The first sign of discomfort is pain. In the initial phase of the disease, they are felt only as a slight discomfort and appear only in the morning hours. Many people notice a nail-like feeling in their heel when walking, but this soon wears off.

- fasciitis
- PLANTAR FACIAL FOOT: CAUSES
- Why heel spurs develop
- Heel Spur Symptoms
- Heel Spur Treatment
- Plantar fasciitis: diagnosis of the disease
- Plantar fasciitis: treatment
- diagnosis
- Treatment of heel spurs
- Pharmacological treatment
- physical therapy
- UWT heel spur treatment
- Heel spurs: causes, symptoms
- The advantages of our treatment:
- diagnosis
- Endoscopic plantar fasciotomy and heel spur removal.
- Mini-invasive transection of the plantar fascia and removal of the heel spur under X-ray control.
- Causes of heel spurs in children
- classification
- Caused
- symptoms
- How long does the operation take?
- When can I drive?
fasciitis

Heel fasciitis is a condition that has long been unfairly overlooked. At first, the pain in the heel resembles a slight electric shock and usually does not bother at all.
The discomfort gradually increases and the pain is far from unbearable and permanent.
'Dr. OST' invites you to treat heel fasciitis early and non-surgically if you can avoid visiting a surgeon on the operating table. Schedule an appointment
PLANTAR FACIAL FOOT: CAUSES
The constant strain on the ligaments, which causes heel pain when it occurs, can have various causes:
- Flat feet and individual physiological characteristics are the most common causes of plantar fasciitis;
- overweight;
- uncomfortable tight or orthopedically incorrect shoes, high heels;
- systemic joint diseases that weaken connective tissue;
- a history of infection;
- Trauma;
- Poor blood circulation in the lower limbs, loss of vascular elasticity.
IMPORTANT!!! Inflammation of the foot fascia is rare in children: their connective tissue is soft, elastic, and the load is age-appropriate. For the treatment of fasciitis symptoms, you should usually only see your doctor after the age of 30:
Why heel spurs develop
The plantar fascia is heavily stressed when walking and running and is therefore prone to micro-injuries – tears. Normally, minor injuries heal on their own and do not require treatment, but the presence of certain predisposing factors means that fascial tears do not regenerate. This leads to inflammation and gradual degenerative changes in the tissues leading to the formation of marginal osteophytes of the heel bone – heel spurs. Plantar fasciitis is most common in middle-aged and older people, more common in women than men, and athletes who exercise intensely are also at risk.
- Prolonged physical stress on the foot: running, walking, standing work;
- obesity, which causes increased pressure on the feet;
- Spinal disorders that disturb the distribution of weight on the foot (scoliosis, etc.).
- Wearing totally flat-soled shoes without insoles, such as flip-flops, ballet flats, or shoes that are tight-fitting or badly worn on the outer edge and cannot provide cushioning and stability to the feet;
- Stretching of the fascia in athletes due to poor training technique or a drastic increase in training intensity;
- Excessive pronation (forward and inward rotation) of the feet - flat feet;
- high arch;
- Occlusive (blocking) lesions of the blood vessels in the feet, affecting normal blood flow;
- Inflammatory and degenerative-dystrophic joint diseases of the lower limbs - arthritis, arthrosis.
Heel Spur Symptoms
The main symptom podiatrists use to diagnose heel spurs is a stabbing and painful pain in the heel and arch area that occurs when the foot strikes after long periods of sitting or sleeping at night. The pain increases after physical exertion or climbing stairs and is noticeable visually and physically through swelling and dimples in the foot area.
Heel Spur Treatment
Heel spurs are treated using conservative methods, except in severe and advanced cases that require surgical treatment. The treatment is based on foot relief and massage. The following measures can help reduce excessive stress:
- limitation of walking on hard ground;
- Immediate rest when heel pain occurs;
- replacing tight and worn-out footwear with loose, well-cushioned footwear with a heel of no less than 2 and no more than 4 centimeters;
- reducing obesity;
- Eliminating inflammation and preventing complications requires special insoles that support the metatarsal arch and relieve pressure on the heel. You can buy ready-made insoles or order custom insoles and put them in the shoes you wear most of the time.
A massage of the sole and arch of the foot, the toes and the ankles is essential. At the same time, you should do specific stretching exercises for the plantar fascia and lower leg muscles every day to avoid strains and shortening of the fascia.
Physiotherapy and pharmacotherapy are used to eliminate inflammation, accelerate healing of fascial fibers, reduce pain and prevent further bone hypertrophy:
- magnetotherapy with low-frequency pulses;
- UHF therapy - irradiation of the foot with an ultra high frequency electric field;
- shock wave therapy to improve microcirculation in the tissues;
- X-ray therapy;
- laser therapy.
Nonsteroidal anti-inflammatory and analgesic drugs in the form of tablets, injections, ointments and gels are used to relieve pain and inflammation.
If conservative treatment is ineffective, surgical treatment is recommended, during which the bony outgrowth is removed and the irreversibly changed tissue is excised.
Plantar fasciitis: diagnosis of the disease
X-rays are generally considered to be the best way to diagnose this condition because ossification of the ligament can be seen on X-rays. However, in the vast majority of cases, a simple medical history, analysis of the main symptoms, visual examination, and palpation of the longitudinal ligament are sufficient to confirm the diagnosis of plantar fasciitis.
However, an X-ray examination helps to diagnose the presence of a spur from other possible causes of heel pain, such as: B. a bone fracture to distinguish. Also, the presence of a bone spur on an X-ray is not always indicative of plantar fasciitis, as there are also what are known as 'silent spurs' - where a spur is present but there is no pain. Conversely, there is pain but no spur. Therefore, the diagnosis should be made by a qualified medical specialist.
Plantar fasciitis: treatment



