I was referred for arthroplasty surgery with a diagnosis of grade 4 dysplastic hip osteoarthritis. At that point, I had severe pain in the affected joint, difficulty walking, and pain throughout the limb with every movement of the leg.
- I or V METHOD OF FINGER AMPUTATION IN NECROTIC DEVELOPMENT OF DIABETIC STAGE SYNDROME Russian Patent 2007, according to MPK A61B17/56.
- Similar patents RU2302217C2
- The main penis hits the foot
- The most common types of amputation
- Big toe amputations:
- Little toe amputation:
- charpus amputation
- Indications and contraindications
- To understand the foot
- Proprioceptive information about the foot
- The risk factors for developing AS are currently the following:
- SDS classification of wound injuries
- University of Texas classification
- amputation or burial
- religious traditions
- Early postoperative period
- prostheses
- Peculiarities of preparation for endoprosthetics in elderly patients
- Postoperative period: patient rehabilitation
- Before the operation
- After the operation
I or V METHOD OF FINGER AMPUTATION IN NECROTIC DEVELOPMENT OF DIABETIC STAGE SYNDROME Russian Patent 2007, according to MPK A61B17/56.
The invention belongs to medicine, purulent surgery intended for treatment of purulent-negrotic complications of diabetic foot syndrome - gangrene of I or V toe, osteitis of I or V toe, purulent pandactylitis of I or V toe.
The well-known method of foot amputation according to Sharp (1). However, this method consists of transmetatarsal amputation of the foot with a plantar flap and primary suture, which is not applicable in patients with purulent-necrotic complications of diabetic foot syndrome.
The aim of the invention is to improve the treatment of purulent-necrotic complications of diabetic foot syndrome and to reduce complications.
Indication: dry gangrene of the I or V toe, osteomyelitis of the I or V toe, purulent pandactylitis of the I or V toe in the neuropathic and neuron-related form of diabetic foot syndrome.
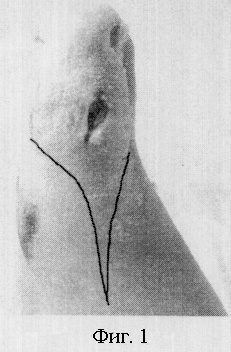
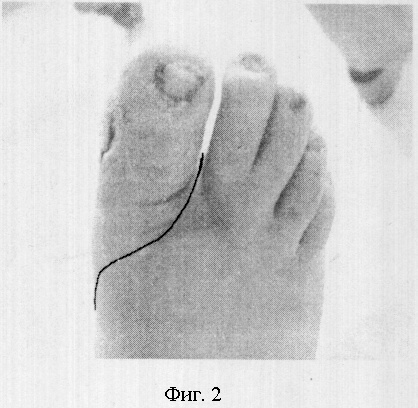
The method is carried out as follows. A plantar flap is cut with an incision at the border of the skin junction from the dorsum to the plantar surface. The boundaries of the incision are shown in Fig. 1 and Fig. 2.
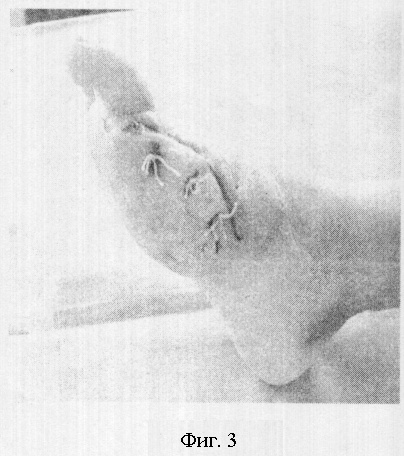
The plantar flap is cut off and the 1st or 5th finger amputated transmontarsally. The joint capsule and the flexor and extensor tendons are carefully removed. In phase 2 of wound formation, place secondary sutures. In this way we close the wound area with a full plantar flap. Fig. 3.
We applied this method to 10 patients with neuropathic diabetic foot and 15 patients with neuroischemic foot. Follow-up examinations after 1, 3, 6 and 12 months revealed no complications. The application of the proposed method of wound surface closure has several advantages: no trophic ulcers, fissures or bicatrial deformities are formed.
