Gymnastic exercises for flatfoot deformity strengthen the muscle and cartilage groups of the lower extremities and foot, form the supporting tone for the longitudinal arch and correct the overall deformity. The following therapy methodology will organize the following tasks:

- Varus deformity of the foot in children
- Classification: types and grades of varus foot deformity in children
- Unusual clubfoot
- What footwear should be worn with a varus foot?
- Crooked Feet
- What type of shoes should I wear if I have valgus?
- Advanced treatment of congenital foot deformities in infants
- Before and after treatment
- Treatment of forefoot shortening (varus)
- WITHOUT plaster cast
- Information for Parents
- Symptoms of a short foot
- What is a metatarsal?
- What is a metatarsal adduction?
- Treatment
- Advice and recommendations from an orthopedist at the Perseus Orthopedic Center. Tel. 8 (495) 469-99-05
- Clubfoot in children
- Treatment of congenital flatfoot
- promotions
- Therapeutic rehabilitation for children in their first year of life
- flat feet and fallen arches
- General information.
- Metatarsus adductus ('sickle foot').
- clubfoot
- flat feet
Varus deformity of the foot in children
A varus deformity of the foot is a pathology in which the heel is set up in an 'O' shape. As a result, when the child walks, it rests on the outer, lateral surface of the foot and the toes point inwards. If this pathology is not corrected, it leads to skeletal anomalies, deformities of the lower limbs, knees and hips, and joint problems. Experienced pediatric orthopedists at the SM Clinic in Moscow diagnose and treat varus deformities of the feet in children and generally stabilize the lower limbs.
The musculoskeletal system of a young child differs significantly from that of an adult. The bones, joints, and ligaments are not fully developed, and the tissues are extremely flexible and soft. Therefore, excessive and abnormal loads, if repeated over and over, can lead to the development of a deformity.
As a rule, parents discover a varus foot deformity when the child begins to walk and only seek orthopedic treatment much later. However, over the years the foot position becomes more and more unstable and the unequal distribution of the load on the legs leads to progressive postural disorders and deformities of the lower limbs.

Classification: types and grades of varus foot deformity in children
Based on the cause of orthopedic pathology, several types of varus foot deformities in children can be distinguished:
- Static: caused by incorrect posture;
- Structural: caused by a defect in the development of the talus;
- Rickets: caused by vitamin D deficiency and rickets;
- Paralytic: occurs as a complication of neurological diseases (encephalitis, poliomyelitis);
- Spastic: caused by muscle spasms (eg, cerebral palsy);
- Compensatory: caused by congenital deformities of the ankle, Achilles tendon or tibia;
- Traumatic: caused by injuries to the foot, ankle, and lower limbs;
- Hypercorrection: associated with abnormal orthopedic correction of other conditions.
Unusual clubfoot

Varus foot position – The knee joints are laterally flexed at the O-joint and not connected in a straight line, resulting in the child having to walk on the external arch of the foot (see tables for pediatric foot types).
Varus foot plantar flexion is more common in infants and in children with diabetes, cerebral palsy, various brain tumors, polymyositis and other serious diseases. (See table on frequency of varus and valgus feet).
If the foot is abnormally varus, it is corrected with orthotics or elastic bandages prescribed by an orthopedist.
What footwear should be worn with a varus foot?
Special varus footwear is used for the treatment.
Varus shoes have a high heel and no backbone. This type of shoe insert is custom-made for a comprehensive correction. Available in Standard 'antivarus' insoleswhich can be purchased in orthopedic shops. These shoes keep the foot in the correct vertical position, prevent buckling and allow the child to rest on the whole foot and not on the outer arch of the foot.
Wearing anti-tilt shoes is obligatory in kindergarten. For the cure MEMO and ORTEK shoes can be considered anti-viscosity shoes. To avoid feet with ankle joint or slight deviation, good prevention shoes with ankle support and ankle bandage should be worn from the first steps; supinating shoes should not be used.
With the foot in question, it is common that This means the foot is pronated. This means that the foot has a wavy curve (see table of pediatric foot variations).
Crooked Feet