To get straight to the point: we recommend treating plantar fasciitis exclusively with shock wave therapy (UWT). All other physiotherapy devices are available in our clinic to treat this condition, but they are not as effective as UWT.
You can see the results of magnetic therapy, laser, ultrasound and other therapies on our website Treatment of heel spurs.
Shock wave therapy in our clinic is performed using a modern, new-generation Zimmer (Germany) device. The advantage of this device lies in the high success rate (more than 95 %) and the low sensation of pain during the treatment. A course of 5-6 treatments spaced 5-7 days apart is usually sufficient to fully regenerate the plantar ligament and eliminate the pain symptoms in the heel area.
There are virtually no contraindications to shock wave therapy for plantar fasciitis (unless the patient has a pacemaker, is pregnant, or has heel cancer). The treatments are slightly painful but are well tolerated by patients. The sensation of pain is noticeable only at the beginning of the treatment, and at the end of the session the device usually does not cause significant pain. A single session consists of 3,000 to 3,500 shocks and lasts around 10-15 minutes.
The percussion sound waves generated by the device easily penetrate through soft tissues and significantly improve metabolic processes in the affected area. This improvement in microcirculation ensures that shock wave therapy is highly effective. However, it is known that no physiotherapy session is complete without a positive reaction from our body: the sensations of pain stimulate our body to be more actively involved in the healing process.
diagnosis
The orthopedist diagnoses and treats heel spurs. X-rays are the primary means of detecting and assessing the severity of the disease. The bony prominences, their shape, location and size are clearly visible on the x-ray.
Other examination techniques are:
- General and biochemical blood tests to detect inflammation, determine uric acid levels (important for diagnosing gout) and some other indicators;
- urine test;
- Ultrasound examination of the foot to assess the condition of the soft tissues to detect a possible abscess;
- Duplex examination of blood vessels in the lower limbs (to detect possible circulatory disorders);
- MRI of the foot to determine the condition of all anatomical structures of the foot, including nerve fibers.
In the presence of concomitant diseases, appropriate laboratory and instrumental studies, as well as consultation with specialists are recommended.
Note that heel pain does not necessarily indicate the development of a heel spur. Similar symptoms can be caused by:
- Gout;
- Rheumatoid arthritis;
- osteoarthritis (inflammation of the bone);
- Bechterew's disease;
- tuberculosis of the bone;
- injuries, etc
Do not take self-medication or uncontrolled painkillers. Only the doctor can select the appropriate remedy.

