It should be noted that in children less than 3 years of age, the displayed fat pad on examination gives false indications of decreased soft arch size and flattening of the internal longitudinal arch.

- Forefoot and toe phalanges
- functions of the foot
- The human skeleton
- clinical picture
- diagnosis
- Skeleton of upper and lower limbs
- Overview of the 'Skeleton of the Upper and Lower Limbs' lesson.
- Conservative treatment of metatarsalgia
- Surgical Treatment of Metatarsalgia (Surgery)
- Surgery for hallux valgus and hammer toe deformity
- Human Foot Tartarus Anatomy Information:
- Which doctors should you see for a metatarsal exam:
- bones of the toes
- Video about the correct anatomy of the foot bones
- treatment of osteoarthritis
- Conservative therapy
- surgical treatment
- Bad osteoarthritis: types, risk factors, symptoms and prevention
- When should I see a doctor immediately?
- The bones of the foot: the tarsal bones
- diagnosis
Forefoot and toe phalanges
The foot is a complex and very important part of the entire human skeleton. It consists of 26 bones, 107 ligaments and 20 different muscles and tendons. The foot is the 'foundation' of the body - it carries the load of the entire body in locomotion.
The foot is made up of the bones that make up the skeleton, the ligaments that move to connect the bones together at their joints, the muscles that move the foot, the blood vessels that carry blood, the nerves that move the making muscles work and the skin covering the foot.
The skeleton of the foot consists of three parts: the tarsus (tarsus), the metatarsus (metatarsus), and the phalanges (phalanges).
The foremost points of the toe phalanges are called the arches of the toes.
The bottom of the foot is called the plantar surface and the top is called the dorsal surface.
The foot is supported at 3 points:
The foot has an arched structure. It has two longitudinal vaults and one transverse vault.
The AC is the inner longitudinal arch (elastic);
Behind the metatarsal bones, in front of the toes, is the widest part of the forefoot, formed by the heads of the metatarsal and toe joints, called the transverse arch (AC arch).
– The internal arch (elastic) is formed by the heel, talus, scaphoid, three cuneiform bones, 1st, 2nd and 3rd metatarsals and is an arch that runs through the entire foot, beginning at the calcaneus tuberosity and ending at the support of the head of the 1;
These bones form a kind of vault, a spring that can flatten and expand.
– The external (weight-bearing) arch of the foot is formed by the heel bone, cuboid bone, 4th and 5th metatarsal bones; it is also arched and runs through the entire foot, beginning at the calcaneus tuberosity and ending at the pivot point of the 5th
The transverse arch is perpendicular to the longitudinal arches over the metatarsal bones.
The arches of the foot can only be considered as separate elements as in reality they are constantly interacting and functioning as a single mechanism.
functions of the foot
The main function of the foot is to support the human body when standing and to help it move.
The foot fulfilled three biomechanical functionsThree biomechanical functions: elastic, balancing and supporting.
function of shock absorption – Cushioning of shocks when walking, running and jumping. It is made possible by the foot's ability to cushion under stress and then return to its original shape. The front, outer and inner padded foot is able to change its shape and move in three planes when the direction of the total load and the shape of the seat changes, so that it moves like a boat on the waves, when the sea ripples'. This is important to catch small irregularities in the ground'.
When the arch of the foot is lowered, the tremor is transmitted more to the joints of the lower limbs, the spine and internal organs, which contributes to their deterioration, micro-injuries and displacement.
equilibrium function – Postural control during movement. This is realized through the ability to move the ankles in three planes and through the numerous receptors in the ligaments. A healthy foot digs out bumps and people feel the surface they are walking on. When bones and joints are realigned, the ligaments deform, affecting motor coordination and stability.
B support function manifests itself in the foot's ability to support the human body by counteracting the vertical load of body weight.
This is the foot's most complex function, as it uses both elasticity and balance.
During walking, all three functions of the foot are constantly being performed.
When the height of the arch of the foot is reduced, all functions of the foot are disrupted.
