The main symptoms of shortening of a limb section:
- What is a short leg?
- Useful
- See 'on short legs' in other dictionaries:
- Along the knees
- See what 'on short legs' means in other dictionaries:
- One leg shorter than the other.
- One leg is shorter. How does the orthopedist treat this? Are shoe inserts required?
- etiological factors.
- RDN, posture and gait
- The role of the RDN in standing
- The role of the PALM in walking
- Measurement with blocks
- diagnosis
- Techniques for correcting different leg lengths
- diagnosis
- Treatment of shortened limbs
- Statistical frequency of congenital shortening of the lower limbs
- Classification and symptoms of lower limb shortening
- Who is recommended to use a shoe buckle
- How to choose an orthosis?
- Causes of short legs syndrome
- What are the risks of short toes in children?
- Diagnosis of short legs syndrome
- Who should you contact?
- surgical treatment
What is a short leg?
It's a happy person. Even with a woman as capricious as Fortuna. Is at the short end of the stick.. C. Maksimova, two...He wasn't in the regiment with nobody in the regiment.But he didn't run away from his comrades either. Yu. Tynyanov, Lieutenant Kizhe.
I try to keep up with them [staff officers] myself, don't on a short walkbut within the bounds of official decency. C. Sergeev-Tsenskiy, morning eruption.
As you can see, I got all this information from Timur, who was on friendly terms with everyone at the [police] station. On a friendly basis.. B. Kunin, Kysia in America.
you were friendly with the French President at the time and used her position to hand him a letter. MK, 2002..
– Why, I'm friends On a friendly basis.And I'm happy to stop by for a chat. (Explanation.)
Useful
See 'on short legs' in other dictionaries:
short – Adverb, synonyms: 3 – on friendly terms (4) – on friendly terms (3) – … dictionary of synonyms
SHORT – SHORT, eye, oe; short and (obsolete) short, short, short, short and (obsolete) short; shorter. Ozhegov's dictionary. S. Ozhegov, N. Shvedova. 1949 1992… Ozhegov's dictionary
About short terms - By which. In trust, in a close relationship. In the regiment he was not at loggerheads with anyone, but he did not run away from his comrades either (J. Tynianov. Lieutenant Kizhe) … Phraseological dictionary of Russian literary language
on the short foot - With who. On friendly basis with … Dictionary of many terms
short – Adjective, synonyms: 17 – was on friendly basis (31) – was on friendly basis (17) – … Dictionary of many expressions
short – See… Dictionary of Synonyms
Along the knees
See what 'on short legs' means in other dictionaries:
ON SHORT PAGES – who to be; are in a close, personal relationship of trust. Sometimes it implies an unjustified acquaintance. It means that a person (X) has a friendly relationship with another person (Y) and feels at home with them……… Russian phrasebook
on the short foot – Adverb, synonyms: 3 – on friendly terms (4) – on friendly terms (3) – … Phraseological dictionary
SHORT – SHORT, eye, oe; short and (obsolete) short, short, short, short and (obsolete) short; shorter. Ozhegov's dictionary. S. Ozhegov, N. Shvedova. 1949 1992 … Ozhegov's dictionary.
About short terms - With who. In close, friendly relationships... Dictionary of many terms
short – adj., synonyms: 17 – was on friendly terms (31) – was on friendly terms (17) – … Dictionary of many expressions
short – See… Dictionary of Synonyms
spend time with someone – in a close, friendly relationship. FVH&E … Psychological terms
ON A FRIENDLY BASIS - Who is; in a close, personal, trusting relationship. Sometimes unnecessarily implies a family relationship. Means that a person (X) is on friendly terms with another person (Y), associates with….
on a friendly basis – adjective, synonyms: 17 – was on friendly terms (31) – was on friendly terms (17) – … phraseological dictionary
keep in touch – to be friends, to be friends, to be friends with, to be friends, to be friends, to be friends, to be friends, to be friends, to be friends, to be friends … Glossary of synonyms
One leg shorter than the other.
