If this condition were a danger to young children, it would probably be taken more seriously in schools and hospitals. But the ailment is not dangerous and does not require special treatment. Therefore, not recognizing them is not a crime, because in this case a medical 'mistake' has no dangerous consequences.

- Cerebral Palsy: Can It Be Cured?
- Why does cerebral palsy occur?
- Prenatal causes (during pregnancy)
- Perinatal causes (during labour)
- Neonatal problems (first 28 days of life)
- outside of maternal life
- statistics
- etiology of the disease
- Symptoms of valgus deformity in adults
- Causes of valgus
- pathogenesis
- symptoms
- Treatment of foot deformities.
- Treatment of foot deformities using the 'plaster correction' method.
- plaster correction.
- Foot deformities are treated with a plaster cast!
- Ivanov Yaroslav Vyacheslav
- What is it and ICD code 10
- Causes and symptoms of foot adduction
- Treatment
- prophylaxis
- Treatment
- prophylaxis
- Symptoms of contractures in children
- Treatment of contractures in children
Cerebral Palsy: Can It Be Cured?
Let's find out what is the cause of brain dysfunction, and therefore the diagnosis of cerebral palsy, and how to deal with it.
Cerebral palsy is a permanent neurological disorder caused by non-progressive damage to a child's brain.
The brain controls all bodily functions, including muscle movement. Cerebral palsy is damage or malformation of a child's nervous system that begins before, during, or shortly after birth to affect the development of motor skills, posture, and muscle tone.
Symptoms range from mild, which one can live with, to severe, which cannot be managed without help.
With mild cerebral palsy, there may be a slight limp in the arm or leg that is barely noticeable to others. With severe cerebral palsy, it can be very difficult to perform everyday activities, maintain posture, and maintain neuromuscular activity.
The rate of cerebral palsy worldwide is 2.5 per 1,000 successful births. Diagnosis of cerebral palsy is usually made by the age of 2 based on clinical signs. Earlier diagnosis is possible based on history, medical evaluation, and magnetic resonance imaging (MRI) or computed tomography (CT).
Why does cerebral palsy occur?
Cerebral palsy has been found to be more common in underweight or weak infants, in asphyxia (shortness of breath) during childbirth, premature detachment of the placenta, abnormal positioning of the fetus during pregnancy, or fetal presentation during childbirth (direction of the head toward the mother's 'exit' ) and other causes.
Prenatal causes (during pregnancy)
- congenital malformations of the brain
- negative vascular events, such as B. occlusion of the fetal middle cerebral artery;
- certain genetic syndromes;
- metabolic disorders;
- maternal ingestion of toxic substances, including alcohol;
- maternal infections in the first or second trimester of pregnancy, such as rubella, cytomegalovirus and toxoplasmosis.
Perinatal causes (during labour)
- Fetal hypoxia due to difficult childbirth, umbilical cord prolapse, prenatal bleeding and other causes;
- injuries during childbirth;
- Fetal metabolic acidosis – an abnormality in the acid-base composition of the baby's blood;
- Encephalopathy (brain damage) in the newborn.
Neonatal problems (first 28 days of life)
outside of maternal life
The above causes only increase increase the likelihood of Occurrence of cerebral palsy. However, the more adverse events that occur during pregnancy, childbirth and/or thereafter, the greater the likelihood of cerebral palsy.
statistics
Various defects of the musculoskeletal system are more common in debilitated children who have previously suffered from rickets (a bone disease associated with disorders of mineral metabolism and bone formation) and who are ill frequently and for a long time. Poor exercise capacity is also a risk factor for developing pes valgus.
A mild deformity occurs in 70 % of children up to 4-5 years of age. In the vast majority of children, the musculoskeletal system and ligaments develop to the required level and gait becomes straighter.
Forefoot adduction in children usually occurs in connection with an O-shaped curvature of the tibia. True clubfoot is much rarer.
Among congenital orthopedic deformities, the pathology in question occurs with a frequency of 2-6 %.
etiology of the disease
There are three main known causes of clubfoot:
- Deformity of the tarsal bone (tarsalvarus). Remodeling of the movable forefoot.
- It occurs in newborns.
- Autocorrection (passive) possible.
