Figure 4: X-ray of an anatomical preparation of the pubic bones at the pubic symphysis in a 13-year-old boy.
1 – The indentation ('filing') of the pubic bones is clearly visible.
- Fracture of the growth zone
- Location of growth zones
- Did you know?
- Symptoms of growth zone fractures
- ICD-10
- Causes of epiphysiolysis
- symptoms
- Classification of plateau fractures
- Indications and contraindications for diagnosis
- Research methods and results
- Endocrinologically independent variants of growth retardation
- What the investigation shows
- Indications and contraindications
- Causes of stunting
- Symptoms of growth arrest in children
- Age-related features of the pelvic bones
- Conclusions
- About the skeleton
- About muscles
Fracture of the growth zone
Epiphysiolysis occurs at the ends of bones. These are the areas (called growth zones) where children can grow. Growth zone fractures only occur in children and adolescents.
A growth zone fracture can occur when the bone is subjected to repeated stress or when a child experiences trauma.
A growth zone fracture causes pain and swelling in that area, and children have difficulty moving the damaged limb.
Doctors suspect this fracture based on symptoms and usually diagnose it with an X-ray.
Some growth zone fractures are treated with a cast or splint, but for more severe fractures, fragments of the damaged bone are replaced (repaired) with or without surgery and a cast is applied.
Growth zones are areas of cartilage in long bones (such as arm and leg bones). They allow the bones to grow longer until the child has reached its full size. Once growth has stopped, the growth zones are replaced with bone. Growth arrest varies by bone, but by the age of 20 all growth zones have been replaced by bone.
Location of growth zones
Growth zones (indicated by pink lines) are areas of cartilage near the ends of long bones, such as arm and leg bones. They allow the bones to grow longer until the child reaches its full size.
Since cartilage tissue is more sensitive than bone tissue, the growth zones are particularly prone to breakage. If a growth zone breaks, the bone may stop growing or grow unevenly. If a joint is affected, permanent damage can occur, leading to arthritis.
Did you know?
In children, some bones have areas of cartilage that are more fragile than the bone and only harden after growth is complete.
A fracture can occur right along the growth zone, where the bone separates from the cartilage. However, the fracture can also run above or below the growth zone, sometimes across the entire width of the bone and reaching the joint. The most serious type of fracture is a compression fracture (in which the growth zone is crushed).
Symptoms of growth zone fractures
The area around the growth zone is painful, especially when palpated. In addition, there is swelling and a local increase in temperature in the injured area. Children may have difficulty moving, applying force or pressure to the injured limb.
If children have symptoms suggestive of a growth zone fracture, they should be taken to a doctor or emergency room.
Doctors suspect a growth zone fracture based on the symptoms.
Most growth zone fractures can be detected by radiographs. However, some types of growth zone fractures cannot be detected. The child is then classified as fractured and appropriate treatment (with a cast or splint) is prescribed. The child will be re-examined a few days later. If the area is still painful when palpated, you probably have a growth zone fracture.
ICD-10

Epiphysiolysis (Salter-Harris fracture) is a traumatic bone injury that occurs only in children during skeletal growth. It was first described in 1963. It accounts for about 15 % of all fractures in children. Almost half of cases involve the wrist and elbow. Boys are affected twice as often as girls. Epiphysiolysis heals well, but damage to the epiphyseal plate can lead to further impairment of bone growth.
Causes of epiphysiolysis
Bone damage results from trauma in the home and on the street. The mechanism is similar to sprains and strains in adults. Epiphysiolysis is caused by suddenly twisting the leg, hyperextending the arm, dropping the elbow or shoulder, jerking the arm, or twisting the limb about its own axis. Sometimes it is also caused by a rapid, strong muscle contraction. Predisposing factors are:
- Male gender. The higher incidence of epiphysiolysis in boys is due to two circumstances: a higher level of motor activity and later completion of the rostral zones compared to girls.
- periods of rapid growth. Uneven growth of bones and soft tissues and the need to adapt to rapidly changing body proportions lead to lack of coordination of movements and increase the likelihood of injury.
- asthenic constitution. Due to insufficient muscle mass, the growth plates of asthenic children are more stressed than those of normosthenic children.
- Injury-prone sports. Soccer, volleyball, handball, rhythmic gymnastics, and some track and field cards increase the likelihood of limb injuries.
