Special examination methods are recommended to confirm the diagnosis. The most informative methods are X-rays, MRI and arthroscopy. X-rays show narrowing of the joint spaces and deformation of the joint surfaces. An MRI scan also shows the extent of damage to the cartilage, meniscus and ligaments.

- osteoarthritis of the knee
- General information
- Osteoarthritis of the knee joint. causes
- The factors that promote the occurrence of the disease include
- Symptoms of osteoarthritis in the knee
- Osteoarthritis of the knee joint grade 1
- Stage 2 of osteoarthritis in the knee
- Main forms of trophic ulcers
- Treatment of trophic ulcers
osteoarthritis of the knee
Gonarthrosis is a chronic disease of the knee joint in which the cartilage tissue thins and breaks down, leading to severe bony overgrowth. As the disease progresses, the ability to move independently may be completely lost. Timely diagnosis and treatment of gonarthrosis offers the chance to stop the pathological process and relieve the affected person of their pain.
General information
Full function of the joint is possible only if several conditions are met:
- perfect smoothness of the meeting bone surfaces;
- the correct arrangement of the articular surfaces;
- the presence of synovial fluid, which serves as a lubricant;
- good condition of muscles, ligaments, joint capsule and other ancillary components;
- good blood supply.
If abnormalities occur, a pathological process is initiated, which can ultimately lead to complete destruction of the joint.
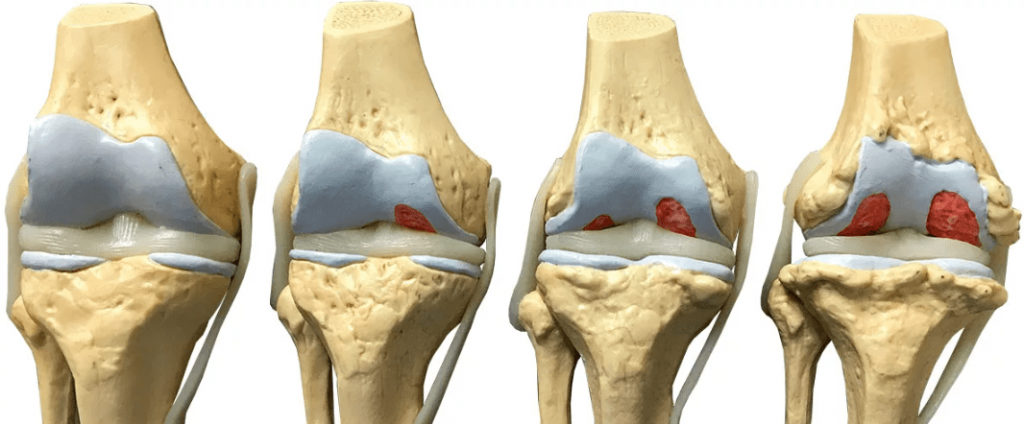
Gonarthrosis begins with the appearance of microcracks and thickening pockets in the cartilage tissue. This leads to a thinning of the cartilage layer and loss of suppleness. The result is increased friction between the bones during movement, which further damages the cartilage. The texture of the surface changes and individual areas begin to emphasize. As the disease progresses, bony outgrowths (osteophytes) form on the edges of the joints and gradually spread throughout the area, restricting movement and causing pain. At the same time, the composition of the synovial fluid changes and the amount of fluid decreases, which in turn increases friction.
Subsequent changes spread to other areas. The joint capsule becomes thinner and the ligaments lose their elasticity. The joint becomes unstable and the risk of a dislocation or subluxation increases. The muscle fibers contract in compensation. The knee and later the leg itself become deformed. At this point, the patient can no longer move properly due to pain.
Osteoarthritis of the knee joint. causes
Osteoarthritis of the knee joint is a chronic disease in which degenerative-dystrophic changes in the cartilage lead to complete destruction of the synovial membrane. Clinical symptoms include pain and limited joint mobility. Gonarthrosis is most often diagnosed in women over 45 years of age, competitive athletes, overweight people and people who perform strenuous, monotonous physical work. There is no single cause for the development of the disease. A number of unfavorable factors weaken the cartilage. The onset of the disease is a fatal combination of circumstances.
The factors that promote the occurrence of the disease include
- Knee injuries (broken bones, sprains, meniscus injuries), joint operations;
- Aging (cartilage loses elasticity with age and breaks easily)
- systemic autoimmune diseases (rheumatism, rheumatoid arthritis, lupus erythematosus, etc.)
- endocrine disorders (diabetes, hypothyroidism), menopause;
- genetic factors (vulnerable cartilage, too little synovial fluid)
- Excess weight (excessive stress on the joints);
- hypothermia and dehydration;
- Overloading of the knee joints due to heavy work and sport;
- Pathologies of the hip joints.
Low physical activity also contributes to the development of osteoarthritis. A sedentary lifestyle leads to reduced blood supply to the lower limbs, a slowdown in metabolic processes, atrophy of muscles, ligaments and tendons, and degeneration of cartilage structures.