- Correct heel alignment.
- Does not require treatment.
- Internal torsion (rotation around its own axis) of the tibia. The shin twists less from the hip than it normally should. Muscles, ligaments and joints are affected by this misalignment.
- It occurs in a child who begins to walk.
- A combination with a knee deformation is possible.
- Developmental tendency: Disappears spontaneously by the age of 5 years.
- Persistent anteversion of the femoral neck. The bone tilts forward more than normal.
- Starts at a young age.
- Worsens by age 8. Usually does not require treatment.
- The twisting of the ligaments causes hypermobility of the joints.
Predisposing factors for foot deformity in children:
- Genetic predisposition to this pathology.
- Inflammatory processes in the tissues of the foot.
- Pathology of the fibula nerve. The innervation of the joints is disturbed. This form of pathology is called neurogenic.
Symptoms of valgus deformity in adults
The main symptom of the pathology is foot deformity. The patient's shins twist into an X shape and the foot is flattened. The patient feels disturbed by this condition:
- pain in the feet, which increases after standing and walking for a long time;
- swelling of the ankles;
- blisters on different parts of the foot;
- Gait deviations and lameness.
Hallux valgus is often associated with an outward deviation of the big toe.
Causes of valgus
At the heart of the development of this pathology is the rotation of the talus in the sagittal (medial) and horizontal planes. This leads to a flattening of the arch of the foot and a change in its support points. These changes can be caused by many factors. They usually occur together and rarely have an isolated effect. The development of a valgus can be the result of:
- overweight;
- hypodynamics;
- neurological disorders;
- genetic predisposition;
- congenital anomalies of the foot;
- progression of any type of flatfoot;
- osteoporosis (brittle bones due to calcium deficiency);
- Injuries to the lower limbs, especially the ligaments and bones of the feet;
- hormonal imbalance associated with menopause, pregnancy or endocrine disorders;
- regular overuse of the feet due to heavy physical work, walking or standing for long periods.
Wearing high-heeled shoes or shoes that are too tight to distribute the load on the foot can also promote foot pathology.
pathogenesis
Disorders of the anatomy of the hip joint already arise in the uterus. After birth, the hip joint can spontaneously move out of the acetabulum. This happens because the posterior superior rim of the acetabular cup is deformed — instead of having a sharp edge that helps hold the femoral head in the acetabular cup, the rim is flattened, allowing it to shift. Inward and outward displacement causes a dislocation and a clicking sound.
Most hip joints that are unstable at birth can set themselves back into place and develop normally. However, some joints with abnormal anatomy do not align properly and remain outside of the acetabulum. When a hip dislocation occurs, the acetabulum remains empty. The body cannot tolerate emptiness, so the bottom of the hip socket begins to fill with fat. The longer the joint remains dislocated, the more difficult it becomes to reset, as the fat padding in the acetabulum prevents the joint from aligning normally.
symptoms
Diagnosis of joint dysplasia is based on clinical, ultrasonographic, and radiographic findings. An unstable hip may stabilize spontaneously, remain dysplastic, or change the proportions of the joint over a period of several months.
During the examination, the specialist must assess the parameters of the joint and determine the movement in the joint. A relaxed and calm child is essential for a successful exam. A bottle or dummy may be needed for this purpose.
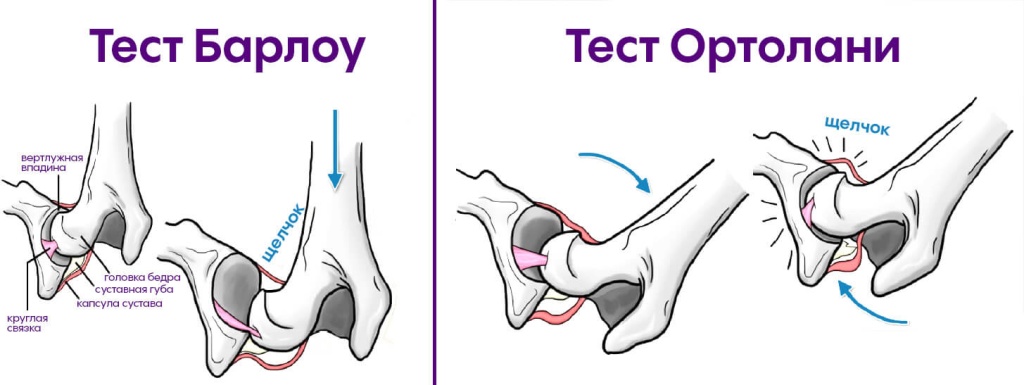
Barlow's test – provocation test. In this test, the doctor attempts to dislocate the femoral head from the acetabulum. Technique: The hip is brought to the side and the doctor gently pushes the femur backwards. The physician's finger is placed back on the acetabular major and the acetabular major can be moved outward. The sign is considered positive when the head comes out of the hip socket, when the doctor relaxes his hands - it comes back in.