Metabolic disorders, malnutrition and a weakened immune system play a role. The relationship between the risk of developing epiphysiopathy and the child's age has not been clearly established. Some experts point out that statistically most injuries occur between the ages of 10 and 18. Other researchers point out that injuries in young children are more likely to go undetected due to an unclear clinical picture and lack of changes on x-rays.
symptoms
Symptoms appear immediately after acute trauma or overexertion. They are usually located around the joint near the epiphyseal plate:
- Pain that worsens when you try to move or feel the injured area
- Restriction or total inability to move the joint.
- When the leg is injured, it cannot fully support the weight of the body.
- When the arm is injured, it is difficult to keep balance.
- swelling
- bleeding under the skin
- In some cases, deformation occurs.
Important: An exact diagnosis cannot be made on site. A fracture in the area of bone growth often closely resembles a bruise, dislocation, strain or torn ligament. To understand the nature of the injury and receive appropriate treatment, you should take your child to a trauma center. Even if the injury doesn't seem serious, it's better to calm the child down.
Classification of plateau fractures
There are three main types of growth zone injuries:
- epiphysiolysis – Rupture of the epiphyseal plate. In this case, only the integrity of the cartilage is affected, and the epiphysis is separated from the metaphysis.
- osteoepiphysiolysis or metaepiphysiolysis – is a condition in which part of the metaphysis is detached from the bone along with the epiphysis. This fragment, as a rule, has a triangular shape.
- apophysiolysis – Detachment of part of the apophysis. The most common example is an injury to the external epicondyle of the humerus, which is where the muscles that primarily lengthen the arm attach.
In 1963, two Canadian orthopedic surgeons, Robert B. Salter and W. Robert Harris, developed a classification of traumatic injuries to the epiphyseal growth zone. It was named after the authors, the Salter-Harris classification (often epiphysiolysis and osteoepiphysiolysis are also referred to as Salter-Harris fractures). The authors identified five types of injuries and labeled them with Roman numerals IV. The following applies: the higher the number, the greater the risk of disturbed bone growth:
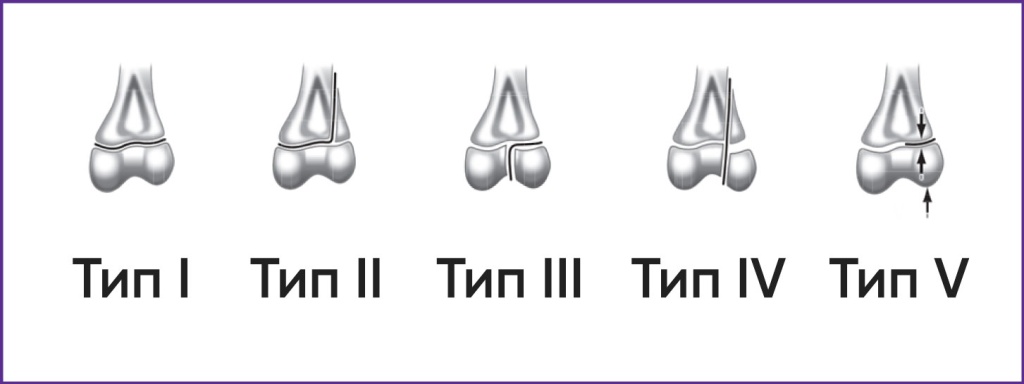
Type I – A fracture that runs along the growth plate. The cap is separated from the metaphysis. – Occurs in 6 % of cases.
Type II – A fracture that runs along the rostral zone and extends into the metaphysis without affecting the epiphysis. Eventually part of the metaphysis detaches along with the epiphysis - as a triangular fragment as shown. – This happens about 75 % of the time.
Type III – The fracture runs along the rostral and extends to the epiphysis but does not involve the metaphysis. In this case, with a complete fracture, the epiphysis splits into two fragments. The articular cartilage is damaged. – Occurs in 8 % of cases.
Type IV – The fracture goes through the metaphysis, the rostral zone and the epiphysis and often damages the articular cartilage. Type III and IV fractures often impair bone growth and joint function and therefore require immediate medical attention. – They occur in up to 10 percent of cases.
Indications and contraindications for diagnosis
The main indications for determining the bone age of a child are various types of disorders in the child's physical development, growth retardation, diseases of the pituitary, thyroid and hypothalamus. Specialists such as endocrinologists, pediatricians and orthopedists deal with this problem by sending the patient for a radiological examination to a medical facility where an X-ray machine is available.