| The foot should be viewed in a 'foot - lower limb - spine' system. Each joint above depends on the joint below and vice versa in the supporting structures of the body. Foot disorders cause asymmetries throughout the body. The figure shows the main anomalies of flatfoot alignment. Flattening of the foot leads to a cascade of compensatory changes and overloads of the lower limbs, pelvis and spine. The flattening and outwardly deviating foot results in external rotation of the tibia and compensatory internal rotation of the thigh. This reinforces the X-shape of the knees. On the other hand, by positioning the body segments over the foot, the condition of the arch of the foot can be improved. The foot plays an important role in forming posture. | 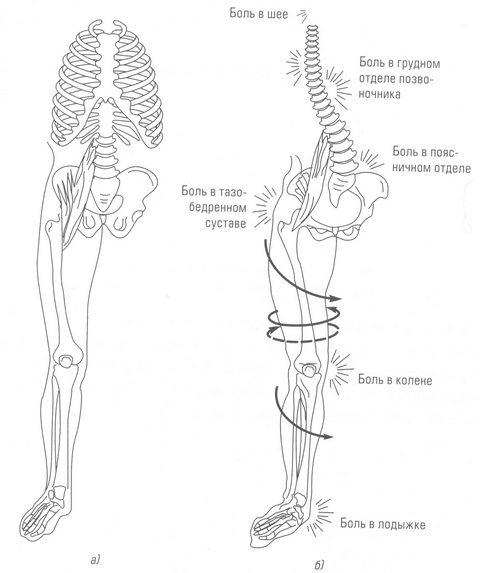 | |
| Changes in the upper body with foot deformities: | ||