Treatment of heel spurs
Treatment of a heel spur largely depends on its causes and symptoms and is prescribed on an individual basis. The doctor uses several methods:
- Medication;
- Physiotherapy – shock wave treatment; laser treatment;
- X-ray therapy;
- Massage;
- therapeutic exercises and gymnastics;
The patient has to adjust his lifestyle and diet and wear orthopedic shoes.
Pharmacological treatment
Medications used to treat heel spurs aim to reduce inflammation and pain. The most commonly used drugs include:
- nonsteroidal anti-inflammatory drugs (NSAIDs): indomethacin, diclofenac, ibuprofen-based drugs in the form of tablets, injections and topicals (creams, ointments, pain patches);
- longer-acting corticosteroids (Diprospan and its analogs) injected directly into the fascia to stop inflammation;
- Antibiotics for purulent inflammation or infectious nature of the disease.

Director, Chief Physician, Orthopaedist/Traumatologist
If there are concomitant diseases, drugs are prescribed to treat these diseases, e.g. B. Drugs to normalize blood flow, antipodigraviva, etc. Only the doctor decides on the appropriate medication, the dosage and the amount that needs to be taken.
physical therapy
The aim of physiotherapy is to improve blood circulation and tissue regeneration, as well as to increase the effect of medication. This is done through the use of:
- Electrophoresis: Injecting drugs into tissues using an electric current;
- Sonophoresis: treatment of tissues with ultrasonic waves that improve drug penetration;
- Ultrasound therapy: tissue heating and reduction of inflammatory reactions with the help of ultrasonic waves;
- mud and mineral baths.
UWT heel spur treatment
Heel spurs: causes, symptoms
The human foot is a perfect mechanism given to us by nature. The thin bones of the foot support the weight of the human body, as do the arched bridges, which are made of thin elements and support the weight of cars driving over them.
| On the plantar side, the sole of the foot is supported by the plantar aponeurosis, a strong band that connects the front and back of the foot. It prevents the foot from flattening under the weight of the body. The rear end of the plantar fascia is attached to the heel bone and the front ends are attached to the toes. |

| This is where a spur is most likely to form. The plantar fascia and the tissue surrounding it are exposed to heavy loads in an upright position. The ligament can usually cope with them, and rare micro-injuries heal spontaneously and without major pain. |
The advantages of our treatment:
- Treatment with the new generation Zimmer UHT device from Germany.
- Magnetotherapy treatment when paying for UHT treatment for free.
Heel Spur Pictures of different spurs HERE.
Below are various photos of heel spurs. This is what a heel spur looks like on an X-ray. As you can see in the photo, spurs can be large and small, but the pain does not depend on the size of the spur. There are spurs larger than 1 cm that do not hurt (heel spur photo 1), while very small spurs hurt a lot (heel spur photo 2). There are also cases where the spurs are not there at all, but pain occurs. This can be explained by the fact that the spur itself does not cause pain, but the pain is caused by the torn ligaments. When the Achilles heel is torn, the spur grows up the ligament (heel spur photo 3).
diagnosis
A simple analysis of the patient's symptoms, visual inspection, palpation of the sole of the foot and an X-ray are sufficient in most cases to correctly diagnose heel spurs. Photographs of the heel spur and palpation help distinguish plantar fasciitis from possible fractures. The absence of plantar fasciitis with pain requires an additional differential diagnosis in relation to the possible presence of systemic inflammatory diseases such as ankylosing spondylitis, rheumatoid arthritis, Reiter's syndrome and some others. Such diseases can also cause heel pain. The presence of a bony overgrowth is not always a reliable symptom, as 70% of adults have such an overgrowth but do not feel pain. The diagnosis should therefore be made by a specialist doctor who is able to correctly identify the cause of the heel pain and also rule out other diseases with similar symptoms.
Effect of geroprotectors - short peptides: - stabilization of metabolic processes in bones and connective tissue - acceleration of regeneration of musculoskeletal tissues in inflammation - reduction of pain when walking - increase in plasticity.
Composition:
– AC4 peptide complex – alanine – glutamic acid – aspartic acid.
Application: 1 capsule 2 times a day before meals. Course of 20 capsules.
Endoscopic plantar fasciotomy and heel spur removal.
Endoscopic fasciotomy. Conducted for the first time in 1991. Performed under regional anesthesia. With a tourniquet on the lower leg. A 5 mm incision is made on the medial surface of the heel, approximately 1 cm distal to the insertion of the aponeurosis. The endoscopic trocar and cannula are inserted superficially through the plantar fascia to the opposite edge of the heel region where an exit wound is made. The cannula is removed and the endoscopic camera is inserted into the medial portal. A retrograde cutting scalpel is inserted into the lateral one. And the dissection is done.
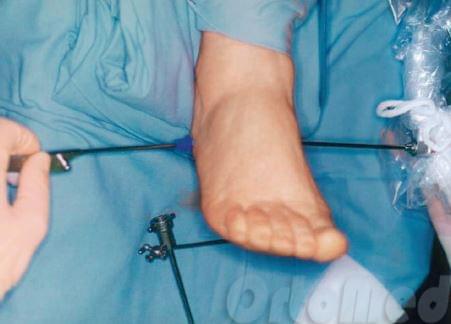
The surgeon can use the camera to observe the operating area. The plantar fascia is cut away from the heel spur (bone) so that its tension is released.
Mini-invasive transection of the plantar fascia and removal of the heel spur under X-ray control.