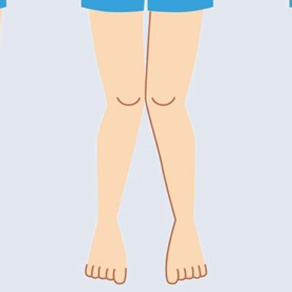
Cobotic Feet – The knees are close together in an X-shape and the feet are spread apart so that the child has to walk on the inner arch of the foot. (See diagram of children's foot position).
The following foot conditions are associated with a diagnosis of valgus:
Longitudinal flatfoot. – This is a flat foot that runs the full length of the foot. It is the most common flat foot in preschool and elementary school children. Statistically, every second child has abnormal foot development. (See table for appearances of varus and valgus feet).
With longitudinal flatfoot, The arch of the foot is flattened. It touches the ground with almost the entire surface of the sole, causing the foot to elongate.

About 30 % of adults have longitudinal flatfoot, which is due to muscle weakness in lower leg and foot caused by increased body weight, standing work, decreased muscle strength due to physiological aging, lack of muscle training in sedentary jobs, injury, etc.
What type of shoes should I wear if I have valgus?
The following is suitable for a valgus foot, a longitudinal valgus foot of the first degree and a longitudinal valgus foot of the first degree
- supinating shoes with good arch support MINIMEN, ORTOPEDIA, TASHI ORTO, ORSETTO, ORTEK prophylactic supinating shoes, etc.
- orthopedic standard insoles
If flatfoot is diagnosed, grade 11 longitudinal flatfoot is appropriate:
Advanced treatment of congenital foot deformities in infants



UNFO is a revolutionary solution specifically designed to correct all degrees of congenital clubfoot, also known as varus, clubfoot and forefoot adduction in infants and young children.
The UNFO orthopedic bandage minimizes the difficulties and stresses associated with frequent plaster casts, ineffective stretching exercises and massages and the subsequent insufficient or excessive clubfoot correction.

Before and after treatment


Treatment of forefoot shortening (varus)
WITHOUT plaster cast
Parents and children around the world can now experience the benefits of UNFO Therapy, which offers an effective and stress-free treatment that relieves family stress and significantly improves quality of life.
Information for Parents

Clubfoot (varus foot, equinovarus, clubfoot, adduction forefoot) is a foot curvature that is common in newborns. Left untreated, this type of abnormality can lead to permanent physical disability.

The UNFO orthosis meets the highest international medical standards. The effectiveness of the method has been confirmed by scientific studies. Thousands of parents who have chosen UNFO sandals have successfully treated forefoot shortening.

Symptoms of a short foot
Your doctor will notice the following symptoms:
- adduction of the big toe. The straps pull him inward.
- Widening of the first toe box (as a result of the first point).
- Adduction (inward rotation) and supination (outward rotation) of the forefoot.
- Inward deviation of the metatarsal bones.
- Flexion of the medial (inner) edge of the foot towards the hindfoot.
- preservation of the longitudinal arch. No signs of flat feet. It occurs as a result of the lowering of the foot with a weakening of the longitudinal ligament.
- A valgus deviation occurs in the heel position. outward turn.
- Displacement or subluxation of the spleen bone.
The patient presents with the following complaints:
- Discomfort and pain when walking.
- Quick fatigue.
- Frequent occurrence of blisters.
- Inflammation in the ankles (redness, swelling, temperature increase, pain).
- changes in gait.
What is a metatarsal?
There are two forms of this disease:
- Innate. It is diagnosed soon after birth. The sooner treatment is started, the less likely the foot deformity will recur.
- Acquired. Often found in infants 8-10 months of age during a visit to the podiatrist. If the curve is corrected before the age of 1 year, the condition will never recur. The deformity arises due to insufficiently rapid development of the musculoskeletal system of the lower limbs.
When walking, the foot is not properly fixed, the whole body weight presses on it unevenly, the ability to swing is lost, and the cushioning function of the limbs decreases.
The muscles of the leg are particularly affected: muscle and ligament disorders appear, the load on the ankle joint increases.
All this causes the gait to change and become uncomfortable. A child with one foot raised causes problems. He falls more often than others, injures his ankle, runs and jumps poorly because his toes are turned in. Later, other anomalies appear, twisting not only the ankles but also the ankle.
What is a metatarsal adduction?

