dentist or as a result of a functional disorder in the cervical spine area.
diagnosis
When an adult or child is standing, a short leg is not always easy to diagnose as the body adapts to the problem with compensatory scoliosis and a repositioned pelvic bone. In addition, the simple measurement with the centimeter is not always accurate enough and has a tolerance for error.
Therefore, the best way to determine whether there is a leg length discrepancy in the neutral supine or prone position is to compare the symmetry of the most prominent part of the inner malleolus.
Symptoms of brachydactyly
Brachydactyly can be an isolated congenital anomaly, but in some cases short legs are associated with other congenital syndromes. In Down syndrome, for example, in addition to brachydactyly, there are also brachycephaly, short neck, epicanthus, cataracts, tooth misalignment, tongue furrow, heart defects, strabismus and chest wall shape (funnel or keel shape), etc.
Brachydactyly, nystagmus, and cerebellar ataxia are minimal diagnostic features of Baymond syndrome. In Polanda syndrome, the pectoralis major and minor muscles are absent; Brachydactyly, syndactyly, aplasia or amastia of the nipples, rib deformities, etc. are present.
Midface cleft syndrome is characterized by microgenia, ciliary atresia, frontal sinus hypoplasia, brachydactyly, pituitary dwarfism, secondary hypothyroidism, bilateral cryptorchidism, penile torsion, oligophrenia, etc.
In addition to brachydactyly, Aarskog-Scott syndrome presents with hypertelorism, short stature, loose joints, syndactyly, wobbly scrotum, phimosis, cryptorchidism, hernia, and mental retardation.
Brachydactyly itself is associated with abnormal shortening of the fingers and toes, sometimes with flattening or splitting. Depending on the severity of the pathology, brachydactyly can be combined with joint stiffness (symphalangia), syndactyly, polydactyly, and muscle weakness, affecting the normal functioning of the hand or foot. Brachydactyly is often characterized by hypoplasia or aplasia of the nail plates.
Special cases of brachydactyly are ectrodactyly and adactyly. In ectrodactyly, the distal (nail) phalanges are poorly developed; in severe cases the nail and middle phalanges are absent. Metacarpal development is unaffected. In adactyly, the phalanges are congenitally absent and the metacarpal bones are partially or fully preserved.
Diagnosis of brachydactyly
Brachydactyly in a child can be diagnosed prenatally or postnatally. Prenatal diagnosis may include a consultation with a geneticist (if there is a family history of brachydactyly) and a 3D ultrasound scan during pregnancy care at 20-24 weeks. Isolated brachydactyly is not a reason for termination of pregnancy; chromosomal syndromes should be treated on an individual basis.
After birth, the diagnosis of brachydactyly is made by a pediatric traumatologist/orthopedist based on clinical examination and radiological findings (x-rays of the bones of the fingers, hands, toes, and feet). DNA diagnosis is crucial.
Symptoms of shortened limbs ↑.
Symptoms of unequal leg length can be mild or severe. The latter contribute to a significant impairment of the functionality of the body. With moderate symptoms, there is a feeling of insecurity when walking and the risk of frequent falls. One hip gets higher than the other.
The most common symptom is pain:
If If the pelvis is shifted…. If the pelvic obliquity has been present for a long time, the body will compensate for the asymmetry and biomechanical disturbance. Over time, the ligaments, tendons, and muscles will adjust. Therefore, it may take time to heal. Also, abnormal pelvic alignment is the most difficult to correct because it creates a pathological pattern of movement. The longer the pelvic deformity lasts, the longer it takes to restore muscular balance.
Diagnosis of the lower limbs
A leg shortening can usually be determined quite easily. Pay attention to the length of the leg when standing. If one leg seems longer than the other, or if your heel keeps hitting your pant leg while walking, you most likely have short leg syndrome. This pathology is the first cause of the child's posture disorder. If a child has short leg syndrome, they will also develop lower back pain. The pain can spread down the leg to the knee joint and thighs.
Different leg lengths can be well diagnosed with a physical examination. If there is an urgent need to diagnose various lesions in the hip joints or spine, instrumental methods of examination, such as MRI or X-rays, may be recommended.