The technical simplicity and the accessibility of the method allow the use of the described method in surgical hospitals.
Similar patents RU2302217C2
- Viktor Ivanovich Nefedov
- Shtilman Mikhail Yuryevich
- Khumburidze Igor Pavlovich
- Osipov EV
- Vyacheslav Timofeevich Krivikhin
- Denis Krivikhin
- Andrei Sergeyevich Meisterov
- Lobakov Aleksandr Ivanovich
- Maria Yevgenevna Eliseeva
- Ambrosimova Olga Sergeyevna
- Bocklin Alexey Alexandrovich
- Alexei Wachev
- Boklin Olga Alekseevna
- Aleksandr Vladimirovich Vavilov
- Maxim Gennadevich Gulyayev
- Alexei Olegovich Demyanov
- Viktoria Vadimovna Dobrova
- Yevgeny Borisovich Yelen
- Alexei Saytsev
- Dmitry Sergeyevich Kazakov
- Maxim Vitalyevich Kotikov
- Fedorin Alexander Ivanovich
- Elena Vladimirovna Frolova
- Oksana Georgievna Khoroshun
- Dmitry Arkadievich Shumkov
- Bensman WM
- Trilandafilov KW
- Trilandafilov KG
- Bocklin Alexey Alexandrovich
- Alexei Nikolayevich Wachev
- Valery Afanasyevich Mitisch
- Yulia Sergeyevna Pashalova
- Lyudmila Doronina
- Victoria Viktoria Garyaeva
- Magomedgadzhiyev M.Kh.
- Magomedgadzhiyev M.-AI
- S. Safarov
- Magomedgadzhiyev MA
- Magomedgadzhiyev M. -GI
- Abdulmadjidow HM
- Magomedov NI
- Aliyev MA
- Bensman VM
- Triandafilow KG
- Ovanes Asvaturovich Yavruyan
- Aleksandr Georgievich Chityan
- Igor Pavlovich Khumburidze
- Mikhail Yuryevich Stilman
- Sergei Alexandrovich Kovalyov
- Tirakant Irina Vladimirovna
- Erik Rafailovich Zadykhanov
The main penis hits the foot
Incidentally, the severity of diabetic complications in the foot is not necessarily related to the severity of the disease. Most complications occur in patients with moderate forms of the disease, often type 2 diabetes, putting a large number of patients at risk.
Diabetes-related lower-limb disorders that increase the risk of amputation include peripheral neuropathy, peripheral vascular disease, and infections.
A major amputation means a reduced life expectancy for a patient with diabetes, and in some cases only half of the patients will later be able to walk again (with or without a prosthesis). In contrast, with distal amputation (transmetatarsal or medial amputation), walking ability can be preserved in up to 92% of the healed cases. For this reason, many efforts are currently focused on finding treatment strategies to convert the previously common axillary amputation into a partial amputation of the distal foot at the level of the tarsus. A location that ensures more favorable biomechanics for the patient.
The vasculopathy in the form of a macro- or microangiopathy is decisive for the prognosis of the extremity. In contrast, peripheral neuropathy in the form of neuroarthropathy is a trigger for deformities and thus for ulcerations and infections in the diabetic foot.
The most common types of amputation
Despite the many possibilities, it should be noted that almost every amputation changes the gait pattern drastically. For example, a simple metatarsal bone loss (MTF) is known to have major negative effects.
Big toe amputations:
This can be done by disarticulating the MTF, but where possible and although technically more difficult, we believe it is preferable to preserve the base of the proximal phalanx. The potential advantage of their preservation is the partial preservation of the biomechanical and functional mechanisms of the first ray through the attachment of the plantar fascia and the short flexor of the big toe.
Even if it is a well-tolerated amputation, it must be said that the change in the propulsion phase of the gait is significant, and there are studies showing how the amputation of the big toe leads to secondary deformations of the adjacent toes and thus new deformations contributes.