Congenital adduction of the foot (about 50 % of cases are bilateral). It occurs in some cases in infants. Hip dysplasia is present in approximately 10 % cases of this deformity. In this case, the front part of the foot points inwards. However, the medial and posterior parts of the foot remain in their normal position.
The medial edge of the foot is curved and the lateral edge is convex. The distance between the first and the second toe is increased, the inward rotation of the big toe is particularly pronounced. Both flexion and extension in the ankle are unaffected. A forefoot stiffening is possible. With this type of deformity, the child turns the foot in with the toes in and wears the shoes improperly.
If the above symptoms are detected, the child should consult a specialist doctor. Doctors recommend wearing orthopedic shoes to correct the deformity.
Treatment
Treatment for flat feet is performed by a doctor, podiatrist, or therapeutic exercise specialist. The treatment can include therapeutic exercises, special massages and carefully selected orthopedic shoes and boots. You can buy all this in our children's shoe store. The following activities are no less effective (depending on the age of the child):

- Wheelchair use: strengthens muscles;
- wall bars, horizontal bar with ropes and ladders;
- Cycling and walking barefoot on a ramp or beam.
In most cases, forefoot adduction is corrected with massage. It is advisable to simultaneously treat the lower limbs with a full body toning massage (except hands). If for some reason these treatments are not possible, it is advisable to limit the massage to the buttocks, feet and lower back.
If forefoot adduction in children is treated from the start, experts recommend a more conservative therapy. Usually the end result is positive. In complicated cases, specialists resort to surgical intervention. In such cases, they perform an osteotomy of the metatarsal bones at their base and correct the misalignment (Peabody surgery).
Gymnastics and massage in the first year of the child's life, appropriate physical activity and the right choice of footwear contribute to the formation of healthy feet. The prognosis is very good with timely treatment.

The indications for treatment in this case depend on the age of the child, as well as the characteristics and extent of the deformity. In some cases, treatment with a splint is recommended. This method is indicated for children under one and a half years old with an angle of deviation of several degrees.
Advice and recommendations from an orthopedist at the Perseus Orthopedic Center. Tel. 8 (495) 469-99-05
- Orthopedic practice
- Advice from a podiatrist
- online consultation
- Visit a specialist
- manufacture of shoes
- orthoses, traction insoles
- Orthotics and corsets for the lower limbs
- Stabilization in cerebral palsy
- Insoles for clubfoot.
- With reinforced arch support
- For dynamic splints
- For children
- teenagers
- Adult
- Home
- Supportive footwear for prostheses and aids
- For diabetics
- Tactical shoes, military shoes, outdoor and hiking shoes
- Custom insoles
Clubfoot treatment with orthopedic footwear. Clubfoot Treatment. perseus 12

2 Complicated orthopedic footwear made from impression and contouring
Shoes with inserted tunic, stiff buttocks and lengthened ankle boots, lengthened heels: P-45, P-48, P-14


Equinovarus Ankle Leather Corset
The splint is designed to accommodate hard-soled orthopedic shoes.