Ortholani test – Reverse Barlow test. With this test, the doctor tries to reduce the displacement of the femoral head. The doctor holds the child's femur between the first and second fingers, uses the remaining fingers to elevate the thoracic spine, and abducts the femur. The test is considered positive when the femoral head is pushed back into the acetabulum, with a characteristic 'click' sound that can be felt under the hands but not heard. These operations must be repeated several times to determine the symptom. These tests are performed in the neonatal period.
Once the infant is 3-4 months old, other signs of dysplasia appear. This is important to understand the progression of the pathology. Signs of joint dysplasia in infants include: restriction of joint abduction, hip shortening, external alignment of the greater trochanter, and butt signs.
Galeazzi test – Hip shortening test. To evaluate the hip shortening test, the hips are flexed 90° and the level of knee joint protrusion is compared. In the case of a unilateral joint dislocation, an asymmetry of the hip joint position towards the healthy side is determined.
Treatment
foot deformities.
Treatment of foot deformities! Make an appointment for a consultation with Dr. Ivanov, orthopedist and surgeon. B.
Treatment of foot deformities using the 'plaster correction' method.
Allows stretching of soft tissues in childhood when they are not yet 'hard' and have not yet formed fixed deformities in the joints.
plaster correction.
It is not only a method for treating fractures, but also for Treatment of foot deformities. It can correct lower limb deformities in children with toe walking, congenital clubfoot, paresis and paralysis.
However, unlike the cast for fractures, when treating foot deformities and contractures (restrictions) of the joints of the lower limbs, the cast is applied gradually. Between 2 and 5-6 plaster casts are required to stretch the soft tissues.
The average length of stay in a cast is 5 to 14 days, after which the cast is changed.
Depending on the cause of the foot deformity, the cast may be short, reaching to the knee (e.g., with toe walking, spastic diplegia, or hemiparesis) or long (in congenital clubfoot, clubfoot) so that the cast does not 'creep', pinch, and cause anxiety when the child moves.
Foot deformities are treated with a plaster cast!
Ivanov Yaroslav Vyacheslav
Turner National Medical Research Center for Pediatric Traumatology and Orthopedics.
Specialization:


Diagnosis is made by ruling out various causes. Thanks to the position created by the plaster cast, the child can no longer tiptoe. This type of cast allows the child to walk on their toes so that they can adapt to walking at home, on the street, and in the learning environment.
There are many reasons for toe walking today:
The diagnosis of idiopathic toe walking is made after ruling out the other forms. Treatment of foot deformity begins with an examination. The examination is mandatory before conservative treatment (casting, stretching, changing shoes) or surgical treatment (Achilles tendon lengthening or calf muscle recessions).
One cause of toe walking is infantile cerebral palsy. Tiptoe walking can occur due to an imbalance in the muscles of the lower limbs. A plaster cast can be used to stretch spastic, shortened muscles. Gradual wearing of a cast can help the child regain a normal gait.

 This condition is often confused with congenital clubfoot. The Achilles tendon is not shortened. A staged cast can correct this deformity in multiple bandages.
This condition is often confused with congenital clubfoot. The Achilles tendon is not shortened. A staged cast can correct this deformity in multiple bandages.
What is it and ICD code 10
Clubfoot is often confused with clubfoot. Viewed from the front, the anomalies are visually similar. To make a diagnosis, the foot should be viewed from the side with the foot in maximum flexion at the joint.