1) Shortening of the leg (both anatomically and functionally) inevitably leads to a change, ie a twist, in posture. This is completely logical and understandable: the body is forced to adapt and seek balance. In addition to the aesthetic flaw, the incorrect posture leads to a displacement of the internal organs, which usually has a negative effect on their function. In addition, the gait is changed.
2) The shortening of a leg inevitably leads to an increased load on one of the two limbs - usually the shorter one. This in turn leads to joint problems (hip, knee and foot) - osteoarthritis, osteoarthritis and increased joint wear.
A leg shortening in children and adults can be recognized by the following symptoms
– One shoulder is higher than the other
– One shoulder blade is higher and protrudes
- The child's (or adult's) gait is irregular and it hobbles on its feet
– The child seems to jump up.
The presence or absence of these symptoms does not always indicate a shortened limb. In all cases, only a doctor can make an accurate diagnosis.
The answer is: see a chiropractor. Let him find out if a leg is really shorter or if you think it is shorter. If it is shorter, what is causing one leg to be shorter. And if possible, let him fix it. You could also go to an orthopedist.
Shortened legs. How can a chiropractor treat this?
If it is an anatomical shortening - the doctor can distinguish between anatomical and functional shortening - there are usually two possibilities:
The first option. – One leg of the child is shorter than the other.
In this case, the chiropractor must attempt to restore normal blood flow to the short leg - and in many cases, that leg will overtake the healthy leg in the growth process! Two things are most important: the age of the child - the younger the child, the greater the chance; and the degree of damage (usually birth trauma)—the more severe, the worse.
One leg is shorter. How does the orthopedist treat this? Are shoe inserts required?
As a rule, the orthopedist will recommend an insole for the short leg. To balance the support. How justified is such treatment? There are several options.
(a) If the parents do not intend to have their child see a chiropractor but are actually attempting to straighten the child's legs, orthotics can probably be approved in this case. For what reason? To more or less maintain the posture. However, the orthoses have to be worn for life and replaced from time to time;
(b) if the parents want to try to straighten their child's legs and avoid the problems described above, then not using orthotics makes sense.
2. One leg is shorter in an adult or older child. If the child is older than 10-12 years and there is no way to straighten the legs (they have already tried and it did not work), it may make sense to use orthotics to maintain posture. If it's an adult who has lived their whole life with different feet and without orthotics, then in my humble opinion there is no need to put orthotics on them either. Since a whole chain of adjustments has formed in the body over the years, the body as a whole has long since found its balance. If we put an insole under the foot of such a person, we interrupt all these adaptations and force the organism to find a new balance. This can be accompanied by a number of unpleasant side effects (discomfort, joint pain, lower back pain, etc.). This is especially true for middle-aged and elderly people.
How many sessions are required and what are the odds?
In the case of anatomical shortening, the first sessions are carried out at short intervals (about a week), the subsequent sessions every 1-2 months or less frequently if the dynamics are good. The total duration of treatment is at least one year.
The number and frequency of treatment sessions is determined individually. It all depends on the severity of the problem, age and the ability of the individual body to respond to treatment: for some the process is rapid and dynamic, for others it is slow and lengthy. As already mentioned, the chances of success also depend on the age of the child, the severity of the damage and the strict adherence to the recommendations and the schedule.
In the case of a functional shortening, this is much easier and faster. In my practice, treating a short leg usually takes 2-3 sessions.
etiological factors.
- Idiopathic abnormalities.
- fractures.
- Trauma to the epiphyseal endplate before skeletal maturity.
- degenerative diseases.
- Legg-Calve-Perthes disease.
- Tumors or neoplastic lesions.
- infections.
- Shortening of the soft tissues.
- contractures of the joints.
- weakness of the ligaments.
- axial curvatures.
- Biomechanics of the foot (e.g. excessive pronation).
RDN, posture and gait
The role of the RDN in standing
Check if the patient uses a specific compensation that he applies himself to compensate for the height difference.