Treatment of leg shortening
If patients complain of this type of problem in a regular hospital, the prescribed treatment is unlikely to be effective and will not lead to a complete cure, only a symptomatic and temporary result. The techniques used in standard orthopedic therapy are not able to relieve the tension in the iliopsoas muscles. The leg remains short, the joint remains locked, and the pelvis remains twisted.
How is a leg length discrepancy diagnosed?
A leg length discrepancy may not be noticed by parents until the child begins to walk. A routine school screening for scoliosis (curved spine) also helps identify this trait.
To diagnose changes in leg length, doctors first examine the child's general health and medical history. He then performs a physical exam, during which he also observes how the child walks.
The child can compensate for the difference in leg length by walking on the toes of the shorter leg or bending the knee of the longer leg. The doctor can measure the difference between the legs by placing wooden blocks under the shorter leg until both hips are level.
Imaging tests (such as X-rays and CT scans) can also be used to measure the length and bone density of the lower leg. If the child is still growing, the doctor may recommend waiting to see if the leg length discrepancy increases or stays the same.
To monitor growth, the doctor may repeat the physical exam and imaging tests every 6-12 months.
causes and symptoms
Bilateral leg shortening is caused by various genetic disorders. The unilateral form can be caused by various pathologies and diseases:
A slight difference in leg length is often not visible even to the patient and is only detected during special examinations. If the difference in leg length is greater than 3 centimetres, there is a significant pelvic obliquity, which impairs normal walking and causes a limp.
In children, shortening of the lower limbs is usually detected during an examination by an orthopedist. Several external signs (position of the back of the knee, upper pole of the knee, etc.) indicate the presence of an anomaly.
diagnosis
To determine the severity and nature of the pathology, the doctor measures the length of the patient's lower limbs, as well as its individual segments, focusing on the bony protrusions (ankles, knees, etc.). X-rays are also recommended.
Shortening of the lower limbs is treated by orthopedic and trauma surgeons. In the case of a slight shortening, conservative correction (wearing special shoes and orthoses) is indicated.
If the pathology is caused by a dislocation or subluxation of the hip, treatment includes splinting, exercises and massage. In some cases, the dislocation is corrected with surgery.
A major dislocation requires surgery. The most common method of orthopedic foot correction is the use of an Ilizarov brace.
Leg length discrepancy is a serious condition that, if left untreated, can lead to serious joint and spine problems.
- Open daily from 09:00 to 22:00
- All diagnostic rooms are open daily from 08:00 to 22:00.
- The trauma and treatment rooms are open 24 hours a day
- Open daily from 09:00 to 22:00
- All diagnostic rooms are open daily from 08:00 to 22:00
- Trauma and treatment rooms are open 24 hours a day
- Open from 09:00 to 22:00 daily
- All diagnosis rooms are open daily from 08:00 to 22:00
- Trauma and treatment rooms are open 24 hours a day
- Open from 08:00 to 22:00 daily
- All diagnostic rooms are open daily from 08:00 to 22:00
- Trauma and treatment rooms open daily 08:00 - 22:00 daily
- Open from 09:00 to 22:00 daily
- All diagnosis rooms are open daily from 08:00 to 22:00
- The trauma and rehabilitation center is open 24 hours a day.
Normal or sick?
The human body is asymmetrical - that's a fact. So it is not surprising that the length of the legs of a healthy, fit person is slightly different. According to orthopedists, the normal discrepancy is up to 0.5 cm. According to various reports, this occurs in 50-95 % of the population. Those who have disparate limbs don't realize their 'defect' and live their lives to the fullest.
Interesting!!! Foreign researchers conducted a study and examined how people feel about the asymmetry of their lower limbs. Individuals with a leg length discrepancy of 5 mm had no subjective complaints. However, with a leg length discrepancy of 10 mm, around 97 % of the subjects complained about functional hip problems.
The finding of a difference in length of the lower limbs before an endoprosthesis is not surprising. Doctors advise patients to 'realign' their legs during surgery.