Symptoms of osteoarthritis in the knee
The course of the disease is different and depends on the age and physical condition of the patient, the cause of the pathology and concomitant diseases. The most common complaints are knee pain when straining, swelling, burning of the affected joint, pain after prolonged immobility, dry throbbing and cracking when moving.
The diagnosis is made by an orthopedist after examination, questioning and additional tests.
Osteoarthritis of the knee joint grade 1
This disease often has no symptoms. Occasionally, patients experience mild discomfort, tension, and warmth in the knee joint.
The typical symptoms of grade 1 gonarthrosis include:
- Pain when moving or at rest after heavy exertion, with maximum flexion and extension;
- Burning, swelling and hypersensitivity of the knee after strain (signs of inflammation);
- X-rays show isolated osteophytes, narrowing of the joint stroma.
Important!!! The clinical signs characteristic of the first stage of the disease may be accompanied by significant cartilage destruction. Early diagnosis is important because conservative treatment is more effective, especially at the beginning of the disease.
Stage 2 of osteoarthritis in the knee
The pain becomes more intense and lasts longer, the functionality of the joint is restricted (the range of motion is reduced). The knee joint begins to deform ('flattening') due to uneven wear of the cartilage, and the lower extremity may bend. Typical symptoms of grade 2 knee osteoarthritis are:
- Constant pain on exertion, increasing in the morning and evening;
- Persistent pain in the joint even after a long period of rest;
- limited range of motion;
- Increased joint volume, periarticular soft tissue atrophy;
- Crunching when moving quickly, while squatting and sometimes while walking.
Main forms of trophic ulcers
Trophic ulcers (long-term non-healing wounds) are the most common form of diabetic foot syndrome. Seeing a doctor and treating diabetic foot ulcers should not be delayed as this can lead to atrophy of the limbs. Basically, diabetic ulcers are divided into neuropathic (in patients with normal blood flow in the legs) and neuro-ischemic (or ischemic), which are due to impaired blood circulation. A small percentage of patients with diabetes suffer from leg ulcers, usually caused by venous disease (venous insufficiency). What types of ulcers are more common? Contrary to popular belief, neuropathic ulcers are more common, accounting for approximately 55-75 % of all diabetic ulcers.
While severe circulatory disorders themselves can cause destruction of the skin (necrosis), diabetic neuropathy itself does not destroy the foot tissue. However, it creates the conditions for the formation of small (and not so small) lesions that go unnoticed by the patient. A diabetic can cut himself while cutting his nails and not feel pain, he cannot feel a foreign object in his shoes (a stone, a shard of glass, a forgotten sock, coins accidentally fallen into the shoe), he can sit on one lying on the floor Kick the paper clip and not feel it. Unfortunately, all of these examples are absolutely real when it comes to diabetes. The last type of injury (stepping on a button without the patient noticing) has happened to the author of these lines no more than three times in his practice. Of course, all these injuries lead to the development of trophic ulcers.
Treatment of trophic ulcers
- Appropriate topical treatment. Clean the wound and apply a new dressing daily or every 2 to 4 days (depending on the condition of the wound and the type of treatment).
a). Use of modern dressing materials (which, unlike gauze, do not stick to the wound). There are now a large number of such materials belonging to different classes: alginates, hydrophilic fibers, atraumatic meshes, polyurethane foam dressings, hydrogels, hydrocolloids, etc. The choice of dressing is made by a medical professional (doctor or specialized nurse) on the basis of a wound examination, of X-ray data etc. taken.
b). Wound irrigation with antimicrobials that do not harm growing tissue, e.g. B. Miramistin solution, chlorhexidine, etc. It is worth remembering that iodine, alcohol, verdict and manganese are contraindicated in diabetes, as they slow down the healing process.
c). Regular treatment of the wound by a doctor or nurse (removal of non-viable tissue, blisters around the wound (often caused by neuropathic ulceration)). Typically performed every 3-15 days. - Protecting the ulcer from stress when walking. As long as the patient continues to step on the wound, the wound will not heal, no matter how expensive medication or bandages are. Unfortunately, just a few steps a day can negate the results of ongoing treatment. Most neuropathic ulcers are painless, so the patient does not feel that he has stepped on the wound and damaged it. There are special relief devices to protect the wound. The 'low shoe' was first used in Russia, in which the forefoot is not put under any strain when walking. However, according to international and Russian recommendations, the most effective offloading method today is the offloading shoe (Contact Cast, see photo on the right) made of polymeric fixation materials (which are now used instead of plaster). This method allows the wound to heal more quickly, reduces pressure not only on the forefoot but also on the rear foot and allows the patient to work and lead an active life (unlike a 'low shoe').
- Competent use of antibiotics for wound infections (usually the choice of drug is based on the results of wound culture). Approximately 40-60 % outpatients with diabetic ulcers require antibiotics.
- Normalization of blood sugar levels (diabetes control). It is very important that a patient with diabetic foot syndrome receives continuous, high-quality diabetes treatment.
- Diabetic foot ulcers.
- Why amputate legs for diabetes?.
- Knee splint for knee arthrosis.
- X-ray of Charcot's foot.
- Photo: Diabetic heels.
- polo varus.
- equinovarus foot deformity.
- Metatarsal amputation.