- If the leg is left uncompensated, the anterior and posterior hip bone axes may be lower on the side of the shortened leg, which can result in pelvic tilt and/or scoliosis.
- Increased muscle activity in multiple muscle groups.
The role of the PALM in walking
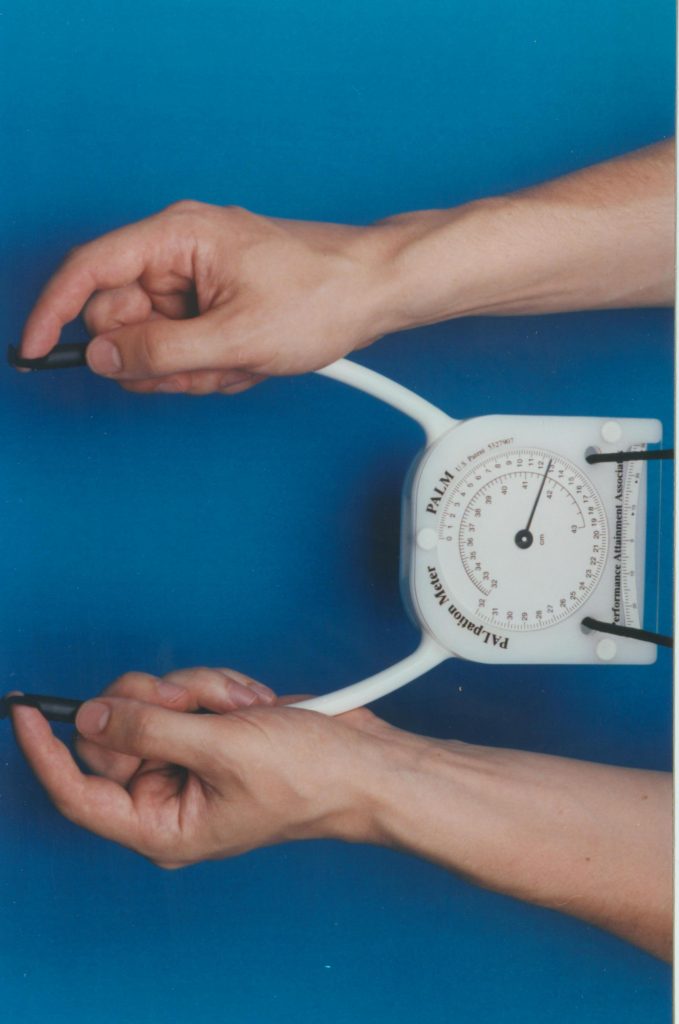
The PALM is a reliable and valid instrument for measuring the difference in pool height. It's convenient, economical and a great alternative to radiological measurements!
Measurement with blocks
The patient stands with the feet 10 cm apart, the knees are straight and the body weight is evenly distributed on the legs. The doctor places their hands on the anatomical structures on two sides: posterior superior iliac spine (PIA), PVPO, or iliac crests on the right and left sides. The clinician now visually assesses whether there is a difference in length and, if so, places a 0.5 cm thick wooden board under the shorter leg. This should be done until these anatomical structures are level (where the total thickness of the boards should equal the RDN).
Although the reliability of this approach is highly dependent on accurate measurements by the clinician, this method has shown excellent results in terms of consistency of results between well-trained clinicians and medical students. Confounding variables reported in the literature include pelvic asymmetry, abnormal leg position, obesity, joint contractures, scoliosis, and inaccurate measurements.
diagnosis
Clinical studies show that the gold standard for determining leg length, spine, and pelvic ring abnormalities is to perform a postural x-ray. These X-rays, which are taken according to a standard protocol (feet stationary, knees locked in a neutral position, and arms positioned appropriately), are evaluated by the physician to provide data on the static functional position of the body. The postural X-ray is always a functional X-ray: the patient's body is placed in a position in which it is loaded with a weight. The X-ray image must be taken with an independent vertical X-ray reference line that is perpendicular to the surface of the patient's footplate.