| (a) normal foot | b) foot deformities | |
The human skeleton
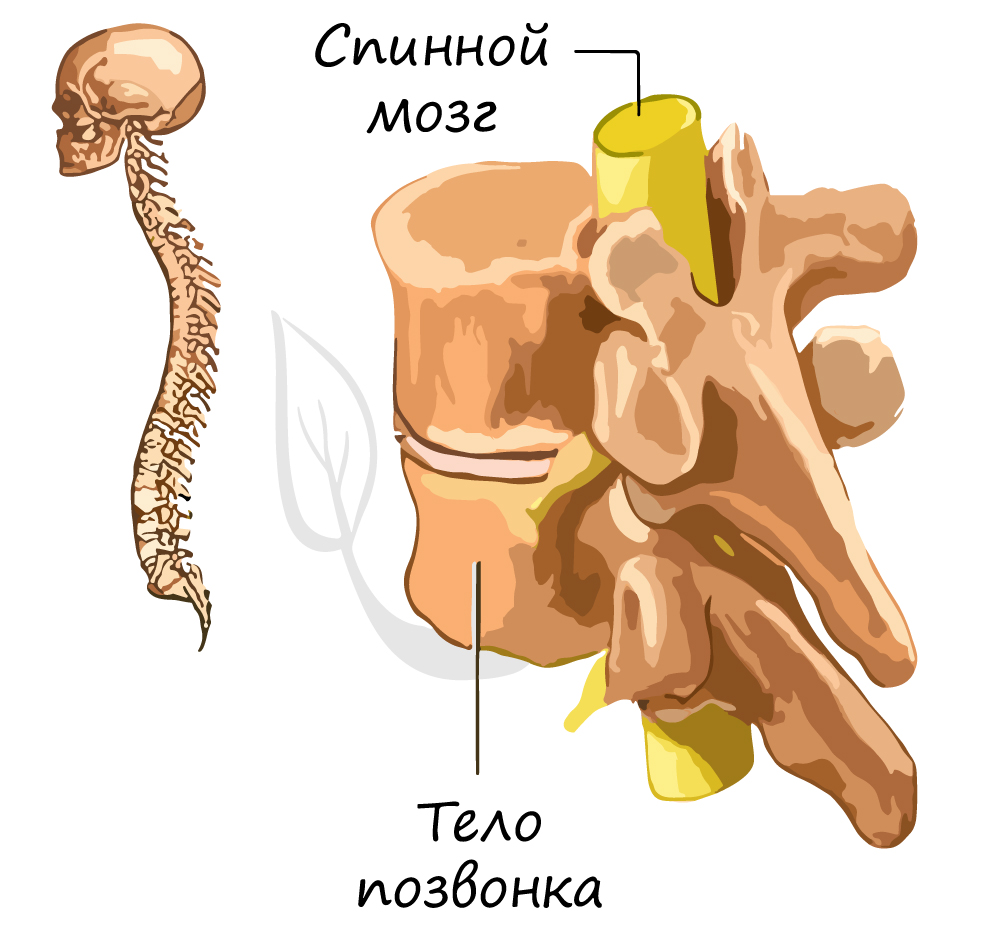
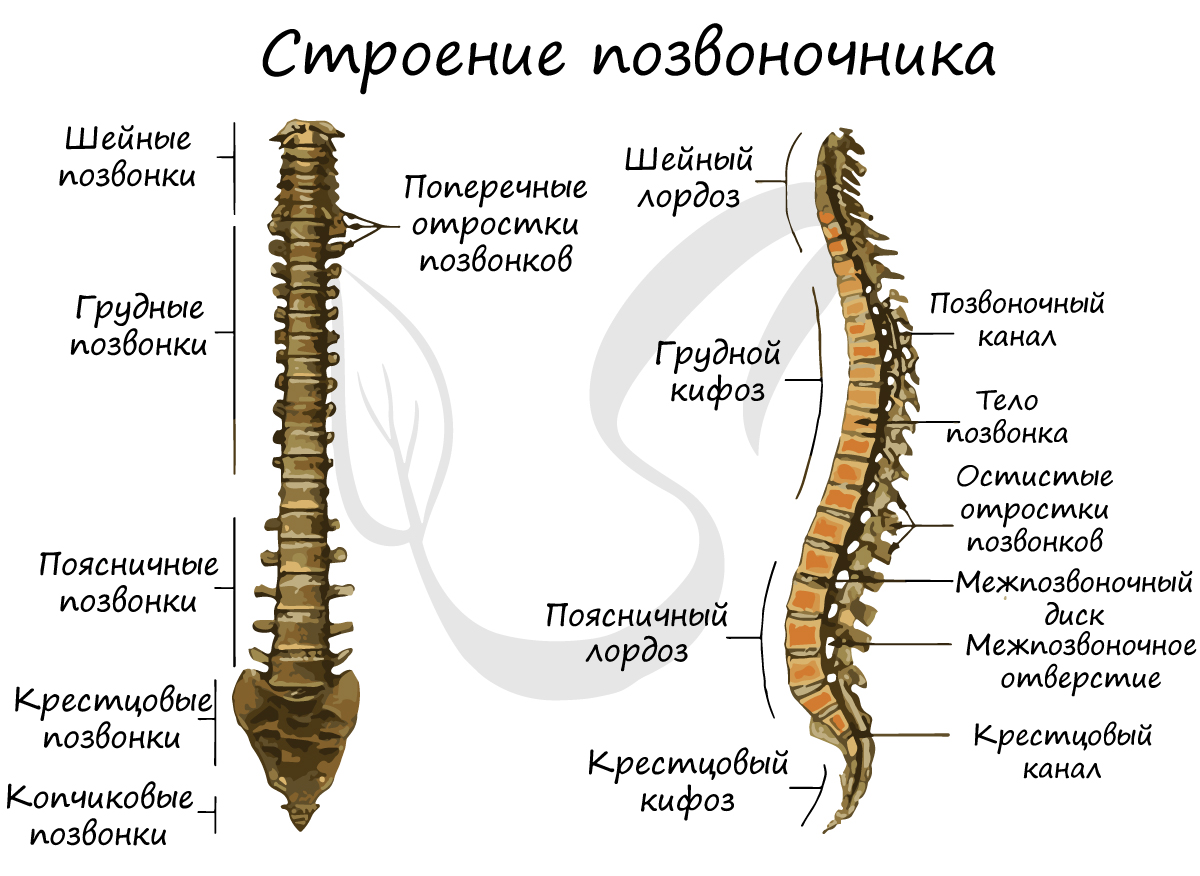
Protects the internal organs from mechanical influences. The skull is the seat of the brain and the sensory organs: it reliably protects them. The vertebrae connect to form the spinal canal, in which the well-protected spinal cord lies.
The skeleton provides support by attaching the soft tissues and internal organs to the various parts of the skeleton.
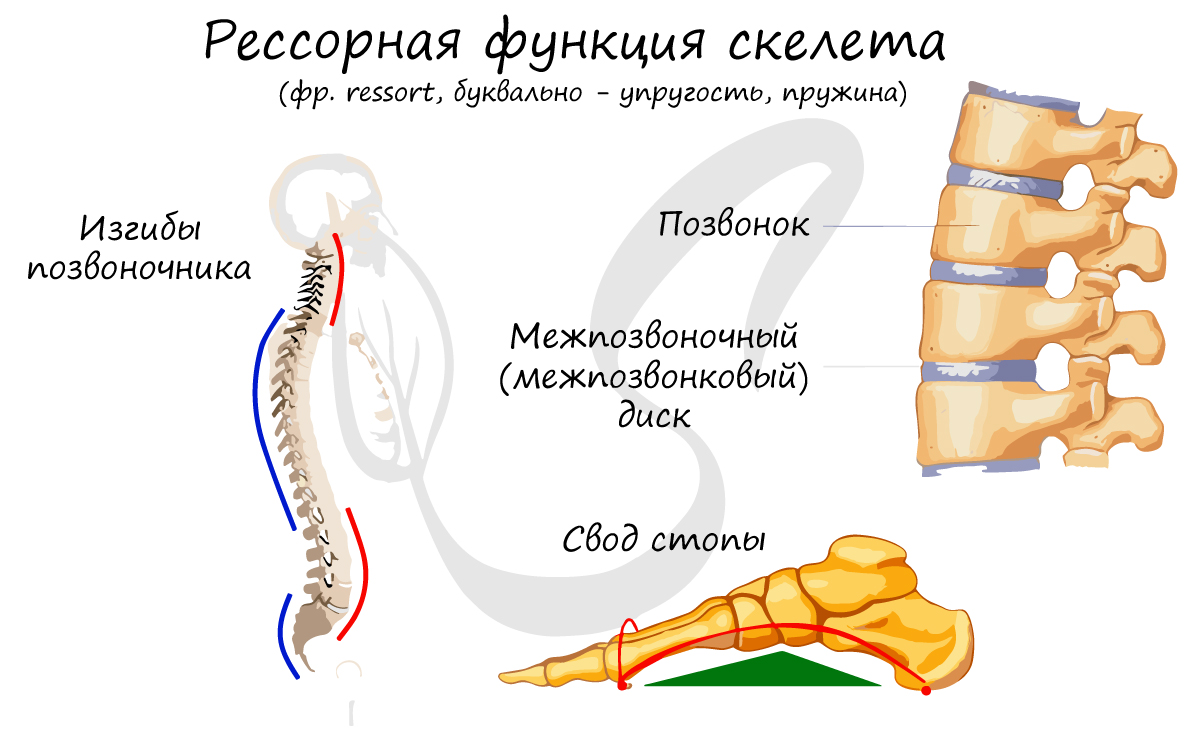
This function of the skeleton is also known as cushioning (amortir – to relax, soften, dampen). The structure of the skeleton (curvatures of the spine, arch of the foot, intervertebral discs) ensures that shocks and blows are cushioned during movement and that the load is evenly distributed.