For example, a radiological examination of the hand may reveal the presence of abnormalities such as pituitary dwarfism or dwarfism caused by growth hormone deficiency, precocious puberty, or bone development disorders caused by genetic abnormalities, e.g. B. the presence of a genetic disorder:
Among the main contraindications for determining the bone age of a child, doctors note an age below 14 years, when the procedure can only be carried out on the recommendation of a doctor. In addition, the examination should not be repeated more often than every six months because of the strong X-ray radiation, which is harmful to the immature body. However, it should be noted that patients do not need any special preparation for the examination.
Research methods and results
X-rays of the wrist and hand are most commonly used to correctly determine a patient's bone age. During the examination, the specialist analyzes and compares the image that he sees on the X-ray with the data that are considered normal for this age group.
With diagnosed and possible diseases of the pituitary gland, physical development is significantly delayed compared to the actual age parameters of the child. This delay can sometimes be up to two years. In contrast, when diagnosed with skeletal dysplasia or genetic stunting, bone growth delay is usually absent or minimal.
When diagnosing the skeleton, it is also worth remembering that there are not only age-specific features, but also gender-specific ones. For example, the female skeleton develops significantly faster than the male, sometimes by 1-2 years. These gender-specific ossification characteristics become noticeable from the first year of life of a child.
The X-ray image can be used to determine the stage of puberty the patient is in at the time of the examination. The appearance of the sesamoid of the metacarpal can be judged by the increased function of the sex glands in the body; when the metacarpal bones ossify, girls start their menstrual cycle and boys start having regular sex.
A growth spurt occurs when the body length increases very rapidly in a short period of time. When sexual maturity occurs prematurely, one can speak of an evolving bone maturation process, and when growth hormone synthesis is reduced or there is pituitary dysfunction, one can speak of a slowdown in the process.
X-ray examination of the bones of the skull reveals an abnormal condition of the Turk's saddle, which suggests endocrine disorders. Pituitary nanism is characterized by a reduction in the size of the saddle, with pituitary tumors thinning its walls, widening the entrance and causing areas of calcification. Intracranial craniopharyngioma tumor originating from pituitary cells - the sutures spread and create indentations on the inside of the child's skull.
Endocrinologically independent variants of growth retardation
In most cases, patients with growth retardation show no signs of endocrine dysfunction, ie growth retardation in most children is caused by non-endocrine factors.
Severe somatic diseases leading to a persistent state of hypoxia (congenital heart defects - consult a pediatric cardiologist, anemia, pulmonary diseases), malabsorption (celiac disease, cystic fibrosis), severe metabolic disorders (chronic liver and kidney diseases) and bone pathologies (chondrodystrophy, hargoilism and other congenital syndromes ) often go with a heavy stunting. There is no evidence of primary endocrine gland involvement in these variants of nanism, and bone age usually corresponds to chronological age. The symptoms of the underlying disease are in the foreground.
Constitutional delay in children – is the most common problem faced by paediatricians.
Constitutional stunting (late puberty syndrome) is characterized by inherited growth and development disorders and occurs in about 2 % of children, more often in boys.
Typically, the parents and/or close relatives of these children share the same developmental characteristics. For example, length and weight at birth do not differ from those of healthy children. The lowest growth rate occurs in the first years of life, so the most pronounced growth retardation is observed in children aged 3-4 years (Markushka Children's Orthopedic Clinic). From the age of 4-5 years, the growth rate returns (5-6 cm per year), but with an initially low growth rate, children remain stunted until school age. Skeletal age is slightly delayed compared to chronological age (by 2 years on average). This could explain the late onset of puberty: pubertal development and thus pubertal growth are delayed by 2 to 4 years in these children. As a result, adolescents with late puberty syndrome temporarily lag behind their peers in their physical development. The late onset of puberty is considered a favorable factor in this case, since it enables patients with such constitutional developmental traits to eventually achieve normal growth.
What the investigation shows

X-ray examination of the hand to determine bone age shows delayed or accelerated physical and sexual maturation. This, in turn, can be the result of pituitary dysfunction (pituitary dwarfism), thyroid disease, congenital adrenal hyperplasia, or a number of genetic disorders.
Indications and contraindications
Since X-rays mean exposure to ionizing radiation, the examination of bone age in children is carried out only in the case of strict indications:
- stunted or excessively rapid growth;
- delayed physical development;
- Suspicion of genetic disorders: Turner-Schereszewski syndrome, congenital adrenal hyperplasia, etc.;
- delayed or accelerated sexual maturation;
- Recognized endocrine pathology: diseases of the pituitary, hypothalamus, thyroid, adrenal glands.
