If you need professional help with lower limb pain, schedule a free consultation with an orthopedist at our chiropractic clinic. During your visit, the doctor will diagnose the problem and explain all the treatment options in your case.

- Stress fractures of the lower leg and foot
- Epidemiology/Etiology
- What is PTSD?
- Premium care: What modern diapers can do
- A bit of history
- causes
- pathogenesis
- Tibialis muscle syndrome
- Tibialis Nerve Syndrome
- Diagnosis of tibial neuritis
- Treatment of inflammation of the tibial nerve
- Over and beyond
- Peripheral Nerve Diseases
- causes
- Secondary Causes
- symptoms
- causes
- symptoms
- causes
- Treatment
- Clinical manifestations and diagnosis of the disease
- Treatment of complex regional pain syndrome
Stress fractures of the lower leg and foot
Stress fractures occur in bones that are subject to mechanical fatigue. They result from excessive, repetitive, submaximal loading that creates an imbalance between bone resorption and bone formation. The fractures usually occur at the point of greatest stress; this is referred to as 'fracture formation'. If this microscopic fracture is not healed and subjected to further loading, the microfracture enlarges and the break becomes larger. This enlargement can be the cause of a macroscopic bone fracture.
Epidemiology/Etiology
It is estimated that 15-20 % of traumatic hyperextension fractures are stress fractures. This type of fracture is associated with physical activity that involves constant exertion (such as running or walking). Approximately 50 % of hyperextension fractures occur in the tibia; however, a hyperextension fracture can occur anywhere. The foot (particularly the second metatarsal) is another common site for stress fractures. It has been found that women are 1.5 to 12 times more likely to develop stress fractures than men.
Georgy Temichev's seminar 'Diagnosis and Therapy of Lower Limb Problems'. Gait and run analysis'. Learn more…
Stress fractures can be caused by a number of factors, such as: B. by activity level, bone strength, anti-inflammatory drugs, radiation, nutritional status, osteoporosis, hormonal imbalances, lack of sleep and collagen abnormalities. Stress fracture recurrence depends on bone chemistry, adjacent muscle attachments, vascular network, systemic factors, and exercise regimen. Other possible risk factors include age, gender, footwear, and exercise regime. Female athletes are particularly vulnerable to the athletic 'triad' (amenorrhea, eating disorders and osteoporosis), but male endurance athletes with abnormally low sex hormone levels are also at risk of fractures.
From a biomechanical perspective, stress fractures can be caused by muscle fatigue that overloads the bone. In addition, the position of the components of the lower limbs is also believed to influence the risk of stress fractures. In addition, early studies have shown that small tibial thickness, high external rotation of the thigh, varus and midfoot alignment of the ankle, hyperpronation of the ankle, pes cavus, and leg length discrepancies may increase the risk of stress fractures in athletes (the data are for some factors inconsistent).
What is PTSD?
According to the modern definition, post-traumatic stress disorder (PTSD) is the result of a strong negative impact on a person's psyche, either once or over a long period of time. Physical or sexual abuse or being present without being able to intervene, threats to life and health, feelings of helplessness and other psycho-traumatic events often leave consequences that are very difficult to cope with.
Symptoms of PTSD include. constant preoccupation with what has happened, inability to 'switch off' from difficult memories, nightmares and the associated insomnia - the person concerned is simply afraid to go to sleep because the past can inevitably build up unhealed emotional wounds during sleep. There is intense anxiety, dissociative reactions and sometimes amnesia as the brain tries to distance itself from the painful memories in order to 'erase' them from memory.
PTSD may not appear immediately, but many months or even years after the traumatic events. Panic attacks, depression and suicidal thoughts associated with PTSD can 'delay' development.
There are also abnormalities in how the brain processes information. When a situation occurs that even remotely resembles the circumstances of the trauma, the body can reflexively trigger a protective reaction that is beyond the control of reason, ie independent of the person's will.
According to statistics from the US, mentally traumatic circumstances lead to the development of PTSD an average of 30 percent of the time, and 60 percent of those affected have trauma symptoms that persist for up to a year after the trauma.

