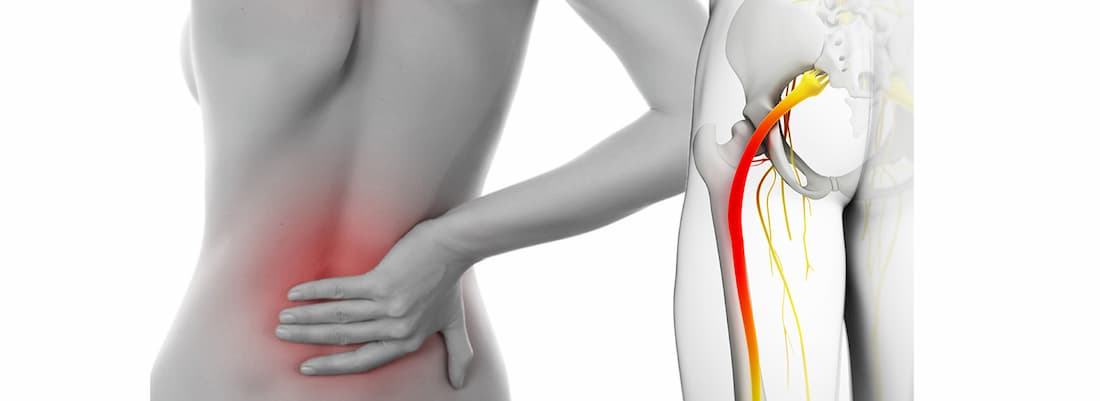
The sciatic nerve is the largest nerve in the body. It is formed by branches of the spinal roots, which emerge from the spine at the level of the 4-5 lumbar vertebrae and 1-3 sacral vertebrae. The nerve exits through the tuberculous opening in the gluteal muscles and runs along the posterior surface of the buttocks and thigh to the knee.
- Neuropathy of the pudendal nerve
- The pudendal nerve - symptoms of neuropathy of the genital nerve
- causes
- Secondary Causes
- symptoms
- symptoms
- diagnosis
- Rehabilitation after neurolysis
- Where is it carried out?
- Compression of the ulnar nerve or carpal tunnel syndrome
- diagnosis
- CONSERVATIVE TREATMENT
- SURGICAL TREATMENT
- causes of pain
- Associated Symptoms
- prevention
- Treatment of occipital neuralgia with herbal medicines
- prognosis for recovery
Neuropathy of the pudendal nerve
Occurs with varying frequency. It occurs up to five times more often in women than in men, for which there is a logical explanation. Pudendal neuropathy can be caused by:
- Chronic trauma of the gluteal region - typical of professional cyclists and jockeys, as well as those whose professional activity is predominantly sedentary - school principals, grandmasters, etc.
- Consequences of severe pelvic injuries with fractures of the pelvis, sacrum, coccyx.
- Operations and diseases of the pelvic organs (here we are of course mainly concerned with the female lobe): inflammatory diseases of the ovaries and adnexa, endometriosis, prolonged and difficult and/or multiple births.
- Gastrointestinal disorders with constipation.
The true frequency of urogenital neuropathy is not known worldwide. It is said to be of the order of 1:100,000, but the French, acknowledged leaders in the treatment of such a delicate problem, claim that it is 1:6,000. Few people openly admit their problem, confide in their doctor, and that's understandable. The 'painful' nerve is called the umbilical nerve, from the word 'pucker', and the name speaks for itself. The pudendal nerve, the genital nerve, the pudendal nerve are synonyms and mean the same thing.
The pudendal nerve - symptoms of neuropathy of the genital nerve
In France, which plays a pioneering role in the treatment of pudendal neuropathy, the classic diagnostic criteria for pudendal neuropathy are given. NANTES
- Pain in the perineum, anus, vagina, penis, or clitoris that is shooting and twisting, sometimes referred to as a 'hot poker', a 'golf ball' at the site, which is understandably excruciatingly painful and distressing to the patient leaves. In France, 3 patients recently committed suicide because of this pain.