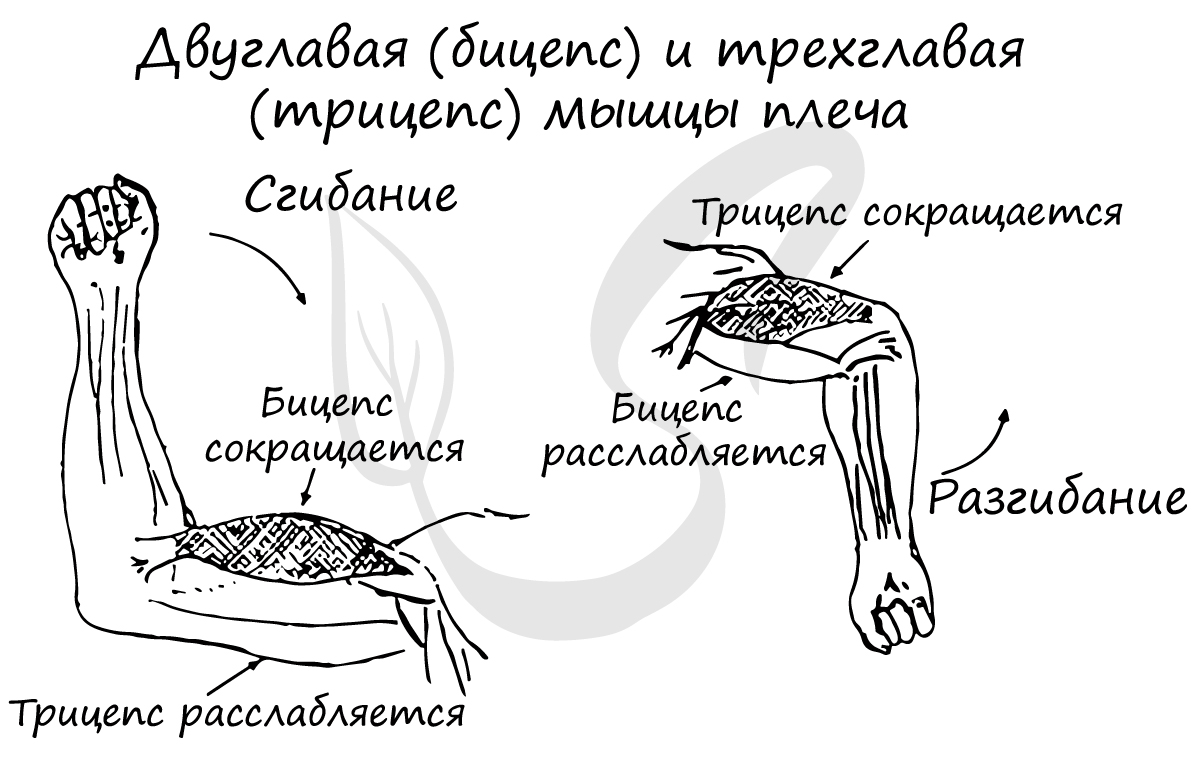
The bones in the joints (moving joints) are the levers that act to make the muscles move.
Bones play an active role in mineral metabolism: Bones store calcium and phosphorus. When mineral metabolism is disturbed, many diseases appear. The most famous of these is rickets, which we will discuss in this article.
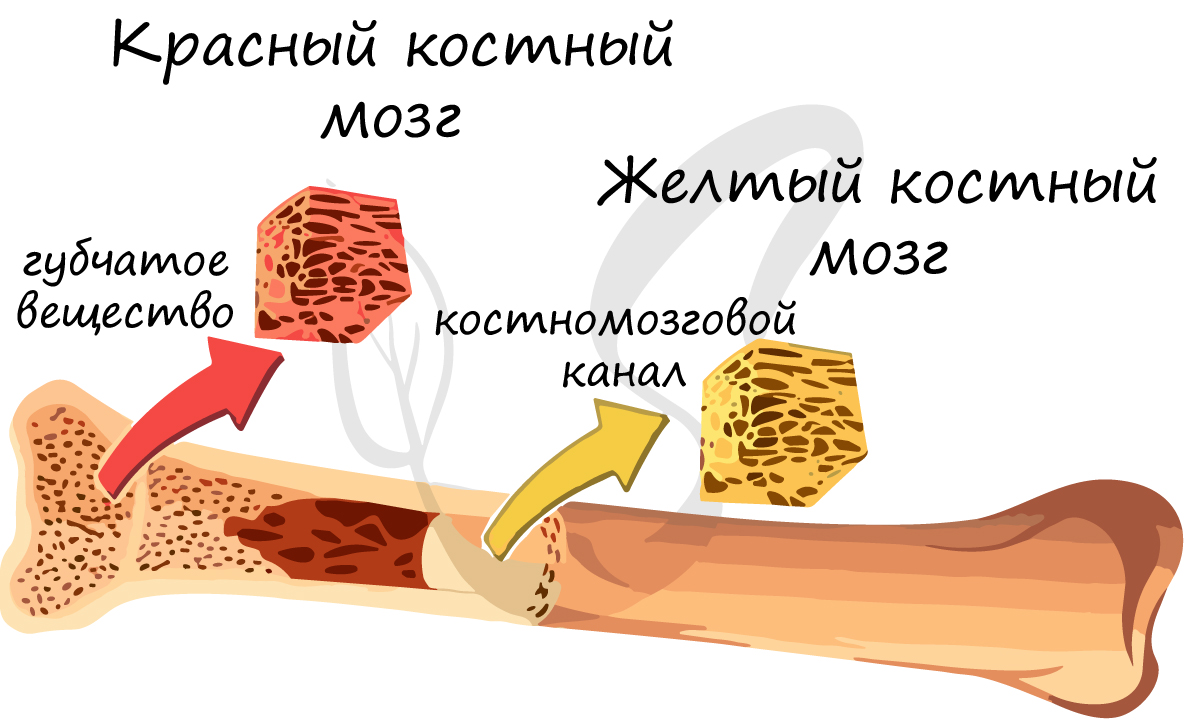
If you're familiar with the structure of bones, you know that the spongy substance is the seat of the red bone marrow, where blood cells form and differentiate: red blood cells, white blood cells, and platelets.