Premium care: What modern diapers can do
A bit of history

Although PTSD is a recent phenomenon, an examination of historical records suggests that it is not a 'modern invention'. Symptoms very similar to PTSD have been described since ancient times.
In the writings of Herodotus, who lived in the fifth century B.C. There is an account of a case in which a warrior who had survived the horrors of the Battle of Marathon went blind. The French king Charles IX, who ordered the outbreak of the Bartholomew massacre, complained of haunting nightmares and horrific visions. Napoleon's army doctors described 'cannonball syndrome', a state of drowsiness in soldiers when a cannonball flew near them. In the United States during the Civil War, doctors described 'soldier's heart syndrome' - a heart condition caused by nervous exhaustion and anxiety.
The 'traumatic neurosis' was first mentioned in 1888 by the German physician G. Oppenheim. Articles soon appeared describing similar symptoms not only in people involved in combat operations, but also in victims of other disasters - such as railroad accidents or natural disasters. Doctors then discovered a similarity between the symptoms of traumatic neurosis and the effects of childhood trauma when the child experiences intense anxiety.
And then World War I broke out, and tens of thousands of soldiers became so psychologically traumatized that many lost their ability to see, hear, remember, and walk. Some of these symptoms were the result of a concussion, but some were not physically damaged, just neurologically impaired. The English psychiatrist Myers called this phenomenon 'shell shock'.
World War II brought even more misery. Symptoms of what is now referred to as PTSD have been observed not only in military personnel or residents of the occupied territories, but also in concentration camp survivors, survivors of the Siege of Leningrad, residents of Japan, and survivors of the atomic bombing of Hiroshima and Nagasaki.
causes
The predominant etiological factor is atherosclerotic damage to the subclavian segment. Rare causes of stromal syndrome include Takayasu's arteritis, aortic dissection, and external compression. The latter can be caused by anterior lumbar muscle syndrome or the presence of an extra cervical rib. Etiological factors include anatomical vascular anomalies, deformation of the vascular wall, in some cases due to degenerative changes. Rare variants of congenital stromal syndrome have been described.
The risk factors are similar to those of atherosclerosis and include:
pathogenesis
Subclavian stromal syndrome is often associated with extensive stenosis and/or occlusion of the subclavian artery, resulting in decreased pressure in the artery distal to the lesion. The more frequent occurrence of a left-sided lesion is explained by the fact that the acute angle of the left subclavian artery increases turbulence and accelerates the development of atherosclerosis at the confluence with the aorta.
The arm that is supplied by the diseased artery has reduced blood flow. When the blood supply deficit is exacerbated by exercise, blood begins to flow from the ipsilateral vertebral artery to maintain adequate circulation. The result is a reversal of blood flow in the vertebral segment on the affected side. Blood drains from the basilar vessel in the posterior fossa, which supplies blood to the trunk, the temporal-occipital parts of the brain, and the cerebellum. Ischemia occurs in these brain regions, which manifests itself clinically as vertebrobasilar symptoms.

Tibialis muscle syndrome
Another condition associated with tibialis muscle syndrome is foot deformity and inappropriate choice of footwear for exercise and regular wear. Both adults and children are affected by this disease.
The main causes of tibialis muscle syndrome are:
- contractures, including ischemia with long-term microvascular impairment;
- Traumatic impact, e.g. B. Contusion with formation of a hematoma in muscle or between muscle and fascia;
- Malpositions or curvatures of the spine, leading to an uneven distribution of physical stress on the muscular skeleton and lower limbs;
- Stress, increased nervous tension, chronic fatigue, lack of sleep, etc.;
- myofascial pain syndrome;
- restless legs syndrome, which usually manifests itself at night;
- Osteochondrosis of the lumbosacral spine with radicular syndrome and impaired innervation of the lower limbs;
- Excessive physical stress on the legs (people who lift weights, men who do physical work, women who have to stand for long periods at work);
- Myofascial syndrome and other types of sciatic nerve compression;
- Myositis, including infectious origin, developing against the background of acute infectious diseases of the internal organs;
- Accumulation of lactic acid and other metabolites in the muscles, which are broken down during exercise;
- foot deformity (flatfoot or clubfoot);
- unsuitable footwear for running, sports and everyday walking.