There are no absolute contraindications to participating in the study. The relative limitation is age under 14 years. In this case, the diagnosis is carried out only on the doctor's prescription and in the presence of clear indications.
Causes of stunting
There are a number of reasons for disability, the most important of which are listed in the table¹:
| abnormality | ICD-10 inhibition | Ground |
| Family stunting | Stunting Not Elsewhere Classified 34.3 | Parental short stature (150-165 cm) |
| Constitutional stunting | Short stature, not elsewhere classified 34.3 | Delayed growth |
| Psychosocial Atrophy | Short stature, not elsewhere classified 34.3 | Psychological atmosphere in the child's environment, dysfunctional family |
| Somatogenic growth retardation | N25.0, K90.0, E24.2 and others | Developed after heart, kidney and respiratory diseases |
| Hereditary Syndrome | Q96, Q87.1 | Various syndromes: Sherejevsky-Turner, Noonan, Russell-Silver |
| chondroplasia | E03.0 - E03.9 | thyroid abnormalities |
| Pituitary insufficiency, including somatotropic insufficiency | E23.0, E23.1, E89.3 | Deficiency of growth hormone STH or several pituitary hormones. Can be caused by tumor and damage to the pituitary gland |
Symptoms of growth arrest in children
The main symptom of growth arrest is one: the lack of growth parameters at different stages of life ² . Depending on the characteristics, there are some nuances:
- Constitutional stunting (Constitutional stunting) goes hand in hand with normal hormone production. Length and weight at birth are normal. Severe stunting occurs at 3-4 years of age, after which growth returns to normal. Bone age is delayed from pass age by 1-2 years. In children, puberty is delayed by 2-4 years, but the growth zones also close later. Therefore, over time, growth normalizes and the disease does not require treatment;
- familial stunting. Growth and weight parameters are normal at birth. At the age of 3-4 years, the growth rate slows down, the child grows 2-4 cm per year. Bone growth is not chronologically delayed and hormone production is normal. Puberty comes at the right time;
- Hormonal insufficiency is associated with the most severe and pronounced symptoms. With STH deficiency, the growth rate and bone age deviate significantly from the norm. The delay is already noticeable at the age of 2 years. The facial features change: they become small, 'doll-like', they become overweight. Boys are characterized by a micropenis;
- tumors …Tumors that cause stunting can cause neurological symptoms and visual disturbances.
To determine the exact cause, a qualified diagnosis is required.
Age-related features of the pelvic bones

Age-related features of the pelvic bones / Fedorov II // Forensic medicine. – M., 1963 – №4. – C. 18-25
Bibliographic Description:
Features of the age of the pelvic bones / Fedorov II // Forensic examinations. – М., 1963. – №4. – C. 18-25
Features of the pelvic bones can be used in forensic practice to determine a person's age.
To study the ossification processes of the pelvis, the radiological method was mainly used, which in some cases was supplemented by anatomical and histological studies.
A total of 630 healthy subjects (from birth to 25 years of age), 48 anatomical specimens of pelvic bones, 40 anatomical specimens of growth zones and 51 histological sections of anatomical specimens of growth zones were examined.
The Hip Bone is already clearly differentiated into shaft and wings radiologically at birth. Its superior edge is arched and gently contoured, its anterior edge is nearly straight, its posterior edge near the posterior superior ostium almost meets the lateral edge of the sacrum. The posterior ostium and superior ischial notch are well defined. The back edge is curved down and the sides are straight and smooth (Fig. 1).
At the end of the first year of life, an irregularity can be seen at the upper edge of the bone. In children aged 2 to 3 years this irregularity takes the form of a distinct jagged formation or 'saw tooth' (see Fig. 5, 1). It is most pronounced between the ages of 13 and 16. By the age of 19-25 years, the irregularity disappears with the onset of synostosis of the back with the ilium.
Figure 1: X-ray of a newborn's pelvis.
Microscopic examination revealed the abnormalities to be an area of preliminary cartilage calcification with irregular resorption and replacement by bone tissue.
The inferior anterior ossicularis develops from an accessory ossification nucleus that is evident on radiographs from 12-14 years of age. Synostosis of the inferior ossicularis with the ilium occurs in women at the age of 14-16 years and in men at the age of 15-18 years.
Conclusions
- The apophysis of the lower branch of the long bone with an enlarged nucleus of ossification occurs at the age of 19-22 years, regardless of sex. Synostosis of the apophysis with the lower branch occurs in men at the age of 22-23 years and in women at the age of 22-25 years.