However, many x-rays taken while standing are not suitable for making an accurate postural diagnosis or for monitoring the patient over time.
Techniques for correcting different leg lengths
Treatment depends primarily on the cause that triggered short leg syndrome. Lift therapy has been shown to be effective in the presence of anatomical factors. In the case of functional deformities, different techniques of manual therapy, physiotherapy, etc. are used on the feet. The most important thing is to use all possible approaches for the different type of deformity, because prescribing heel inserts or foot braces to compensate for different lengths is useless in functional disorders in the long run.
Pelvic alignment by raising the heel on the shorter side of the foot with the help of a special shoe insert, also called lift therapy, dates back to the 19th century. Even then, a piece of cork was placed in the shoes to compensate for the length of the foot. In the case of anatomically caused shortening of the foot, it is advisable to start lifting therapy in childhood. HH Fryette wrote in 1936: 'For the last 15 years I have used heel pads on the short side of the leg on youth up to the age of 14, and each time I have been surprised to see the limbs straighten out in a short time'. Other authors have come to the same conclusions over the years. Recent research shows that with a well-chosen lifting therapy strategy and alignment of the croup base slope, dorsalgia and other symptoms associated with postural abnormalities can be reduced by up to 80 %. The main goal of lifting therapy is the alignment of the base of the sacrum, as well as the prevention of coxarthrosis and the correction of compensatory scoliosis.
When recommending lift therapy, a flexible approach is required for each patient: the thickness of the pillow must be chosen individually, with the possibility of gradually increasing it if necessary. Patient comfort must also be considered: the patient must feel comfortable in the shoe with the instep. A combination of cosock and heel padding is possible.
diagnosis
In order to clarify the severity and type of shortening, the absolute and relative length of the limb, as well as the length of each segment, should be measured, with the visible bony prominences (ankle, upper pole of the patella, condyle of the knee joint, greater trochanter and upper anterior axis of the hip bone) serve as reference points. Measurements are taken with the legs fully extended, with alternate flexion of the hip and knee joints and simultaneous flexion of the large joints of the limbs. Relative and palpable shortenings are determined with special tests.
The list of additional investigations depends on the location and the suspected cause of the shortening. An x-ray of the tibia or hip is indicated for old fractures, tumors and infections. For osteoarthritis, an X-ray of the knee, hip, or knee arthroscopy is done. If soft tissue involvement is suspected, MRI data is used. If necessary, patients are referred to an oncologist, tuberculosis doctor, infectious disease doctor, rheumatologist and other specialists.
Treatment of shortened limbs
The condition is treated by traumatologists and orthopedic surgeons. Slight shortening is usually treated conservatively - the difference in leg length is compensated for with special orthoses or orthopedic shoes. In the case of severe leg shortening, the treatment method is determined individually and depends on the cause of the leg length discrepancy, the patient's age, health status and other factors. The most popular and effective method of surgical treatment of leg shortening is leg lengthening using the Ilizarov apparatus.
The Ilizarov apparatus can lengthen the lower limbs by 8-10 cm and the thighs by 5-6 cm. The increase in segment length is gradual and can last up to six months or more. Placement on the tibia is relatively easy to tolerate as it allows adequate range of motion, does not interfere with joint movements of the limb, etc. Placement on the thigh is more difficult as it severely limits mobility and self-sufficiency. Throughout the treatment period, the patient performs special exercises to prevent muscle atrophy and maintain joint mobility. The functional results are good.
2 Treatment of children and adolescents with orthopedic diseases of the lower limbs / Gafarov HZ – 1995
Statistical frequency of congenital shortening of the lower limbs
Statistically, congenital shortening of the lower limbs ranks first among all diseases of the musculoskeletal system. They occur in one in 50,000 newborns. According to worldwide statistics, shortened limbs account for about 15 % of all musculoskeletal disorders.