Forefoot adduction is a disorder of the musculoskeletal structures that make up the Lisfranc joint. It can be congenital - an infant is born with this diagnosis - or acquired. Without treatment and as the child ages, the metatarsal bones deform and the space between the first toe and the other toes increases.
This dysfunction occurs in 70 % of children under 5 years old. In the vast majority of cases, it resolves spontaneously as the child ages. Anterior adduction is associated with varus deformity of the tibia or O-shaped feet.
There are 2 clinical forms of foot deformity:
- Simple - the Lisfranc joint is affected and there are no changes to the bony structures. The function is preserved
- Complex – with varus type disorder. The bony structures are distorted, the heel is valgus and motor skills are impaired.
The International Classification of Medicines ICD 10 has given this condition the code Q66.2 - adducted foot.

Causes and symptoms of foot adduction
Adduction of the foot, a disorder of the muscles that control the physiological alignment of the big toe and the ligaments of the inner toe, is caused by an imbalance between the adductors and abductors of the foot.
Factors contributing to the development of the pathological process:
- genetic predisposition,
- a weak, physically underdeveloped child,
- history of rickets,
- Osteoporosis,
- frequent colds and viral diseases,
- inflammatory processes in the joints, ligaments of the leg,
- Disease of the perineal nerve. The innervation of the foot is compromised, leading to stiffness in the muscles and ligaments.
Symptoms are similar to many musculoskeletal disorders. The child may complain of pain on movement and fatigue. When wearing shoes, calluses form and the gait is altered.
- The big toe is turned inwards and the first toe space is enlarged,
- the forefoot is directed inward and rotates outward,
- the metatarsal bones have deviated from their physiological position,
- The arch of the foot is intact and there is no flatfoot,
- heel valgus deformity,
- Dislocations and subluxations of the small joints.
To read: Efficacy of Treatment of Pediatric Flatfoot Deformities Using Conservative and Surgical Methods
Treatment

In rare cases, each disease heals spontaneously. Orthopedic pathology only tends to get worse.
The elimination of the foot requires a comprehensive treatment approach under regular medical supervision. The process is long and complex, and relapse is possible by age 18, when the musculoskeletal system is fully developed.
The most effective treatment. In a newborn, the foot is corrected within a month. Casts (dressings for small deformities) are used in the form of 'shoes' from the toe to the knee joint.
These are needed to improve the transmission of nerve impulses to the foot muscles. In addition, hormones are injected into the joint cavity to eliminate inflammation.
The special technique of toning the lower limbs is best performed in combination with a general full-body massage. Kneading is necessary not only for the legs, but also for the lumbar region of the back.

The training of the musculoskeletal system promotes an even and correct development of the foot tissue.
The most popular is shock wave therapy.
There are now special shoes with an individually adjustable insole and a heel cap that give the foot the right alignment.
Doctors rarely use this method: when conservative treatment is ineffective, when the disease is advanced and at a more mature age. The child can only be operated on from the age of three.
prophylaxis
All the prerequisites for the development of a pes valgus lie in childhood. This defect progresses with age and should therefore be corrected as early as possible. It is even better not to treat, but to prevent the onset of the disease.
Prevention methods focus on comprehensive strengthening of the musculoskeletal system:
- Foot massage and therapeutic exercises in the first year after childbirth.
- Regular and sufficient physical activity for the child.
- Appropriate orthopedic footwear. These help to distribute the pressure along the entire length of the foot.
- Control of the first steps. Parents should check that the child's feet are in the correct position when standing and walking. The ability to walk develops during the first 3 years of a child's life.
Treatment
As you may have guessed, the condition goes away spontaneously and without any specific treatment. It lasts about a week, after which the symptoms do not return. Therefore, at all stages of treatment, the task of parents is to create conditions for the child that will allow the body to heal faster. Bed rest, plenty of warm drinks, no stress and light food, the digestion of which does not require a large amount of energy from the child's body.
Since the main danger to the child is dehydration caused by hyperthermia, must be ensured that the child drinks a lot. If he's not drinking, give him the liquid with a disposable syringe.Run the liquid down his cheek to make him spit less. If they won't drink or vomit all over again, call an ambulance and take the child to the hospital. At the hospital, the child is given a tube or IV fluids to rule out dehydration.