All of these causes can trigger primary tibialis muscle syndrome. If pain and symptoms of inflammation go unnoticed, a large cyclic deformity can develop in the near future, leading to impaired tibia function.
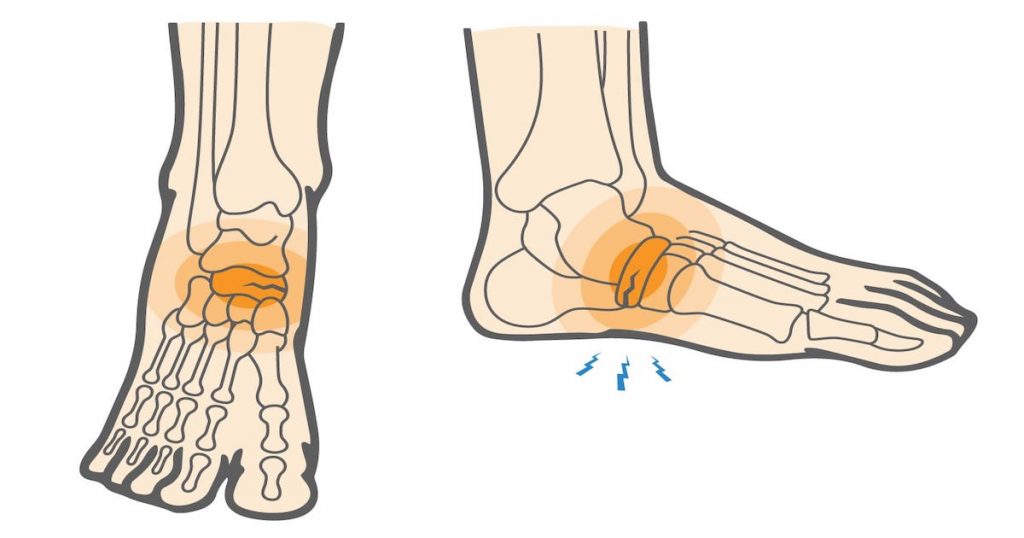
Tibialis Nerve Syndrome
Tibial tunnel syndrome also causes pain. However, the location of the discomfort largely depends on where the nerve is pinched. Tibial tunnel syndrome is most common in people who are used to sitting with one leg over the other.
The sciatic nerve runs along the back of the thigh to the back of the knee (popliteal fossa). At this point, it branches (divides) into two branches: the tibia and fibula. The first branch on the outside of the tibia and the second branch on the inside of the tibia are directed toward the heel, followed by several branches of each branch. As such, they are responsible for the innervation of foot tissue.
Tibial nerve syndrome is compression of its tissues in the tarsal canal due to hypertrophy of scar tissue. It can be caused by trauma, osteoarthritis of the knee, a shin deformity, flat feet, clubfoot, obesity, etc.
Diagnosis of tibial neuritis
Damage to the shin nerve (tibialis neuritis) leads to paralysis of the muscles that flex the foot and toes (plantar flexion) and rotate the foot inward. A neuralgia of the tibial nerve leads to a loss of the Achilles reflex.
Sensory disturbances in tibial neuralgia occur on the posterior surface of the tibia, sole, sole surfaces of the fingers and dorsum of the terminal phalanges. The musculo-fascial sensation in the fingers is unaffected when the peroneal nerve is functioning (it is only affected when both nerves are affected, ie the peroneal nerve and the tibial nerve or the main trunk of the sciatic nerve).
The muscle wasting associated with tibial neuromas is usually significant and affects the posterior muscle groups of the lower leg and sole of the foot (lowered arch, regression between the toes). The foot is in a stretched position. Gait is impaired, but to a lesser degree than in the dorsally flexed heel foot; in this case, due to the extensibility of the foot, the patient walks in heels.
The extent of damage to the tibial nerve in neuritis is diagnosed by electronography (ENG).