- Accessory ossification nuclei of the iliac crest and ischial apophysis appear in girls at 13-15 years of age and in boys at 15-18 years of age. Our observations suggest that synostosis of these apophyses occurs at 19-22 years of age in males and 19-25 years in females. However, this question can only be finally answered after examining a much larger number of observations of 22-25 year olds.
- Synostosis of the lower branches of the ischium and pubis occurs in girls at the age of 6-12 years and in boys at the age of 8-15 years; incomplete synostosis occurs from the age of 3 years, regardless of gender.
- An additional nucleus of ossification of the anterior inferior ilia manifests itself by the age of 12-14 years, regardless of sex. Hip bone synostosis occurs in girls at the age of 14-16 years and in boys at the age of 15-18 years.
- Synostosis of the bones that form the acetabulum occurs in girls at 13-15 years of age and in boys at 15-17 years of age.
Ossification sequence of human laryngeal cartilages / Poletaeva MP, Gelguldiev GG // Selected issues of forensic examination. – Khabarovsk, 2021 – №20 – C. 117-120.
Age-related changes in the articular cavity of the scapula / Chertovskikh AA, Tuchik ES // Forensic expertise. – M., 2019 – №2. – C. 31-33.
About the skeleton
Infant bones are formed from soft pieces of cartilage (growth plates) and grow (proportionally) with the child's body. Towards the end of growth, the cartilage hardens but stops increasing in length (so we're not getting taller). Children's bones can be damaged by even minor stresses. However, with proper care, a child's skeleton is able to heal injuries quickly (because it's mostly made up of cartilage). An exception is damage to the growth plates, which can lead to abnormal bone growth and possible disability.
Nadezhda Kuzmenko, Pediatric Orthopedist at ON Clinics Kharkiv Medical Center said:
'Healthy children are not protected from developing musculoskeletal disorders in childhood or adulthood. In most cases, this is due to children's anatomy and trauma. Many children are unaware of what they are doing when they are playing or moving, are inattentive or do not follow adult directions, resulting in limited mobility.
In the maternity ward, a pediatric orthopedist examines the newborn's skeleton. This assessment is based on the position of the baby's head and the flexion of the upper and lower limbs. If abnormalities are detected, they are corrected with massage, physiotherapy and therapeutic exercises. I would like to point out that severe skeletal abnormalities do not always cause pain in the child. Sometimes deformities are painless, but as the child grows, they can affect their ability to walk.
It is worth paying attention to how children move, squat, bend or straighten their arms and legs. Regular orthopedic check-ups (once or twice a year from the first year of life) help to detect hidden signs of diseases of the musculoskeletal system that the parents may not notice.
Treatment for bone disease in children depends on the diagnosis. Some children can recover from certain disorders, while others require ongoing rehabilitation or surgery.
About muscles
Our muscles are controlled by the nervous system. When it's not working properly, muscle contractions and diastoles occur. This affects the musculoskeletal system, leading to spinal deformities and other bone and joint disorders. Notice how the child moves, turns, and moves their limbs. If nerve irritation or pain sensations occur, you should consult a doctor.
It is equally important to pay attention to the development of the child's feet: they support the weight of the body and allow them to walk, run and jump. Uncomfortable shoes, obesity and lack of mobility can deform the feet. Parents should monitor their child's walking (toes, heels, or flat feet, clubfoot, foot lift or drop) and seek orthopedic assistance at the first obvious sign of difficulty walking.
In the first years of life, children's feet are very flexible and therefore prone to deformities. Allow your child to walk more barefoot on a safe, level surface without shoes restricting movement. This sets the pace for natural walking and forms the correct foot load. Almost all newborns have flat feet, which gradually deform when walking. If this is not the case, you should see an orthopedist who will select orthotics (e.g. insoles and orthopedic mats).
Evgeniy Popov, pediatric orthopedist at ON Clinic Nikolaev Medical Center, emphasizes:
Read more:'It is wrong to think that flat feet only occur in children under the age of three or six. Flat feet can be congenital or acquired (particularly due to endocrine or nervous system dysfunction) and can occur at any age.
- At what age do girls' legs grow?.
- The intercondylar syndesmosis is the.
- foot bone in Latin.
- The so-called lateral foot bone.
- Lower leg and foot bones and their connections.
- foot bone in Latin.
- What should you do if your child has tics?.
- Girls feet 13 years old.