Little toe amputation:
As with the big toe, it is preferable to leave the remaining portion of the toe disarticulated when possible. In this case, the advantage is that the remaining toe acts as a spacer, preventing deviation of the adjacent toes.
charpus amputation
charpus amputation (metatarsal amputation or amputation through the metatarsal bones) is the severing of the distal portion of the foot and the formation of a stump. It is carried out with severe trauma and purulent processes associated with the loss of viability of this part of the limb. Performed under general anesthesia or using a nerve conductor, it involves making incisions on the sole and back with the formation of two flaps of skin, severing the bone, ligating the spinal artery, and suturing the wound on the back of the foot. The foot is then fitted with a special shoe to ensure walking function.

Sharp foot amputation (metatarsal amputation or amputation through the metatarsal bones) means that the distal part of the foot is severed to create a stump. It is performed in severe trauma and purulent processes with loss of vitality of the affected limb. It is performed under general or regional anesthesia and involves incisions on the sole and dorsal surface with the creation of two skin flaps, division of the bone, ligation of the dorsal artery and closure of the wound on the back of the foot. The subsequent walking is supported by footwear.
Indications and contraindications
Acute amputation is performed in the event of contusions, extensive traumatic bone and soft tissue injuries, deep pressure sores, circulatory disorders of various genesis, acute infectious processes in the distal sections of the foot. Since operations in traumatology are usually carried out as emergency procedures, only pronounced coagulation disorders and severe general diseases due to other injuries or decompensated chronic diseases are considered contraindications.
The operation is performed under or under general anesthesia. The doctor makes incisions on the dorsal and plantar surfaces of the foot. On the dorsal part of the foot, the incision is made near the diaphysis of the metatarsal bones with a slight forward tilt. A longer flap of skin is applied to the plantar side. The long flap on the plantar side is placed in such a way that the scar is on the dorsal surface and the support function of the foot is not compromised. The flap of skin is cut off. The tarsal bones are divided at the base of the flap. The dorsal artery of the foot is ligated. Stitch the skin shut and cover the wound with an aseptic bandage. The limb is immobilized with a plastic or plaster cast.
To understand the foot
First we must understand its primary function, which is: it is an important support to be able to walk on two legs (two feet).
The feet perform several basic functions:
They absorb the entire weight of the body and ensure its balance.
They absorb constant shocks and soften the energy generated by the forces involved in walking.
They adapt to different types of surfaces, even the most uneven.
Acting like a rigid lever to generate the propulsive force needed for walking.
Transmission of the rotational forces generated by the hip.
Of course, this is related to walking.
Proprioceptive information about the foot
Your muscles, tendons and joints have special sensors that react to movement or pressure. These allow your brain to know how your feet are positioned in relation to the surface.
All of the structures that make up the foot, the muscles and tendons, work with the bones, ligaments and joints and are synchronized with the brain to enable the foot to perform these functions. If one of these components is not working properly, all the others will be affected as well.
The risk factors for developing AS are currently the following:
- peripheral sensorimotor and autonomic neuropathy;
- chronic arterial insufficiency of the lower limbs;
- foot deformities;
- previous ulceration and/or amputation;
- Trauma;
- inappropriate footwear;
- social and psychological factors;

SDS classification of wound injuries
*(Wagner FW, St Louis: Mosby Year Book, 1979:143-165)
| Degree | characteristics |
| 0 | Dry skin, beak-like deformation of the fingers, osteoporosis |
| 1 | Superficially ulcerated cavity with no evidence of infection |
| 2 | Deep infected ulcer without bone involvement |
| 3 | Deeply infected ulcer with bone involvement, abscess, mucus |
| 4 | Limited gangrene (toe, part of foot) |
| 5 | Gangrene of the entire foot |
University of Texas classification
*(LA Lavaery, Armstrong DG, Harkless LB Foot Ankle Surg, 1996, 35:528-531)
A classification of the diabetic foot that assesses the risk of ulceration and amputation risk, taking into account the degree (horizontal) and extent (vertical) of the ulceration.
Grade 0 means no ulceration, I - superficial soft tissue lesion, II - ulceration extending to the tendon or joint capsule, III - ulceration extending to the bone or joint.