- The pain increases when sitting and is caused by tension and compression of the nerve between the massive ligaments.
- There is no objective sensory impairment in the perineal area, although patients describe a subjective feeling of dullness.
- The pain does not bother at night, and patients often wait until night. In the supine position, the pelvic-musculoskeletal system is relaxed, nerve tension is reduced, and the intensity of pain is reduced.
- The effect of local anesthetic block on the genital nerve is that under X-ray control, the anesthetic is injected into the projection of the genital nerve in the allocockygeal canal and the pain subsides.
In addition, there are additional diagnostic criteria related to intestinal and urinary disorders, erectile dysfunction, pain on palpation of the alveolar canal, pelvic tone syndrome, pain on palpation of the perineum and positive skin roll test.
Instrumental methods are of secondary diagnostic importance, and the diagnosis of this disease is carried out at the bedside, that is, by simply asking and examining.
Ultrasound diagnosis is definitely helpful in making a correct diagnosis, but this depends on the experience and empathy of the ultrasound technician. The St. Mark's electrode ENMG is also frequently used for diagnosis.
causes
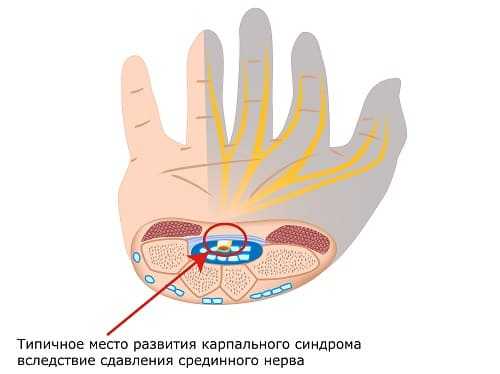
It's not just injuries or illnesses that can cause discomfort and dangerous consequences. The pathology is caused by an unfavorable working posture of the hand, which leads to the development of tunnel syndrome.
Damage to the hand, lack of mobility or sensory disturbances in the hand raise the suspicion of neuropathy of the median nerve of the upper extremities. The abnormal condition can have various causes.
- Bundle compression in the narrow canal between the muscles of the forearm and hand. This affects not only the wrist, but also the skin of the hand and fingers I-IV.
- Toxic affliction. Caused by regular alcohol consumption, drugs or chemical poisoning.

- Rarely from long-term use of neurotoxic drugs. Nervous tissue gradually deteriorates and ceases to perform its functions.
- A hand injury with isolated bundle damage leads to the development of post-traumatic mononeuropathy (neuropathy) of the median nerve. Soft tissue, muscles and ligaments can be damaged extensively and extensively. In many of these patients, the problem can be corrected, including through surgery. However, sometimes it is not possible to restore the nerve fibers to their original state.
- Diabetes. If the blood sugar level is too high, the nerve fibers lose their ability to function. A process of irreversible degeneration occurs.
It is possible that the tunnel neuropathy of the median nerve in the hand is accompanied by inflammation, the treatment of which can only be prescribed by a doctor. Multi-joint inflammation occurs, for example, when the small joints between the forearm and hand are inflamed.
Secondary Causes
In addition to the main causes mentioned above, certain diseases and pathological processes can also provoke the problem:
symptoms
The most common condition is thought to be compression neuropathy (neuropathy) of the median nerve in the upper limbs, caused by stretching and swelling of the muscles that the nerve bundle runs between. It's important to realize that the median nerve is long and radiates from the shoulder. And damage can occur at a high level.
The severity and dynamics of clinical symptoms depend on the damaging factors. Trauma and compression, such as in carpal tunnel syndrome, cause acute damage to the innervation of the hand. Diabetes, on the other hand, is characterized by a gradual deterioration in nerve function.
Mononeuropathy of the median nerve is characterized by:
- decreased sensitivity of the skin in the middle of the hand, from the thumb to the ring finger;
- a drawing pain in the wrist;
- a burning sensation in the same area;
- The fingers can no longer be bent;
- grip strength decreases;
- Muscle atrophy occurs over time.