Inside the long bone is the medullary canal, which houses the yellow bone marrow. It has a nutritional function (fat storage) and can turn into red bone marrow (reserve function) in the event of blood loss.
axial skeleton
clinical picture
In contrast to arthrosis, osteoarthritis is not associated with inflammation of the joint. However, the bone structure can injure the surrounding soft tissue. This leads to an acute inflammatory process. If the synovial membrane, ligaments, and tendons are affected, doctors diagnose synovitis. In the acute course of the disease, symptoms of general intoxication appear: fever, neurological and gastrointestinal disorders.

In the early stages of metatarsophalangeal arthritis, symptoms are minor. The sufferer notices pain in the first toe after walking or standing for a long time. The pain subsides when resting or applying a cold compress. The severity of clinical symptoms gradually increases:
- The pain also occurs at rest and makes it difficult to sleep at night;
- The pain is accompanied by a burning sensation;
- Calluses and dry calluses often form;
- The phalanx of the toe is swollen in the morning and stiff in motion ;
- The big toe becomes crooked and there is a valgus deformity of the foot;
- The foot is twisted, causing a change in posture and gait.

The most severe pain occurs with grade 2 arthritis. If a podiatrist is consulted at this stage, this pain can be managed conservatively. Thereafter, the severity of the pain decreases with full or partial joint stiffness. In the fourth radiological stage of metatarsophalangeal arthrosis, the joint becomes immobile. The doctor then only has to diagnose the ankylosis and prepare the patient for the operation.
diagnosis
An experienced diagnostician will suspect an inflammation of the metatarsophalangeal joint when examining the foot. A developing valgus deformity, swelling of the big toe, and flexion of the sole of the foot when walking are signs of this condition. Instrumental studies are performed to confirm the diagnosis. X-rays show osteophyte formation, joint space narrowing, and calcified areas. If necessary, a CT or MRI scan is recommended. These methods are most powerful when it comes to detecting changes in ligaments, muscles, and tendons. Laboratory tests are also carried out:
- General blood and urine tests, the results of which provide information about the general health of the patient;
- Biochemical studies to confirm or rule out rheumatic diseases, endocrine and metabolic disorders, including gout.
Examination of the synovial fluid helps establish the infectious origin of the inflammatory process. The results can be used to determine the type of pathogenic bacteria and their sensitivity to antimicrobial agents.
Skeleton of upper and lower limbs

In this lesson, students will deepen their knowledge of the human skeleton. They deal with the skeletal structure of the upper and lower limbs. The upper limb marginal skeleton and upper limb free skeleton, lower limb marginal skeleton and lower limb free skeleton are explored in detail. The video lesson contains informative material that will help broaden the students' collective perspective and stimulate their interest in the topic.
Overview of the 'Skeleton of the Upper and Lower Limbs' lesson.
The upper extremities (upper limbs) are represented by the hands. The human hands are characterized by a high degree of mobility, with which people carry out various work activities and manipulate objects.
The lower extremities are represented by the legs. They withstand great loads and take over the entire movement function. They are characterized by massive, large and stable joints.
Therewith, Main functions of the limbs are. – are to support the body and to move in space. i the support of work activities.
The upper and lower limbs are attached to the spine via the bones of the limbus: upper part of the shoulder girdle i lower edge of the limbs.
Skeletal structure of the upper limbs. It is formed by the shoulder girdle and the free upper extremity.
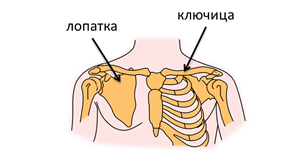
The skeleton of the upper extremity consists two shoulder blades i two collarbones. shoulder blade – is a flat, paired bone with a triangular shape. The shoulder blades lie loosely between the muscles of the back. They form the connection between the humerus and the collarbones. If necessary, they participate in the movement of the arm together with the collarbones.
collarbone – The clavicle is a small, paired bone with a sigmoidal, curved shape. It connects the shoulder blade to the breastbone.