Grade A - lesion without infection and ischemia, B - lesion with infection, C - lesion with ischemia, D - lesion with infection and ischemia.
| category 0 (no pathology) | The patient has diabetes mellitus. The protection sensitivity is intact. PLE > 45mmHg. No history of ulcers. Foot deformities may be present. |
| category 1 (neuropathy without deformities) | Protective sensitivity is absent. PLE > 0.8, thumb systolic pressure > 45 mmHg. No history of ulceration. No history of Charcot foot deformity. |
| category 2 (neuropathy with deformities) | No defensive sensitivity. PLE > 0.8, systolic thumb pressure > 45 mmHg. No history of ulceration. No history of Charcot foot. Deformities of the foot (pressure points) present. |
| category 3 (Severe medical history) | No defensive symptoms. PLE > 0.8, systolic thumb pressure > 45 mmHg. History of ulceration. History of Charcot foot. There are foot deformities (pressure points). |
| Category 4A (Neuropathic Ulcer) . | Lack of defensive sensitivity. PLE > 0.8, systolic thumb pressure > 45 mmHg. ulceration present. Lack of a Charcot foot. Deformities are present. |
| Category 4B (Charcot foot, acute stage) | Lack of Defense Sensitivity. PLE > 0.8, thumb systolic pressure > 45 mmHg. Uninfected neuropathic ulcerations may be present. Charcot foot is present. |
| category 5 (Infected Ulcer) | Protective sensitivity may be present. infected ulcer. Charcot foot may be present. |
| category 6 (coronary limb) | The protective sensitivity may not be preserved. PLE < 0.8, systolic pressure in the thumb < 45 mmHg or foot oxygen saturation < 40mmHg. Ulcerations may be present. |
amputation or burial
Although amputation is a surgical procedure known to all, most people do not give much thought to what happens to organs when they are removed from the human body. There are basically two ways to dispose of them: either they are disposed of as medical waste (by incineration) or they are buried. In countries where the latter is legal, it's not uncommon for patients to ask doctors to donate amputated limbs and internal organs for burial - particularly in the United States and some European countries. There are no reliable statistics on the number and frequency of such cases, but at least we know the causes of such patient requests: religious traditions, folk traditions and the need to process the loss in a ritualized form. For the latter reason, surgeons in some countries are advised to anticipate such patient requests and address the issue early.
In countries where it is possible to bury limbs and internal organs, healthcare professionals typically have three options for burial of dead tissue:
- A private agreement with tacit consent to the burial of dead tissue provided for in legal and other documents.
- By providing explicit instructions for the removal of specific tissues (and obtaining the patient's informed consent).
- By specific regulations for further disposal of dead tissue.
In the latter case, it is usually envisaged that the healthcare institutions themselves will contact the undertaker to whom the limb will be buried and follow their path to ensure that the amputated organ is buried according to sanitary standards. In another case, an agreement can be made with the patient whereby the patient accepts responsibility for contacting the undertaker and arranging for the burial of the removed tissue within a specified period of time. In some health care facilities, the question of the subsequent removal of the amputated tissue is part of the consent form for the operation. If the healthcare facility provides for the amputated tissue to be handed over directly to the patient or his representative, the patient must sign additional documents confirming his awareness of all the risks involved and his responsibility for burying potentially hazardous medical waste.
religious traditions
Limb burial is primarily associated with the religious traditions of Judaism in many countries, although Christians and Muslims often practice limb burial in similar ways. In the Jewish ritual tradition, the custom of burying amputated limbs is quite old - at least fifteen hundred years old. As the Babylonian Talmud indicates, there were places in cemeteries where severed limbs were buried. However, we cannot be certain that the original motivation for burying limbs was based on theological reasons: most likely, limbs were buried because something had to be done with them, and the ancient followers of Judaism could not find a better way to dispose of body parts in such a way that humans or animals could not desecrate the remains - in that sense, burying them deep underground seems a perfectly rational solution. This hypothesis is also supported by the fact that no specific rituals for limb burial are described in the sacred texts of Judaism, nor do we have any historical evidence that such rituals existed in ancient times.