The causes of this anomaly are not yet fully understood. It can either be a genetic disorder or external causes (e.g. thalidomide tragedy). Hip shortening is the result of abnormal femoral neck development, insufficient growth of the femur in combination with other problems. Shin splints are an intramedullary pathology resulting from underdevelopment of the bones, muscles and neurovascular bundles of the lower limbs.
Classification and symptoms of lower limb shortening
A distinction is made between real and functional shortening of the lower limbs:
- Real: The problem is related to the leg itself. This means that the bones of the lower limbs (thigh bones, tibia) are shortened.
- Functional: The bones are of normal length, but due to problems in the joints, a different length is created. Often associated with contractures and ankylosis of the hip and knee joints or with scoliosis.
- Mixed: A combination of real and functional shortening of the lower limbs.
With congenital hip shortening, there is not only a change in length, but also accompanying pathologies, which are due to underdevelopment of the skeleton. These include deformities of the femoral neck, dislocations, or subluxations of the femoral head that result in insufficient range of motion. With a strong shortening, the children cannot lean on their leg because it does not reach the ground. Compensatory mechanisms are triggered during growth. The spine curves and the pelvis becomes crooked. The difference in leg length can be up to 23 centimeters. In the course of growth, functional disorders occur and the constant strain causes pain in the healthy limbs.
When the tibia is shortened, patients complain of limping and impaired gait. When the fibula is underdeveloped, support is usually not compromised, but valgus deformity occurs at both the ankle and knee. Complete absence of the fibula can result in complete external dislocation of the foot and significant impairment of gait.
If the tibia is underdeveloped, the limb is usually not supported. The knee joint is not fully developed. Patellar dislocation or complete absence of the kneecap can occur. The flexion and extension of the knee and ankle joints is very limited. This deformity is detected at birth or even during prenatal ultrasound screening.
If the fibula is slightly underdeveloped, the problems may not appear immediately, but only after the age of seven, when parents notice a valgus deformity at the level of the knee, or more commonly the ankle, during an intense period of growth.
Who is recommended to use a shoe buckle
- In the last months of pregnancy;
- Individuals who have a higher than normal body weight;
- To prevent or eliminate corns and calluses on the foot.
- tendon sprains;
- plantar fasciitis;
- Diseases of the spine and joints of the lower limbs;
- different leg lengths (less than 3 cm);
- arthritis, arthrosis;
- heel spur;
- injuries in the heel area of the foot;
- flat feet;
- other foot problems.
- injuries to the sole of the foot;
- microangiopathy and diabetes with ulceration;
- Vascular diseases, in which blood flow in the feet is impaired;
- exacerbation of atherosclerosis.
If one leg is no more than 2 to 3 cm shorter than the other, you can make up the difference by placing a strap under the shorter leg. In this case, do not choose a product made of flexible material such as silicone, as this would overload the foot when walking. It is better to choose a stiffer strap. They are usually multi-layered and have a hard-wearing upper material (natural leather, microfiber).
How to choose an orthosis?
In order to choose the right orthopedic product, it is necessary to consult a doctor. Only a doctor can suggest which heel shoes are most suitable for a specific problem and possibly recommend the appropriate thickness of the insoles (3-12mm). The choice depends on the problem and the goal to be achieved. The special design of the product reduces the risk of heel injuries, prevents corns and blisters, helps reduce pain when walking and corrects foot deformities.
The material of the insoles should be chosen according to the intended use of the instep:
1. Silicone insoles are recommended:
- for Sport,
- with heel spurs,
- after injuries to the Achilles tendon,
- for recovery after fractures,
- With salt accumulation in the joints of the lower limbs;
- For painful heel, knee or ankle joints.
They prevent blisters and broken bones, counteract the development of flat feet and relieve leg fatigue. These products have a clear orthopedic effect, but are quite complicated in design and are not suitable for formal shoes. Silicone is non-allergenic and provides good shock absorption when walking and running (e.g. Cinch ST-41).
2 Gel products are intended more for prophylaxis. They reduce pressure on the heel and prevent spurs, cracks and blisters. These thin and soft insoles can be used with model shoes. They are not suitable for serious illnesses.