Clubfoot in children

Clubfoot is a deformity of the distal part of the lower limbs.
It includes equinus, varus, pes cavus, and anterior adduction. Clubfoot is more common in boys than girls.
Clubfoot in childhood is congenital. In newborns, this defect occurs with a frequency of one in a thousand. Acquired clubfoot occurs as a result of nerve disease or as a result of trauma.
Massage and incremental affusions are required for effective treatment of clubfoot.
The best treatment results are achieved when treatment is started in infancy. Success depends on age and the severity of the deformity. Orthopedic shoes are prescribed for minor deformities when a cast is not indicated, or after cast removal to prevent recurrence of the deformity. During the child's active growth, the foot deformity may recur. If treatment is started on time, the prognosis is favorable. Clubfoot is a developmental disorder that can be identified soon after the baby is born. In the early stages, clubfoot in children can be treated in a short time. If clubfoot is neglected or not properly treated beforehand, children can lose their ability to walk normally and become disabled. If you suspect this condition in your child, you should immediately contact an orthopedist who can make the correct diagnosis.At our center you will receive the necessary advice on clubfoot treatment and can confirm or dispel your fears. It takes about two months to correct this abnormality in a child. The main factor that can delay clubfoot treatment for a long period of time is the severity of the deformity. In this case, surgical intervention can be avoided. Chiropractic adjustments, orthopedic shoes, and a gradual change in casts may help. Clubfoot is a developmental disorder that can be detected at birth. In the early stages, clubfoot in infants can be treated in a short time. If clubfoot is neglected or not properly treated, children can lose their normal ability to move and become disabled. If you suspect this condition in your child, you should immediately contact an orthopedist who can make the correct diagnosis. At the Perseus Orthopedic Center you can get the advice you need to prevent and treat clubfoot. With timely treatment, the prognosis is favorable.
Treatment of congenital flatfoot
If a foot deformity is detected at birth, e.g. B. a reduction of the forefoot, the child is observed for about 1 month. In some cases, the deformity is uterine (caused by a spasm of the uterus) and then resolves spontaneously at about one month of age with massage and special exercises. If this is not the case, this foot deformity is also treated with plaster casts in stages. But in this case the number of plaster casts will be less, about 2-3. An achillotomy is not performed, and after the step casts, the result must also be stabilized with clamps, bandages or orthoses until the age of 2-3 years.
A deformity such as congenital flatfoot is also started with a step cast, but in a different way, namely with the Dobbs method. However, there are some differences in treatment. The number of plaster casts is higher, about six to eight, and after the step cast, an operation must be performed in a special trauma surgery and orthopedic department for children. As with clubfoot treatment, a plaster cast is applied to consolidate the result.
In all cases, rehabilitation during the plaster period is recommended. Parents are taught the LFC technique and work on special simulators. The orthopedist also gives recommendations for the right choice of footwear. A general massage is recommended for all children except for the lower extremities and feet.
An important and indispensable prerequisite in the treatment of foot deformities is to establish contact and build a relationship of trust between parents and doctor. Once treatment has started, parents should always keep in touch with the doctor. In case of complaints or doubts, parents can always contact the doctor and ask questions. At the first meeting between the doctor and the young patient, the doctor will answer any questions the parents may have, e.g. B. how the child is to be cared for in all phases of the treatment, how the orthosis is put on and what to pay attention to during the treatment.
In each individual case, the treatment protocol may be modified depending on the foot deformity and the severity of the condition. Each child is unique and treatment is customized. It is important not to miss the moment and make an appointment with a podiatrist. Therefore, if you have concerns, and the diagnosis of a congenital deformity of the foot was made in the first days of life, then you should not wait for a medical examination at the age of one month, but consult an orthopedist yourself as soon as possible.
promotions

You can pave the shortest path to health and active longevity when you have an accurate guide to your own health—a safe guide.

The inpatient department of the LOTOS Medical Center is one of the best day care facilities in the region. Your uniqueness lies in.

QUALITY We work with precise, state-of-the-art equipment that allows us to achieve the most accurate results.