Only the branches that provide sensitivity on the back of the hand pass through the carpal tunnel. Therefore, skin sensitivity on the surface of the hand is rarely affected.
Sensory neuropathy of the terminal branch of the left or right median nerve is characteristic of the early stages of the pathology, when only the sensory branches are damaged. Unpleasant sensations in the hand can even cause a person to wake up at night. The hand feels numb, burns and tingles. Symptoms subside when the hand is shaken but return and worsen when the hand is flexed or flexed.
The appearance of motor disorders, preceded by sensory disorders, indicates the progression of the pathology. In traumas in which the thick bundle is damaged (fractures of the shoulder and forearm), sensory and motor disorders occur simultaneously.
symptoms
The main symptom of a compressed sciatic nerve is pain. It starts in the buttocks and moves down the back of the thighs to the knees and ankles. Depending on the location and severity of the entrapment, the sensation may be sudden and abrupt or it may be stabbing and persistent.
If the impingement is in the spine or hip joint, the pain is excruciating and worsens when walking, squatting or bringing your legs together.
The affected person notices impingement in the foramen magnum of the sternum
- A dull pain in thigh ;
- a feeling of cool or burning skin in the affected area;
- Decreased feeling in the hamstrings and around the Achilles tendon;
- Sweating in the feet, feeling of heat in the toes.
If a major artery in this area is crushed along with a nerve, the patient will develop claudication syndrome. Prolonged walking causes pain in the leg with numbness in the fingers and paleness of the skin in that area. This spontaneously disappears with rest. There are often slight functional disorders of the pelvic organs, e.g. B. to take a break before urinating.
Symptoms worsen with walking and sitting.
diagnosis
Diagnosing a compressed sciatic nerve requires a comprehensive examination of the patient. The doctor not only has to determine whether the nerve fibers have been compressed, but also at what level this has happened. This is done by:
- Conversation with the patient in which he describes his complaints; special attention is paid to the nature of the pain, its intensity and additional sensations associated with the attack;
- Collection of medical history: time of onset, chronic illnesses, previous injuries, etc.;
- Examination: assessing the quality of the reflexes, the condition of the spine, identifying the areas of greatest pain, etc.;
- X-ray, CT, or MRI of the lumbosacral spine to look for signs of osteochondrosis, disc bulging or herniation, and spinal stenosis;
- Ultrasonography of the affected area to detect muscle spasms;
- Lower limb vascular duplex scan (USDG): to assess the condition of the arteries and veins and rule out a vascular cause of the abnormality;
- General blood and urine tests and, if necessary, biochemical blood tests.
If the sciatic nerve is affected by a pelvic disease, an additional consultation with a urologist or gynecologist is required, and appropriate examinations (ultrasound, tests, swabs, etc.) are carried out.
The diagnosis is finally confirmed when examination reveals specific symptoms characteristic of sciatic nerve damage:
- Bonnet's sign: With the patient lying supine, the physician elevates the straight leg, which causes more pain, and then bends it at the knee, which causes less pain;
- Crossed Syndrome: Raising one leg also causes pain on the other side;
- Decreased expression of the plantar, knee and Achilles reflexes.
Rehabilitation after neurolysis
Recovery from neurolysis begins with restoring sensation and eliminating pain sensations. It does this by relieving pressure on the nerve. All other functions recover slightly more slowly. The earlier the operation is performed, the easier the rehabilitation. After the operation, the function gradually returns:
- Nerve function improves or is fully restored.
- The pain is gone.
- restoration of sensation.
- normalization of sweating.
Where is it carried out?
Neurolysis requires extreme care, thorough knowledge, high qualification and experience of the surgeon. Neurolysis can be performed at NCC Clinic No. 2 (Central Clinical Hospital of the Russian Academy of Sciences) in Moscow. Experienced specialists perform the operation with a guarantee of quality. To make an appointment with a surgeon, receive an initial consultation and find out more about prices and terms of service, please call the telephone number provided on the website.