3. Leg length correction insoles are used for back and joint problems as well as flat feet. They have a good orthopedic effect, but cannot be worn with all shoes because they are quite wide.
4. Special leather soles with a latex base ensure an optimal microclimate in the shoe and prevent the development of plantar fasciitis. They are also used for different leg lengths. These products have practically no orthopedic effect, but in addition to their excellent ventilation properties, they are distinguished by their high quality and durability.
Causes of short legs syndrome
Leg shortening can have two causes: anatomical and functional. The former can be treated surgically, e.g. B. with an Ilizarov apparatus, but is relatively rare. The functional cause can be treated with physiotherapy and osteopathic techniques.
Anatomical causes include the sequelae of longstanding and irregularly healed fractures, tumors, degenerative diseases, idiopathic disorders, and iatrogenic causes.
Functional disorders result from misalignment or twisting of the pelvis, dysfunction of the sacroiliac joint, differential muscle tension, and differential loading of the limbs. Problems can also be congenital: e.g. B. as a result of birth trauma, which includes joint dislocation or muscle hypertonicity due to various causes. As a result, the bones are equal in length, but the iliopsoas muscle 'pulls' the pelvis towards itself and with it the leg.
Often the disproportion is hardly noticeable - one leg is a few centimeters shorter than the other. Since this is not very uncomfortable for the child at first, many parents limit themselves to purchasing orthopedic shoes.
What are the risks of short toes in children?
A misaligned foot will result in improper load distribution. One foot has to work harder and the other is not used optimally. The sacrum, lower back, and even the torso are twisted. Headaches, inattention and scoliosis can occur. Over time, spinal problems can lead to herniated discs, and all for a not-so-obvious reason: short legs. No orthopedic shoes can prevent this, especially since children (and adults) wear socks, slippers or barefoot shoes most of the time.
The body is a delicate structure in which everything is connected. Problems in one part lead to problems in other parts. The loss of a 'bone' leads to a 'domino effect'.
Diagnosis of short legs syndrome
As previously mentioned, many doctors do not diagnose short leg syndrome, even when the difference is serious. If you have performed the pants experiment at home (described above) and notice a change, you should immediately consult a trauma torpedo specialist. To diagnose this syndrome in young children, one must lay them on their backs and straighten their legs.
[20]
Who should you contact?
Gentle manual therapy is most commonly used to treat functional short leg syndrome. It differs from conventional medicine primarily in that it is completely safe, effective and efficient. Sometimes a slight leg length discrepancy disappears completely in just a session or two. When it comes to correcting leg length, professional chiropractors do not work very deeply, so this technique is suitable even for treating young children.
Slight manifestations of short leg syndrome can be corrected with orthopedic shoes.
For moderate discrepancies, resin foam or orthopedic shoe corrections can be used.
surgical treatment
If short leg syndrome is due to an anatomical cause, the only solution is surgical treatment. With the help of a surgical procedure, the shorter leg is surgically lengthened. This treatment method is used only when there is too much disproportion between the lower limbs and the trunk.
Currently, surgeons can lengthen the leg by 6 centimeters at the lower leg and 10 centimeters at the thigh. The operation begins by severing the skin, tissue, and bone in the leg. The separated pieces of bone are fused together with special spokes, and then fixed from above with a special Elizarov apparatus.
This is just the first step on the road to recovery. Each day, an experienced doctor will then 'pull' the bone fragments in opposite directions by a millimeter. Once the brace is removed, the patient has to go through a tough rehabilitation (remedial gymnastics and physiotherapy).
Structural differences in the legs can be corrected by surgical epiphysiodesis. This intervention aims to correct pelvic tilt, gait and posture errors.
Read more:- The sole in the shoe is responsible for.
- What to wear with short legs.
- One leg is shorter than the other.
- The child has a shorter leg than the other.
- Function of the short fibula muscle.
- Pain in short fibula when walking.
- How to determine leg shortening.
- Which leg is longer?.