It connects the shoulder to the body. The clavicle lengthens the shoulder joint at some distance from the rib cage and gives freedom of movement to the arm. The long collarbones, the position of the shoulder blades, the flat and wide chest and the large number of muscles make the arm very flexible. It is characterized by a high level of movement precision, which allows e.g. B. allows a circus performer to juggle several objects at the same time and a clockmaker to assemble miniature clocks from parts difficult to see with the eye.
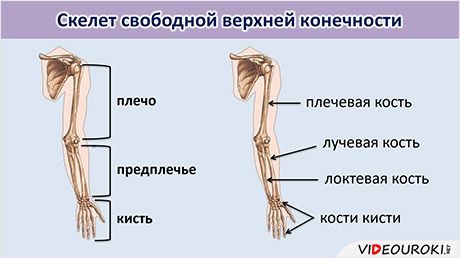
The upper limb consists of three parts: the arm, the forearm i the hand. The skeleton of the free upper limb consists of the humerus, two forearm bones - radius and ulna (on the little finger side) - and the hand bones.
Conservative treatment of metatarsalgia
In many cases, metatarsalgia can be effectively treated with conservative therapy. The type of treatment directly depends on the type of disease diagnosed. Therefore, some patients may be prescribed complex drug therapy, others receive physiotherapy and exercise therapy, and still others only need orthopedic aids.
However, conservative treatment will not be effective unless patients eliminate repetitive forefoot overload. This can be achieved by changing from uncomfortable, tight footwear, especially high heels, to more practical and orthopedically correct footwear. However, many patients, especially women, loathe the idea of having to wear orthopedic footwear. That's because many people find orthopedic shoes gross and unattractive. In fact, there are now many beautiful and shapely models for all occasions that prevent overloading of the forefoot and thus the occurrence of pain and the progression of existing diseases.
Orthopedic shoes have a moderately stiff sole, a rounded, moderately wide nose, often a comfortable, wide heel, and a high, well-fitting footbed.

Also, it is important to normalize weight, which is especially important in overweight patients. Since metatarsalgia prevents patients from significantly increasing their physical activity, a visit to a nutritionist may be recommended. The doctor will draw up an optimal diet plan, explain the basic principles of food selection and combination, calculate portion sizes, etc. At the same time, such a diet will be rational and balanced. It will provide the body with all the necessary substances and contribute to gradual weight loss. However, all diets, especially mono-diets, are dangerous and give only temporary results. Therefore, they should be abandoned once and for all.
Surgical Treatment of Metatarsalgia (Surgery)
In some situations, patients may be offered surgery immediately, e.g. B. in the case of

- a grade 3-4 valgus deformity of the first toe;
- hammer toe deformity;
- Morton's neuroma;
- pronounced flat feet
- severe osteoarthritis of the metatarsophalangeal joint;
- relative extension of 2-3 metatarsal bones;
- Excessive calf muscle tone;
- Failure of conservative therapy after 3-4 months of treatment.
Currently, there are multiple surgical tactics for each type of condition that causes metatarsalgia. In any case, the orthopedist will choose the best surgical technique to achieve the best result.
Modern orthopedic surgery is very safe, especially when performed by a highly qualified, experienced orthopedist. This minimizes the likelihood of classic postoperative complications such as infections, nerve injuries, venous thrombosis and thromboembolism.
Surgery for hallux valgus and hammer toe deformity
Depending on the severity of the deformity, the extent of the degenerative changes in the metatarsophalangeal joint, and the shape and size of the metatarsal bones, the orthopedic surgeon determines the optimal surgical tactics. This can be soft tissue surgery, indicated in the early stages of the lesions, or a more serious procedure that directly affects the bony structures and joint. The latter is performed most often, since metatarsalgia, as a rule, occurs when the pathology reaches stage II or III. If hallux valgus is accompanied by a nodule on the lateral surface of the foot, this is also resected as part of the main reconstructive operation.
Human Foot Tartarus Anatomy Information:
The tarsal bone, metatarsus (English).consists of five metatarsal bones, ossa metatarsalia, which belong to the short tubular bones (monoepiphyses) and resemble the metacarpal bones of the hand. Like these, they have a proximal end, the base, a medial part, the body, and a distal end, the head, the caput. They are counted from the medial side of the foot.

The metatarsals are fused to the distal tarsal bones in such a way that metatarsals I, II, and III are fused to the corresponding sphenoid; the metatarsal bones IV and V are fused with the elbow bone.
The base of the II metatarsal projects noticeably backwards because of the shortness of the intervening ischium that connects it. In addition to the articular surfaces at their proximal ends (articulation points with the tarsal bones), the bases of the metatarsal bones have narrow lateral surfaces - articulation points among themselves. The base of metatarsal V has an articular facet for metatarsal IV on the medial side only. However, on the lateral side it forms tuberositis ossis metatarsalis V.
At the base of the I metatarsal bone is also a tuberous surface, the tuberositas osis metatarsalis I, which extends towards the sole. The heads are flattened laterally and, like the heads of the metacarpal bones, have holes on each side for attaching ligaments. The 1st metatarsal is the shortest and thickest, the 2nd is the longest.
Which doctors should you see for a metatarsal exam:
Are you worried about something? Want to learn more about the metatarsal bones, or need an investigation? You can make an appointment with your doctor – Clinic Eurolaboratory is always there for you! The best doctors will examine you, advise you, give you the help you need and diagnose the problem. You can also make a home visit. clinic Eurolaboratory is open for you 24 hours a day.