In contrast to the endoscopic technique, only an incision of 3 mm is made. A triangular-pointed scalpel is inserted to cut the plantar fascia where it meets the heel bone.

In a further operation, the exostosis (spur) of the heel bone itself is removed. A major advantage of this method is minimal trauma to the heel area (sole of the foot). This shortens the rehabilitation time to two days.

Many patients ask me: Can flat feet get worse after fascia removal?
No. Flat feet will not get worse because we only cut the medial (inflammatory) fascia during the operation, but the lateral fascia, which is connected to the heel bone of the same name, is preserved. With severe heel pain, gait disorders are much more dangerous. The patient reflexively begins to shift his body weight to the forefoot and the other foot. A limp or poor posture may occur. All of this can accelerate the progression of osteochondrosis or scoliosis!
The results of the heel spur operation and X-rays can be seen here.
Causes of heel spurs in children
In the normal state, the fascia is always taut and protects the bony and muscular structures of the foot from damage. With trauma, inflammation, or excessive deposition of calcium salts, the integrity of the fibers is compromised, and a bony outgrowth, known as an exostosis, gradually forms in this area.
The main causes of bony outgrowths in children of different ages forming spurs are:
- flat feet, in which the load on the ligaments and muscles of the foot is abnormally and unevenly distributed;
- Obesity, which increases the pressure on the lower limbs;
- wearing shoes that are too tight, narrow, heavy and uncomfortable, not adapted to the size of the foot;
- a sedentary lifestyle;
- Certain musculoskeletal disorders that shift axial loading of the skeleton, such as B. scoliosis;
- inherited predisposition;
- Excessive physical exertion in sports and other physical disciplines;
- metabolic disorders and diseases of the endocrine system;
- Injuries to the bones and joints of the lower limbs (dislocations, sprains, fractures, severe bruises);
- vascular diseases, in which the blood supply to the feet is impaired;
- Bone and cartilage diseases (osteoarthritis, arthritis, deformities of the limbs, etc.).
In some cases, the starting point for the development of the disease is an infectious inflammatory process in the surrounding tissues, as well as conditions in which there is a decrease in the density of bone structures.
Risk factors are children who are regularly subjected to static loads (running, long jumps, long walks), children who are subject to hormonal changes, and children who have problems with calcium and phosphorus absorption.
classification
According to the International Disease Registry ICD-10, plantar fasciitis refers to pathologies of the musculoskeletal system and connective tissue. The disease can be unilateral, with osteophytes forming on one foot, or bilateral, with osteophytes affecting the soles of both feet.
The course of development of plantar fasciitis can be divided into three stages:
- The first stage, entosopathy, is characterized by the first pathological changes in the longitudinal fascia under the influence of a traumatic factor;
- The second stage, fasciosis, is characterized by aseptic inflammation of the plantar fascia, that is, the process proceeds without the involvement of foreign pathogens;
- In the third stage, calcification, excessive accumulation of calcium salts occurs in the damaged fascia, leading to the formation of bony outgrowths.
The process of osteophyte formation is quite lengthy, lasting from 2 weeks to several months, depending on the type of injury and the cause of the pathology.
Caused