Our experts will contact you shortly.
Subscribe to the NCC2 Telegram channel to keep up to date with our news.
Compression of the ulnar nerve or carpal tunnel syndrome

It occurs in people who frequently bend their arm at the elbow—cyclists, computer programmers, and others. The ulnar nerve is often affected in very slim women. In this case, the pain and numbness begin in the little finger and spread to the whole hand. The muscles on the back of your hand between your thumb and forefinger become thin and work harder. In wet, cold weather, the pain is almost unbearable.
diagnosis
Pain, numbness, 'goosebumps' and restricted movement in the arm cannot only be caused by a compression of the nerves in these bone canals. There are also brachial plexus disorders, herniated discs, muscle thickening, and other disorders that can cause shoulder pain. Therefore, it is advisable to consult a specialist immediately instead of trying to find the cause on your own.
It can take two to three days to diagnose arm pain. The first step is to be examined by a neurologist and to use the usual clinical methods (tests, X-rays, MRI) and special techniques to determine the exact extent of nerve damage - electromyography and electroneurography.
These methods are used to study the electrical activity of muscles and the speed of nerve impulses. By combining the results of both methods, it can be determined whether the nerve has retained its function or whether it has degenerated and been replaced by connective tissue. The method of treatment depends on the results of the test.
CONSERVATIVE TREATMENT
In the initial phase, conservative treatment is recommended in all cases of Morton's neuroma. Patients are advised to wear shoes with a wide toe and low heel. Soft pads or a custom-made orthotic can be used to relieve pressure on the painful area.
Nonsteroidal anti-inflammatory drugs may be prescribed to relieve pain. Physiotherapy in the form of ultrasound or electrical stimulation can be effective in some cases. Injecting a corticosteroid into the space between the toes together with a local anesthetic for diagnostic purposes allows for a fairly long-lasting effect in some cases.
If conservative treatment is unsuccessful over a long period of time and other possible causes of foot pain are ruled out, surgical treatment may be indicated.
SURGICAL TREATMENT
There are several surgical treatment options for Morton's neuroma that involve resection of the affected nerve area.
Another surgical option is to loosen the interdigital ligament and remove the scar tissue.
Nerve resection is a radical method of treating the condition, but it's important to remember that it can result in permanent loss of sensation in the area of nerve innervation and the development of a true stump neuroma, which also causes problems for the patient.
causes of pain
Neuropathic pain is not caused by irritation of the pain receptors, but by impairment of the integrity of the nerve endings or the nerves themselves (sensory, motor, vegetative). The neural network is part of the peripheral nervous system, which is found throughout the body.
- a nerve – mononeuropathy;
- multiple nerves in a limited area - multifocal neuropathy;
- multiple peripheral nerves – polyneuropathy.
When one or more nerves are damaged, impulse conduction is also disrupted. Neuropathic pain has a multifactorial origin. Metabolic disorders, chronic infections, vitamin deficiency, trauma, poisoning with toxins (poisons, drugs, heavy metals, alcohol) can contribute to the destruction of nerve fibers.
Other causes of neuropathy include:
- Diabetes. Diabetes mellitus is characterized by a metabolic disorder and abnormal vascular changes caused by consistently high blood sugar levels. This condition can be corrected with diabetes medications.
- Varicose veins of the lower limbs. The occurrence of neuropathic pain is associated with a chronic disruption of blood circulation and blood supply to nerve fibers.
- HIV, AIDS. Antiretroviral drugs are quite toxic.
- herpes. A severe course of infection leads to irritation of the nerves in the area of \u200b\u200bthe rash - herpetic neuralgia.
- Multiple sclerosis. The disease is characterized by focal destruction of the myelin sheath of nerve fibers.
- chronic alcoholism. The nerve endings are destroyed by toxins. Alcoholic drugs can help.
- Osteochondrosis, disc protrusions and herniations. The main cause is compression of the spinal nerve roots.