Currently, this question is handled differently not only by country, but also by rabbinate: some rabbis, citing various theological arguments and historical precedents, decree that their flock should make an obligatory effort to donate amputated organs for later burial, others Rabbis consider this to be better than mandatory, and still others generally tend to leave the matter open and left to the discretion of individual families. There are also differing opinions among Jews as to whether a person should be buried in the same grave as their amputated limb or whether it should be a different burial site.
In Islam there is a similar diversity of opinion regarding the burial of limbs. Different imams in different countries will interpret this situation differently, and likewise some may argue that limb burial is mandatory while others find it more desirable. This has long been a problem for Christians – for Catholics in particular, cremation was forbidden until the late 20th century, so medical disposal of internal organs and limbs by cremation also became problematic. Banned in the 19th century, medical disposal of internal organs and limbs by incineration also became problematic. Many Christians today insist that lost organs be donated to the earth and then reburied in the grave where they themselves eventually lie - some believe this is necessary in order to be resurrected in their bodies when the last days come.
Early postoperative period
In order to avoid serious complications, it is important to strictly follow the doctor's instructions and take painkillers at the right time and in the right amount to relieve the pain. Swelling should not be interpreted as pathological, it is a typical body reaction to the operation. Compression therapy, massage with lymphatic drainage and correct positioning of the residual limb should be used, e.g. B. It is not recommended to keep the residual limb in flexion for a long time.
To prepare for fitting a prosthesis, you should see a physical therapist. The physiotherapist will find a series of muscle strengthening exercises to relieve the severed limb and normalize circulation. If the leg has been amputated, physical exercise is required to prepare for axial loading. Therapeutic exercise is an effective way to avoid pressure points and contractures, which can be an impediment to fitting a prosthesis. The more time spent in immobility, the faster contractures develop and grow in the joint. When exercising, it is important to avoid movements that cause pain.
- keep the balance
- move with additional support (e.g. with crutches),
- caring for the remaining limb (good hygiene, use of medicated and moisturizing skin preparations),
- Monitor scar healing (this process can take up to 18 months).
prostheses
Physicians recommend fitting prostheses as early as possible, as this allows for appropriate compensatory adjustment of motor behavior, thus facilitating motor function recovery. The initial provision of a prosthesis can be made 14-21 days after the amputation, when the wound has started to heal and there is no inflammation of the stump tissue. A second adjustment of the prosthesis (or orthosis) is performed when the prosthesis wears out.
After fitting the prosthesis, a second rehabilitation measure is recommended. As a rule, the team of specialists at the rehabilitation center consists of an attending doctor, an occupational therapist, a physiotherapist, nurses and a psychologist.
If the leg has been amputated, the person concerned must learn to stand securely on the prosthesis, climb stairs and carry out everyday activities. If the arm has been amputated, the person must learn to flex and straighten the joint and hold objects. It takes two to four weeks to prepare a person with a prosthesis to walk.
Amputee survivors must readjust their clothing and footwear. Even shoes with a flat sole do not always fit the prosthesis:
Shoes with a slight instep in the heel area are recommended. When an arm is amputated, an occupational therapist's help is needed to show how to perform everyday activities with one hand or with a prosthetic device.
Peculiarities of preparation for endoprosthetics in elderly patients

Joint replacement is the partial or complete replacement of a joint with an endoprosthesis or an artificial implant. Arthroplasty is a highly effective and often the only way to restore joint function.
The most common type of endoprosthetics is hip replacement. The indication for a hip joint prosthesis is a severe functional impairment of the joint. Osteoarthritis, which develops on average in people over the age of 50, and progressive osteoarthritis are the most common reasons for the need for a hip replacement. These diagnoses are also much more common in older patients than in younger ones.
The preparation phase is an important and integral part of the entire hip replacement process. The state of health before the operation determines the success of the operation and the recovery time. Elderly people require special attention during the preoperative examination.
In middle-aged and older patients, factors complicating the surgical and rehabilitation process are more likely than in younger patients, e.g. B.