Table 1 Degree of leg length discrepancy.
| Length deviation, cm | Possible causes | symptoms and consequences |
| < 1 | Degenerative changes in the hip joint against the background of deforming arthrosis or chronic arthritis. | It causes no symptoms or functional limitations. Note that some professionals consider a 1.5 cm discrepancy to be acceptable. |
| 1-2 | Severe osteoarthritis with ankylosis, functional stretching of the lower limb after hip replacement in the first few months after surgery, improper selection or placement of a hip prosthesis. | Associated with abnormal hip function compensated by reflex muscle tone, pelvic obliquity, and spinal curvature, with no neurological symptoms. |
| > 2 | It occurs as a result of failed hip replacement surgery and can be caused by inadequate rehabilitation during the recovery period. | It leads to pronounced hip dysfunction, spinal curvature and neurological disorders. People with this deformity complain of limping and severe leg pain. |
type of problem.
In many foreign countries, different leg lengths and the resulting lameness are a common reason for complaints against surgeons. In our country, this discrepancy is a variant of the norm. After unsuccessful operations, those affected silently accept the defect or correct it with heel pads or shoe heels.
The most uncomfortable consequence of a leg length discrepancy is the 'fall limp', in which the sufferer abruptly shifts their entire body weight onto the shorter limb. This leads to an abnormal gait rhythm and the development of adaptive postural changes. The consequences are pelvic tilt, curvature, muscle tension and chronic pain in the lower limbs.
Conclusions!!! Leg discrepancy after total hip replacement is an uncomfortable and dangerous complication that often leads to discomfort, reduced function and even disability.
Diagnostic methods for the 'short legs syndrome
The examination and treatment of a suspected short leg syndrome is carried out by orthopedists and podiatrists.

'I would like to draw attention to the connection between leg length differences and the wide range of musculoskeletal and neurological pain that patients complain about,' says Vladimir Nechaev. – I often see anatomically caused leg shortening in patients who come with chronic complaints and back pain. Unfortunately, they are often prescribed expensive and unnecessary equipment and laboratory tests. In the case of conspicuous clinical symptoms, proven and accurate manual assessment methods are of great importance.
The so-called block, block position and block stretching methods have proven to be good diagnostic methods. In the block position method, special plates (blocks) are gradually placed under the heel of the shorter limb. The amount of correction required is determined visually and by palpation.
In the block-flexion method, the flexion test is repeated with the patient standing with feet shoulder-width apart and successive blocks of 2, 4, 6, 8, and 10 mm placed under the heel until a negative flexion test is achieved on the shorter leg . The visible results of this test make it possible to understand the cause of the impairment and then to develop the most effective treatment strategy.
Postural x-rays and other methods of assessing the patient's condition may also be used.
How do you treat a short leg?
Treatment is always individual and depends on the cause of the shortening and the severity of the disease.
Anatomically caused leg shortening can be treated with a lift therapy, in which a special heel strap is placed under the shoe to compensate for the leg length.

The thickness of this insole is chosen individually, can be adjusted when wearing the shoe and can be supplemented with a heel insert.
The best results are achieved when lift therapy is started in childhood. Studies show that in children and adolescents who are fitted with orthoses on the side of the shortened leg, the length of the legs adjusts over time. Lift therapy aligns the base of the sacrum, the pelvis, serves to prevent coxarthrosis, corrects scoliotic symptoms and combats gait disorders caused by asymmetry.
'From my many years of practice, I know that lift therapy drastically reduces pain in many cases and significantly shortens the recovery time,' says Dr. Nechaev. - says Dr. Nechaev.
If the leg length discrepancy is due to functional causes, chiropractic, kinesitherapy, and physical therapy should be included to achieve the proper effect. Lifting therapy can be used for relief for a short period of time until the patient undergoes comprehensive health rehabilitation under medical guidance.
Read more:- How to determine leg shortening.
- The child has a shorter leg than the other.
- How to balance leg length.
- One foot is bigger than the other.
- Feeling that one leg is longer than the other.
- Which human leg is shorter?.
- Shortening of the lower limbs.
- On the short leg.