Other causes of neuropathy can include:
- operations;
- trauma (bruises, fractures, lacerations, lacerations, sustained tissue compression);
- chemotherapy, radiotherapy;
- Pregnancy;
- autoimmune diseases.
Associated Symptoms
Patients with neuropathic pain syndrome have an impairment (loss) of the ability to adequately perceive stimuli emanating from the external environment or from their own tissues. This impairment results from the neurons' ability to process, store and relay information from the receptors to the central analyzer.
This leads to insufficient sensation:
- Dysesthesia - itching and burning sensations;
- paresthesia - a feeling of goosebumps running through the body;
- Allodynia - severe discomfort that occurs after stimuli that do not cause pain in a healthy person;
- Hyperalgesia - hypersensitivity to noxious stimuli.
The type of sensation depends on which nerve endings have been damaged. The severity of symptoms increases at night (at rest), so patients with neuropathy often suffer from insomnia.
Neuropathic pain is often accompanied by these symptoms:
Patients have diminished or lost sensation, leading to trophic changes in tissues.
prevention
Trigeminal neuritis is a disease that needs to be treated early. To prevent their development or possible recurrence, attention should be paid to preventive measures – these include:
- Avoiding trauma to the face and head;
- Avoid hypothermia, especially on the face, and do not wear hats or scarves in winter;
- Avoid drafts; turn off the air conditioner when you sleep or work;
- Visit the dentist twice a year for a check-up and have dental problems treated in good time;
- Avoid stress, anxiety and worries.
Trunk neuralgia is a complex and persistent disease that brings with it a lot of unpleasant moments. It is treatable in most cases, especially with early diagnosis, effective diagnostics, and a well-designed treatment and rehabilitation plan. If the inflammatory process affecting the trigeminal or trigeminal nerve is accompanied by dental disease, a visit to the dentist is necessary. In most cases, the prognosis is positive, since the function of the nerve is fully restored after treatment.
PROPRICUS Clinic offers treatment of trigeminal neuralgia under the guidance of experienced specialists. The cost of treatment is calculated individually, on average from 25,000 rubles.
Treatment of occipital neuralgia with herbal medicines
Medicinal plants can be used as an additional method of treatment, but are not considered the main therapy. The doctor treating the patient must monitor the use of herbal medicines.
The following herbal remedies can be used for treatment:
- Baths with a collection of medicinal plants: dried leaves of oregano, thyme and mint are crushed, mixed thoroughly and poured over a glass of warm water. The resulting solution is strained through a fine cloth and added to the bath. It is recommended to take a bath with the medicinal collection every day before bedtime.
- Beetroot ear drops: Peel the beetroot from the skin, grate on a fine-mesh grater and squeeze out the juice. Put the pure juice obtained in this way as drops in the ears 2 to 3 times a day.
- St. John's wort tea: A tablespoon of dried herb leaves are poured with 250 ml of boiled water and left to steep for 10 minutes. St. John's wort tea can be drunk three times a day without fear of overdose. Sun exposure should be avoided as much as possible during treatment with this herb, as prolonged sun exposure can have negative effects on the skin and cause allergic reactions.
- Topical Mustard Poultice: The powder of the mustard plant is brewed with boiling water to form a thick paste and after cooling it is placed on a dry napkin and applied to the affected area. To enhance the warming effect, the painful area is additionally wrapped in a scarf or other warm material.
prognosis for recovery
The prognosis for a full recovery of a patient with occipital neuralgia depends on how early the patient seeks qualified medical care and what etiological factors play a role in the development of the disease. With significant organic or traumatic damage to the occipital nerve root structure, the prognosis for full recovery is very difficult.
In the early stages, the disease can be successfully treated with conservative methods.
Read more:- Syndrome of the tibial nerve.
- Innervation of the lower leg muscles.
- Tarsal Tunnel Syndrome.
- heel nerve.
- Long fibula muscle.
- Medial tibial strain syndrome.
- Tibialis posterior muscle.
- peroneus muscle.