Tibial nerve disorders can be diagnosed by electronography (ENG):
Pain from inflammation of the tibial nerve (and its fibers as part of the sciatic nerve) is often very intense.
Injuries to the tibial nerve and its bundles in the sciatic nerve trunk can cause a causal syndrome. Vascular and secretory-trophic disorders are also usually important. In this regard, there are some similarities between the tibial nerve and the median nerve.
Treatment of inflammation of the tibial nerve
The treatment of shin splints is recommended for each patient individually. It includes a complex of conservative treatments:
Acupuncture is very effective in treating shin splints.
Neurostimulation (physiotherapy) eliminates paresthesia and pain and restores muscle strength in tibial neuritis.
Over and beyond
Peripheral Nerve Diseases
- Anatomy of the nervous system
- Leg pain (osteochondrosis, herniated and protruding discs, radiculitis)
- Shoulder and neck pain (injuries, osteochondrosis, cervical radiculitis)
- The eyeball and the visual pathway:
- Anatomy of the eye and physiology of vision
- The visual pathway and its disorders
- Structures of the eye and the visual disturbances that occur when they are damaged
- Retina and optic nerve head, visual disturbances that occur when they are damaged
- Eye movement disorders
- Nystagmus and nystagmus-like states
- Meningiomas of the optic nerve sheath
- Optic Nerve Arachnoiditis
- atrophy of the optic nerve
- Inflammation of the optic nerve in adults
- Optic neuritis in children
- Ischemic Optic Neuropathy
- Compressive optic neuropathy
- Edema of the Optic Nerve Head
- Pseudoedema of the Optic Nerve Head
- Toxic gastrointestinal optic neuropathy
causes
Not only injuries or illnesses can lead to complaints and dangerous consequences. Working in an awkward hand position can trigger this pathology and lead to tunnel syndrome.
Hand injuries, lack of mobility, or sensory disturbances in the hand raise suspicion of neuropathy of the median nerve of the upper limb. The abnormal condition has several causes.
- Bundle compression in the narrow canal between the muscles of the forearm and hand. This affects not only the wrist, but also the skin of the hand and fingers I-IV.
- Toxic affliction. Caused by regular alcohol consumption, drugs or chemical poisoning.

- Rarely from long-term use of neurotoxic drugs. The nervous tissue gradually deteriorates and ceases to perform its function.
- A hand injury with isolated bundle damage leads to the development of post-traumatic mononeuropathy (neuropathy) of the median nerve. Soft tissue, muscles and ligaments can be damaged deep and over a large area. In some of these patients, the problem can be solved, including through surgery. However, sometimes it is not possible to restore the nerve fibers to their original state.
- Diabetes. If the blood sugar level is too high, the nerve fibers lose their ability to function. An irreversible process of degeneration takes place in them.
It is possible that the tunnel neuropathy of the median nerve in the hand is accompanied by inflammation, the treatment of which can only be recommended by a doctor. Multi-joint inflammation occurs, for example, when the small joints between the forearm and hand are inflamed.
Secondary Causes
In addition to the main causes mentioned above, certain diseases and pathological processes can also trigger the problem:
symptoms
Compression neuropathy (neuropathy) of the median nerve in the upper limbs is considered the most common condition caused by stretching and swelling of the muscles between which the nerve bundle passes. It's important to realize that the median nerve is long and radiates from the shoulder. He can be greatly damaged.
The severity and dynamics of clinical symptoms depend on the cause of damage. Trauma and compression, such as in carpal tunnel syndrome, cause acute disruption of innervation to the hand. Diabetes, on the other hand, is characterized by a gradual deterioration in nerve function.
Mononeuropathy of the median nerve is characterized by:
- decreased sensitivity of the skin in the middle of the hand, from the thumb to the ring finger;
- a drawing pain in the wrist;
- a burning sensation in the same area;
- The fingers can no longer be bent;
- grip strength decreases;
- Muscle atrophy occurs over time.