How to contact the clinic:
Phone number of our clinic in Kiev: (+38 044) 206-20-00 (multi-channel). The clinic secretariat will find a suitable day and time for you to visit the doctor. Click here for our coordinates and directions. You can find more information about all of the clinic's services on the clinic's website.
If you have been examined before Be sure to bring the results with you to your doctor's office. If you have not yet done any examinations, we will carry out the necessary work in our clinic or with our colleagues in other clinics.
It is important that you take a very close look at your general health. There are many diseases that initially do not make themselves felt in the body, but unfortunately are treated too late. To do this, it is simply necessary to be examined several times a year Several times a year.Your doctor should not only prevent diseases, but also maintain the health of body and mind.
If you have questions to ask your doctor, you can find the answers in our online consultation area. Self Care Tips. If you are interested in reviews of clinics and doctors, you can get information on the forum. You can also register on the physician portal Eurocoolto stay up to date with tarsal news and information, which will be automatically sent to your email address.
bones of the toes
The toe bones, the phalanges digitorum pedis (short tubular bones of a toe), differ from the bones of the hand in their small size. The toes, like the hand, are made up of three phalanxes, except for the first toe, which has only two phalanxes. The end members have a thickening at their end, the tuberositas phalangis distalis, which is their main distinguishing feature.
Sesamoid bones are located in the metatarsophalangeal joints (around the first toe) and in the interphalangeal joint of the first toe.
Note some ossification features of the foot skeleton (Fig. 62): There is an apophysis in the heel bone, tuber calcanei, which develops from several points of ossification, appears at the age of 7-9 years and fuses with the shaft by the age of 12-15 years ; separate bone nuclei are found in the posterior tali process, in the apophysis of the navicularis bone, tuberositas ossis navicularis, in the apophysis of the fifth metatarsal bone, tuberositas ossis metatarsi quinti. During the time that these bone cores exist, they can be mistaken for bone fragments. The crescent-shaped bones of the first toe, which ossify between the ages of 8 and 12 in girls and 11 and 13 in boys, should also be considered in this context. As a result of the reduction, there are often only two phalanges in the V finger – bipalangeal.
It is important to be aware of the possibility of extra, overcomplete or rather incomplete bones in the foot. Truly incomplete bones can be described as those that reflect peculiarities of phyto- and ontogenetic development. There are nine such bones in the foot. They lie between the middle and middle sphenoid bone (os intercuneiorme), between the 1st and 2nd metatarsal bones (os intermetatarseum), over the scaphoid bone (os suprana-viculare), over the talus bone (os supratalus) and at the flexion point of the M. peroneus above the elbow bone (os sesamoideum peroneum).
The remaining 3 bones represent the non-capsular ossification points of the navicular tuberosity (os tibiale externum), the posterior tali process (os trigonum) and the medial ankle (os subtibiale).
Video about the correct anatomy of the foot bones
Publisher: Iskander Milewski. Publication update date: 21.07.2021 r.
The foot consists of three parts: the tarsal, the metatarsal, and the pontics.
The tarsal consists of seven short, spongy bones arranged in two rows. The back row includes the heel and talus bones. The front row consists of the internal group of bones: the navicular bone, the median, medial, and external bones, and the external sphenoid.

The tarsal bone consists of five metatarsal bones. They are short tubular bones with a base, a shaft and a head. The 1st, 2nd and 3rd metatarsals are connected to the sphenoid at the base, the 4th and 5th. The 1st metatarsal is the shortest and thickest, the 2nd is the longest. The mechanical strength of the 1st and 5th metatarsal bones has been found to be three times greater than that of the 2nd.
The toe bones are short tubular bones. The toes provide additional support when walking (see also walking). A good overview of the role of the toes in supporting the foot is to look at the inside of a worn shoe insert, where the areas of the foot that we rely on when walking are clearly contoured.
These differently shaped and sized bones make up the foot and are connected by numerous ligaments and muscles that provide mobility in three planes. The muscles of the foot and lower leg help support the form and function of the foot.
treatment of osteoarthritis
Conservative therapy
To slow down the progression of the disease and make life easier for the patient, podiatrists recommend wearing wide, comfortable shoes with a stiff sole. Individually fitted orthopedic insoles and various types of silicone bursa protectors should be used.
In the early stages of the disease, physiotherapy – UHF, magnetotherapy, electro- and phonophoresis can be used.
Inflammation and pain can also be reduced by nonsteroidal anti-inflammatory drugs. But unfortunately, NSAIDs have a devastating effect on the stomach lining. Not only are they contraindicated in patients with gastritis or peptic ulcer, but they can also promote the development of these diseases.
Intra-articular corticosteroid injections can also be used to reduce pain and reduce inflammation.
The problem is that all these methods can only relieve symptoms and slow the progression of the disease. The only possible solution to osteoarthritis is surgery.
surgical treatment
The choice of the appropriate method depends on the severity of the problem and is determined by the orthopedic surgeon.