As a rule, however, most parents manage to get their child to drink on their own. What can be given? Tea, compote, homemade nibbles, still mineral water, rosehip decoction, plain clean drinking water.
The most important thing is that the liquid is neither hot nor cold, but preferably at room temperature so that it is absorbed more quickly by the body.
The baby should be fed on demand. If he's not hungry, don't force him.. In infants, during the illness, it is better to refrain from complementary foods and give only breast milk or infant formula, and children over a year old should be given light meals, porridge, mashed vegetables, soups that do not cause too much stress on the body.
The room in which the sick person is located should be ventilated for 10-15 minutes every hour.Even when it's winter outside. Try not to overheat the room, the optimal temperature for a sick child with a high fever is 21 degrees Celsius.
Try to get rid of all warm clothes and warm blankets. Leave it in underpants under a light sheet to avoid hyperthermia. Fever, if painful, can be controlled with an approved antipyretic such as acetaminophen. If this does not help, the child can be given a nonsteroidal anti-inflammatory drug, such as ibuprofen.
prophylaxis
The feedback from the parents shows that they usually only find out about the rubella after the child has become ill. Sometimes signs of antibodies are found in the blood during an immunological test (immunity is acquired for life), and sometimes the mother just reads about the disease and suddenly remembers that something like this happened to them a few years ago. Based on that, the question of prevention would be quite odd. But there isn't. Roseola is almost as unavoidable as at least one childhood diarrheal disease. There is no vaccine against the herpes virus.
So it's worth looking at the disease philosophically, as something inevitable. Remember that rubella only looks scary, but in reality it does not cause much harm to the child's body.
dr Komarovsky explains more about rubella in the following video.
Elena Lisova
Medical assessor, psychosomatic specialist, mother of 4 children.
Symptoms of contractures in children
Among the main symptoms of contractures in children include. an involuntary limitation of joint mobilitywhich expresses itself as follows:
- inability (or difficulty) to perform normal activities of daily living;
- trouble lifting or carrying objects;
- pain during physical activity.
At the same time, other symptoms also appear symptoms:
- staggering while walking
- impairment of movement coordination;
- inability to fully flex or straighten a limb;
- reduction in sensitivity;
- numbness, 'goosebumps', especially after physical exertion;
- tissue swelling;
- deformation of the joints;
- Reducing the length of the affected limb or delaying its development (if the disease is congenital).
Treatment of contractures in children
Doctors such as orthopedists, neurologists and neurosurgeons are usually involved in the diagnosis and treatment of contractures in children. Depending on the suspected causes of the disease and the condition of the child, it may be necessary to see other specialists.
diagnosis As a rule, the diagnosis of contractures is made according to the following algorithm:
- During a face-to-face exam, the doctor checks the degree of restriction and assesses the joints and skin;
- The child's medical history, details of previous injuries and illnesses are considered, and the child's individual physical characteristics are examined, which is important for determining the exact cause of the disease;
- If necessary, the child will be referred for laboratory tests (OAC, OMV, etc.).
If there is suspicion neurogenic contractures The neurologist will assess the child's neurological and mental status.
In addition, additional instrumental investigations:
- X-ray (to clarify the extent of joint damage and restricted mobility);
- Computed tomography (to determine the location of the deformed structures in space);
- MRI (to assess damage to periarticular tissue);
- ECG;
- ULTRA SOUND.
Treatment of contractures in children includes a comprehensive treatment of the body. For minor joint damage, the following treatments are recommended. conservative therapywhich includes:
- physiotherapy (physical therapy, therapeutic massage, ion therapy);
- Plaster casts, which are also associated with straightening the affected joint (if the tissue is still sufficiently mobile).
treatment with medication may be indicated for analgesic, anti-inflammatory and immunological reasons. If the cause of the contracture is neurological, the focus should be on treating the underlying pathology.
Read more:- Clubfoot in children therapeutic exercises 7 years old.
- Toe movement in children.
- Clubfoot in 7-year-old children.
- Footwear for children's clubfoot.
- Why does a child develop clubfoot?.
- Equino valgus.
- Massage for clubfoot in children.
- baby splashing.