A heel spur develops when calcium deposits build up on the lower part of the heel bone, a process that usually takes many months. Plantar fasciitis is commonly caused by straining of the muscles and ligaments, stretching of the plantar fascia, and repeated tears in the membrane covering the heel bone. Heel spurs are particularly common in athletes who jump and run a lot.
Risk factors for developing heel spurs include:
- Impaired gait that puts undue stress on the heel bone, ligaments and nerves in the heel area.
- Running on hard ground
- Poorly fitting or worn shoes
- overweight, obesity
In most cases, plantar fasciitis develops without a specific cause.
However, there are some risk factors that increase the likelihood of developing plantar fasciitis and these are
- Older age. Tissue changes lead to a decrease in the elasticity of the plantar fascia and a reduction in fatty tissue in the heel area
- diabetes
- Activities that require standing on your feet for a long time
- Episodes of vigorous physical activity
- Flat feet or high arches.
- Thick calf muscles and limited foot dorsiflexion.
The function of the fascia is to absorb the loads that fall on the foot. At some point, however, the fascia can no longer take the load and a tear and fasciitis develop.
symptoms
Although many patients with plantar fasciitis have a heel spur, a spur does not always cause pain. Almost 10 percent of adults have a spur, but only 5 percent experience foot pain. Treatment of heel pain therefore does not require removal of the spur in most cases.
The most common symptoms of plantar fasciitis are:
- Pain in the lower part of the foot in the heel area
- Pain with the first steps after getting up in the morning or after a long period of rest, e.g. B. after a long drive. The pain subsides after walking for a few minutes
- Increased pain after (not during) exercise or physical activity.
A heel spur often causes no symptoms. However, a heel spur can occasionally cause pain or chronic pain—especially while walking or jogging if inflammation develops in the area where the spur originated. As a rule, the cause of the pain is not the heel spur itself, but a soft tissue injury originating from the spur.
Many patients describe Pain caused by heel spurs and plantar fasciitis causes pain that feels like a pin on the sole of your foot when you get up in the morning and later develops into a dull ache. There is also often a stabbing pain immediately after getting up after sitting for a long time.
How long does the operation take?
This is probably the most common question surgeons are asked. The total duration of the procedure is not just the time from the start of the incision to the placement of the last suture. Traveling by air, for example, is not just about the time you spend in the air, but also about check-in, pre-flight security, and boarding and disembarking.
The times given below are only guidelines.
Proximal relief of the medial head of the calf muscle:
When can I drive?
Proximal release of the medial head of the calf muscle:
Most patients can drive within 2 weeks after the procedure. See below for more information.
Our recommendations in this regard are listed above and here. Ultimately, the responsibility for this rests entirely with the patient. A good way to check if you can already drive or not is to place your right foot on the ground and press down hard to simulate a sudden slam on the brake pedal. If you feel anxious or in pain, it is better not to drive as it can be dangerous. In addition, driving a car puts your foot in a constrained position for a long time. This can worsen the postoperative swelling.
Read more:- Treatment of plantar fasciitis.
- Treatment of plantar fasciitis at home.
- Treatment of plantar fasciitis ointment.
- Longitudinal soleus muscle.
- Structure of the human heel.
- Tear of the foot fascia.
- Treatment of plantar fasciitis on the sole of the foot.
- Orthopedic shoes for women with heel spurs.