- High levels of sugar in the blood, which causes damage to the walls of the blood vessels and affects the blood supply to the organs and limbs;
- Iron deficiency anemia (especially in women). This factor can be both a manifestation of a latent disease and delay recovery;
- a tendency to form blood clots;
- varicose veins of the pelvis and limbs;
- overweight. A body weight that exceeds the optimal BMI (Body Mass Index) can pose a serious obstacle to the body's adaptation to the implanted joint;
- osteoporosis, bone thinning, brittleness;
- cardiac arrhythmia, coronary artery disease;
- Chronic inflammatory processes.
Postoperative period: patient rehabilitation

A rehabilitation program after an endoprosthesis is essential for patients of all ages, although there are no major age-related differences. You need to get used to the implant, consider its (and your) abilities and, of course, begin to restore blood circulation and muscle function in the operated limb almost immediately after the operation.

Maxim Mikhailovich Rankov
Rehabilitation after surgery is crucial for elderly and elderly patients. It is often the age factor that determines the need for an active rehabilitation program. Young patients sometimes become active themselves and recover without the help of professionals: they literally get up and walk'. They are in a hurry to return to their former active lives, engage in their old activities and go to work.
In older patients, chronic medical conditions and the habit of sitting before surgery can hinder active movement. Therefore, these postoperative patients should be cared for by physiotherapists. Physiotherapeutic treatments for patients are indicated, and it makes sense to use the facilities of sanatoriums and recreation centers. Again, rehabilitation leave is essential for these patients.
In general, the rehabilitation program does not differ by age: the exercises, procedures and principles are the same for each body. However, older people rarely recover on their own in the postoperative period; they need treatment. Postoperative pain and a lack of motivation to move 'here and now' prolong and complicate the recovery time. If the operated person is unable to take care of the rehabilitation himself, the functional result remains the same: the patient was unable to walk and still cannot.
Before the operation
- The patient is hospitalized the night before the operation and is not allowed to eat or drink for 12 hours before the operation.
- The necessary medication can be swallowed with a few sips of water as directed by the doctor.
- The surgeon may give the patient general anesthesia to ensure the patient falls asleep and does not get sick. Alternatively, the patient may receive spinal anesthesia to numb the surgical area.
- First, the surgeon makes several incisions (cuts) on the front of the patient's foot.
- The surgeon cuts through and removes any damaged or infected bone.
- The surgeon then cuts through nerves, blood vessels and tendons.
- If the infection is severe, the surgeon places a sterile bandage on the surgical wound and leaves it open to heal. Or the surgeon closes the wound with stitches or staples.
- The surgeon may use a skin graft from a donor or from another part of the patient's body to close the wound.
- The surgeon may trim the wound and insert drains to remove excess blood and fluid discharge.
- The surgeon will flush the wound with a sterile solution and then apply a bandage.
After the operation
- The patient is transferred to the general ward and monitored for several hours.
- Antibiotics and analgesics are administered. Intravenous fluids are continued.
- The bandage is usually removed on the third day, the wound is checked for healing, cleaned and redressed.
- The patient is discharged from the hospital after 5-14 days.
If the patient has diabetes, he must consult his doctor about diabetic foot treatment.
The patient must wear a splint, shoes, or special footwear such as custom-made shoes (eg, steel implants in the soles of the shoes) to support the rest of the foot.
The patient must lie down and elevate the foot above the heart to reduce swelling. Once the pain and swelling have subsided, the patient will see a physical therapist who will show them some exercises to restore mobility and strength to the operated foot.
Ideally, the wound should heal completely in about four to eight weeks. Once the wound has healed, the patient can opt for a prosthesis.
The transition from your own foot to an artificial foot can be psychologically draining, and adjusting to this new life change can be a long process. Therefore, professional counseling of the patient is important in this phase.
Read more:- Why amputate legs for diabetes?.
- X-ray of Charcot's foot.
- Indications for amputation.
- What is Charcot?.
- The reamputation is.
- Diabetic foot ulcers.
- Charcot-Marie foot.
- Limb amputation.