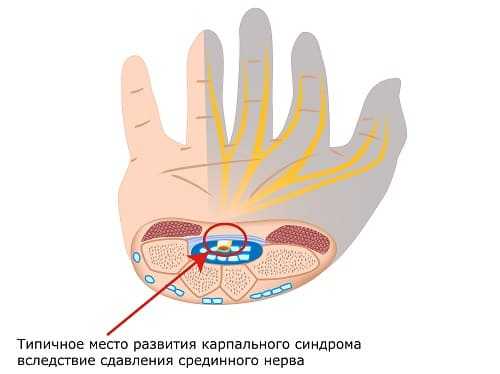
Only the branches that provide sensitivity to the back of the hand pass through the carpal tunnel. Therefore, the skin sensitivity on the palm of the hand is rarely affected.
Sensory neuropathy of the terminal branch of the left or right median nerve is characteristic of the early stages of the pathology, when only the sensitive branches are damaged. Unpleasant sensations in the hand can even lead to waking up at night. The hand feels numb, burns and tingles. Symptoms subside when the hand is shaken but return and worsen when the hand is bent or flexed.
The appearance of motor disorders, preceded by sensory disorders, indicates the progression of the pathology. In injuries where the thicker part of the hand is injured (fractures of the shoulder and forearm), sensory and motor disorders occur simultaneously.
causes
Fibula canal syndrome is most commonly diagnosed in people whose jobs require prolonged kneeling or standing. Therefore, it is most commonly found among furniture assemblers, builders, farmers, etc.
In contrast, habits such as: sitting on the other leg for long periods; sitting for a long time with one leg pulled over the other; sitting for a long time with the other leg pulled over the other; long sitting with the other leg pulled over the other:
- Sitting with one leg dragged over the other for long periods of time;
- Sitting in the wrong size chair with your legs dangling;
- sleeping with bent legs hanging over the edge of the bed;
- sitting in a chair with your legs drawn up for a long time, as is common for many office workers.
Direct trauma to the knee joint, fibula head, or immobilization of the limb with a cast as a result of fractures, dislocations, certain surgical procedures, etc. can also cause fibula canal syndrome. Also, inflammatory muscle diseases, tumors in the knee area, bruises and swelling of the lower limbs caused by the development of certain pathologies lead to nerve compression.
symptoms
A pinched foot nerve is accompanied by specific symptoms:
- sensory disturbances of various kinds, particularly numbness, tingling, tingling, burning on the outer surface of the shinbone and dorsum of the foot, involving the first interdigital space but not the big toe, and tending to disappear with walking and moving the foot;
- peripheral paresis (muscle weakness) of the extensor muscles of the foot, resulting in a wobbly foot, gait abnormalities, decreased stability while walking, and frequent stumbling while walking, forcing the patient to lift the affected foot with each step, known as 'houndstooth' ;
- inability to draw the toes of the foot together;
- Pallor, dryness and coldness of the skin on the lower leg and foot.
In most cases, sensory and other disturbances are observed within 1 to 24 hours, but they can also occur much longer, even lasting 10 days or more.
The disease tends to be insidious. If not treated early, the sensory disturbances are accompanied by pain. The pain can be burning or stabbing. However, with increasing muscle weakness, it decreases and is replaced by a sharp bending of the foot when walking. The muscles of the lower leg then shrink (atrophy), which is visible to the naked eye in severe cases.

causes
Important factors for the development of Baastrup syndrome are Increased lumbar lordosisThis is caused by increased lumbar lordosis, regardless of the cause.
With increasing lumbar lordosis, which reduces the radius of curvature of the lumbar spine formed by the vertebrae, the posterior vertebrae converge. The spinous processes begin to touch, which initiates the disease process. Touching the edges of the spinous processes provokes an increase in the size of the spinous processes, contributes to the formation of new articular surfaces, cartilage formation, capsule formation and even a synovial cyst.
If this is accompanied by frequent, rapid, and repetitive stiffening of the lumbar spine.This creates direct contact between bones that would otherwise be cushioned by the ligaments between the spinous processes. There is a predisposition to rupture, impingement and acute low back pain.
Also Wear of the intercondylar ligaments may be a key process in the degenerative manifestations of Bastrop syndrome.