In the early stages of arthrosis, joint-preserving operations are performed: cheilotomy (removal of osteochondral outgrowths) and decompression osteotomies of the metatarsal bones and the base phalanx of the first toe (shortening of these bones). As a result, the pain syndrome is eliminated, the joint surfaces are spared and the mobility of the joint is restored.

In the case of severe arthrosis (Hallux rigidus), it is unfortunately pointless to save the joint. In recent years, endoprostheses have been used to treat hallux rigidus. Unfortunately, the results are not always satisfactory. The best treatment for advanced osteoarthritis is removal of the joint.
Bad osteoarthritis: types, risk factors, symptoms and prevention
A distinction is made between transverse and longitudinal foot. In transverse flatfoot, the transverse arch of the foot is flattened and the forefoot rests on the heads of all five metatarsal bones, not just the first and fifth. In longitudinal flatfoot, the longitudinal arch is flattened and the entire sole of the foot is in contact with the ground. The main cause of flat feet is muscle and ligament weakness as a result of trauma or an occupational disease (in people whose jobs require long periods of standing or walking). Flat feet are more common in obese people than in people of average body weight. Many people's feet also become flatter and longer in the evenings (due to muscle fatigue).
Flat feet are characterized by pain in the foot area and rapid fatigue in the legs. The pain can also be felt in the lower and upper thighs and can be accompanied by deformation of the toes. In children, flat feet can develop from frequent physical exertion: carrying heavy objects, the habit of lifting younger siblings, etc.
Prevention of flat feet consists in strengthening the muscles of the feet and lower legs through special exercises (e.g. walking on tiptoe, walking on the outer edge of the foot), avoiding standing on your feet for a long time and using special insoles to increase the arch of the foot.
Occupational stress on the foot leads to significant changes in the foot. An example is the foot of ballet dancers. When standing and walking on tiptoe, the entire weight of the body rests on the first three toes, so the metatarsals and phalanges of these toes are relatively more massive in ballet dancers than in other professions. Although the human foot is highly specialized as an organ of support and locomotion, it is used by some peoples as an auxiliary organ for work. Therefore, they have a high mobility in the ankles and a skilful musculature. If necessary, the mobility of the ankles can be improved by appropriate exercises.
When should I see a doctor immediately?
If the outer part of the foot hurts, but only causes discomfort, then after 2-3 days you should consult a doctor and avoid excessive exertion and other unusual situations that could provoke the pain syndrome. However, in the event of trauma or acute, stabbing pain without an identifiable cause, you should consult a doctor immediately. In the event of a sprain or fracture, medical interventions can help prevent further damage and maintain foot mobility. If the pain is unexplained, a comprehensive examination should be carried out to exclude degenerative processes or hidden fractures.
If you have excruciating or excruciating pain in your foot for more than two days, it is important that you have an examination to rule out a variety of medical conditions, otherwise you risk losing foot mobility and becoming disabled.
The bones of the foot: the tarsal bones
The tarsal is one of the most important bones of the foot. It consists of 2 parts - the rear and the front. The rear part is formed by the heel bone and the ankle bone. The front part consists of 3 sphenoid bones. It also includes the elbow bone and the heel bone.
Regarding the anatomy of the rear part, mention should be made of bones such as the heel bone and the talus. The heel bone consists of the shaft and the head, with the neck (the narrow part) lying between these parts. At the top is the articular surface, which serves as a connection to the adjacent part of the limb - the shaft.
The heel bone is elongated and flattened on the sides. It's the largest bone in the foot. It consists of a shaft and a tubercle that can be easily felt with the hands. There is a protrusion on the inside that serves as a support for the adjacent talus.
In the front area are the sphenoid bones, which are connected to each other. The elbow bone and umbilical bone are also located there. The latter is near the inner edge. Its surface is bumpy on the inside so that the height of the arch of the foot can be determined by touch. It has several articular surfaces that connect it to the neighboring bones.
The elbow bone runs along the outer edge and connects to the parietal bone. It is also in direct contact with bones such as the heel bone and metatarsal bone. There are also three sphenoid bones: the lateral (back), medial, and middle.
diagnosis
As a rule, orthopedic traumatologists deal with establishing the cause of distal leg deformity. If necessary, patients are referred to podiatrists, rheumatologists and other specialists. The examination may include the following diagnostic procedures:
- Anamnesis, external examination
. The specialist determines when and under what circumstances the deformity appeared, notes external changes, assesses the mobility of the joints, determines the pulsation, assesses the sensitivity of the foot. - X-rays.
Depending on the nature of the pathology, X-rays of the toes or the entire foot may be recommended. If necessary, stress tests are carried out. This method can be used to detect traumatic injuries, flat feet, osteoarthritis, chronic arthritis and deep hip joint forms. - plantography.
Allows the diagnosis of longitudinal and transverse flat feet as well as the detection of valgus and varus deformities of the foot. It can be supplemented by podometry and podography to increase the informative value. - laboratory tests
. Intended to determine markers of rheumatic diseases, metabolic disorders and signs of inflammation, study of microflora.
- Metatarsal Bone Injuries.
- Metatarsal amputation.
- tarsal bones of the foot.
- The tarsal bone hurts from above - what to do?.
- Fractures of the tarsal bones.
- tarsal bone in Latin.
- Shapar joint.
- The key to a chopper joint is.