Treatment
In general, the following types of treatment of Bastrup's syndrome are distinguished:
- Initial treatment is conservative and symptomatic: painkillers and/or nonsteroidal anti-inflammatory drugs and rehabilitation.
- If this fails, injections into the intercondylar bursa with echography can be done, usually with very good results.
- Several surgical procedures are known to reduce the intensity of symptoms, with inconsistent results.
– According to Filum System®:
Bastrup syndrome is very common in patients with terminal fiber disease. The tension forces occurring in this disease also affect the spinous processes of the vertebrae, overloading them and contributing to osteoarthritis. In addition, with or without idiopathic scoliosis, there may be an increase in lumbar lordosis, causing degenerative disease of the spinous processes. For this reason, before treating osteoarthritis, we carry out a Filum-System® diagnosis to detect the presence of spinous process disease that should be treated first.
Clinical manifestations and diagnosis of the disease
Patients suffering from complex regional pain syndrome have pain in a limb. It can be a burning, aching pain in combination with sensory and vegetative disorders (swelling, skin discoloration, local skin temperature changes, sweating). Hair and nail growth is disturbed, local osteoporosis and movement disorders occur.
Most often, symptoms of complex regional syndrome appear immediately, a few days or weeks after injury, rarely as long as a month after injury. The first stage of the disease lasts 2-3 months. It is characterized by a pain syndrome of varying intensity. Patients suffer from stabbing, throbbing and burning pain. It increases with movement, touch, weather changes or excitement, and excessive heat.
If not controlled, the pain becomes constant and annoying. Patients must immobilize the limb with a bandage or support it with a good arm. The pain can spread to the entire arm and shoulder joint, and in some cases to that side of the body as well. The patients have doubts about their recovery and suffer from insomnia.
Massive swellings form on the back of the hand or foot and in the lower third of the forearm or lower leg. Initially it has the consistency of a cake, later it becomes thick. Some patients only suffer from pain. They may not have any discoloration or swelling.
The second stage of the disease develops after 3-6 months. The pain decreases, the joints of the hand or foot become stiff, and the interphalangeal and metacarpophalangeal joints become stiff. The following skin changes are characteristic of this stage:
- loss of elasticity,
- Hypertrophy;
- transition from initial congestion to blueness or pallor;
- Gradual increase in atrophy, dryness, shine.
Treatment of complex regional pain syndrome
The first phase of treatment for complex regional pain syndrome is primarily about controlling the acute pain. It consists of good pain management. Analgesics and traction are administered. In the second phase, rehabilitation treatment is reserved for patients who are not yet able to return to work. This will ease the transition from initial treatment to a normal lifestyle. Psychologists at Yusupov Hospital also work with patients. In the third phase, doctors apply an individualized intensive complex treatment.
In the treatment of complex regional pain syndrome, doctors use the following drugs:
In most cases, a good effect is obtained when rational combined drug therapy is combined with rehabilitation measures. Patients with complex regional pain syndrome are prescribed anticonvulsants by doctors at the Yusupov Hospital. The most effective drug is gabapentin. It shows a moderate to significant effect after eight weeks of treatment. Carbamazepine significantly reduces pain intensity.
Antidepressants have a pain-relieving effect. In the early stages of the disease, neurologists conduct pulse therapy with high-dose corticosteroids. Treatment is most effective when there is marked inflammation.
Bisphosphonates reduce inflammation, pain, and swelling. They are effective at all stages of the disease. The doctors of the Yusupov Hospital individually select the optimal dosage of drugs and determine the duration of treatment. Calcitonin has an analgesic effect. It also helps prevent osteoporosis. With moderate pain accompanied by swelling and autonomic dysfunction, a short course of nonsteroidal anti-inflammatory drugs (Ibuprofen, Voltaren, Movalis) is carried out. If the pain is severe, these drugs are not very effective.
- Tibialis posterior muscle.
- Syndrome of the tibial nerve.
- Innervation of the lower leg muscles.
- fracture of the elbow in the foot.
- Medial tibial ankle joint.
- shin tendon.
- Medial sphenoid of the foot.
- Tendon of the tibialis anterior muscle.