Are you dreaming of a baby, but you can't see the long-awaited two stripes? Have you been diagnosed with infertility? Advantages.
Therapeutic rehabilitation for children in their first year of life
Physiotherapy for children with congenital clubfoot is indicated from the first days of life as part of general orthopedic treatment. At the age of 7-10 days, the toddler's ligaments and muscles can be effectively treated.
The comprehensive LFC approach involves the gradual application of corrective plaster casts. A so-called positioning treatment is carried out, which is reinforced by special massages. After the cast is removed, the massage therapist performs foot and lower extremity exercises, and then reattaches the cast with a corrective bandage.
The purpose of the massage is to ensure that the muscles of the foot and lower leg are completely relaxed. For this purpose, stroking, vibration, kneading, muscle diastasis and stretching of the heel tendons are performed.
After the relaxation massage, muscle tension is released, and the masseur performs the next phase of therapeutic rehabilitation - physical exercises:
- The child's starting position is supine. The goal is to eliminate external adduction of the foot. Suppose the masseur works with the right foot. He applies pressure to the ankle with his left hand, placing the first finger on the outer knuckle and the second finger on the inner knuckle so that the heel rests on the massager's hand. With the right hand on the foot, with the first toe on the outside edge, the massager's curled second toe on the back of the limb, and the third toe on the inside, push the child's foot outward. Do the same with your left foot.
- The starting position is as before. The goal is to eliminate the rotation of the foot in relation to the longitudinal axis. The masseur grasps the child's right foot with his right hand and places the first toe on the sole of the foot and the other toes on the back of the foot. With the other hand, the heel is held. The massage is done by pressing the first toe from bottom to top on the outer edge of the child's limb, while the massage works from top to bottom on the inner edge.
- The starting position remains unchanged. The goal is to eliminate plantar flexion. The therapist's right hand presses the child's left shin against the table so that the first and second toes rest on the ankle. The left hand of the masseur presses the sole of the foot upwards with the palm.
flat feet and fallen arches
There is not only a congenital varus foot deformity, but also a valgus foot deformity.
Even bad joint problems can be treated at home! Just remember to swab once a day to treat this condition.
Flat feet are an orthopedic form of foot deformity in which the arch of the foot is flattened. It is associated with loss of cushioning function and is a common deformity.

In orthopedics, there are several types of flat feet.
type of deformation Cause and characteristics of the disease Congenital flatfoot Clinical pathology caused by underdevelopment of the fibula, retention of the amniotic sac, or embryonic defects. rickety flatfoot A consequence of rickets in young children. Flat feet are caused by softening of the bones and weakening of the muscles and ligaments. The child's foot becomes plastic under the weight of the body, the arch of the foot sinks and the forefoot sticks out. Paralysis of the flat foot Cerebral palsy secondary to poliomyelitis. The severity depends on the number of shin muscles damaged - one or two. Post traumatic flat foot Deformity of the foot caused by a fracture of the tarsal bone or an abnormal stiffening of the ankle. Static flat foot The main cause of valgus deformity is poor muscle tone. The latter type of orthopedic disease is the most common. Early signs of static ankle deformity include rapid ankle fatigue and calf muscle pain when running or walking.
This type of valgus deformity is very difficult to treat. Therefore, special attention is paid to the prevention of flat feet:
General information.
The foot as a group of diseases occupies a special place among congenital pathologies.
Even if the diagnosis seems easy, late treatment is often unsatisfactory because the patient later walks on a deformed foot, with significant social consequences.
Clinical relevance in outpatient practice The most common foot deformities are..
- – Clubfoot (metatarsus varus, metatarsus adductus, clubfoot);
- – congenital flat valgus foot;
- – heel foot;
Metatarsus adductus ('sickle foot').
The outer contour of the foot is convex, the forefoot is lowered. Passive manual corrections are possible due to the plasticity of the foot. In some cases, spontaneous regression in old age is possible.
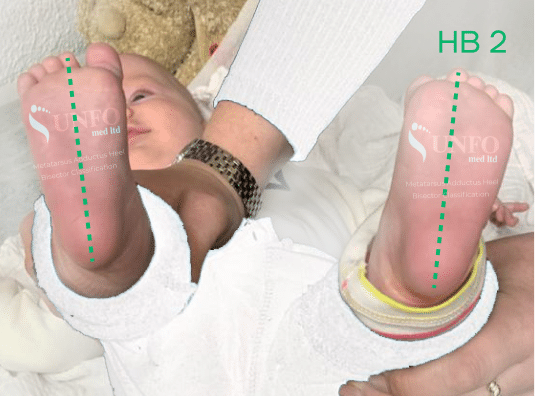
The child has metatarsus adductus (minimal adduction of the forefoot) and pes valgus (valgus flatfoot).
This is caused by hypertonia of the tibialis anterior muscles and hypotonia of the tibialis posterior muscles, ie there is an imbalance in the tonus of the foot muscles, resulting in a deformity of the foot.
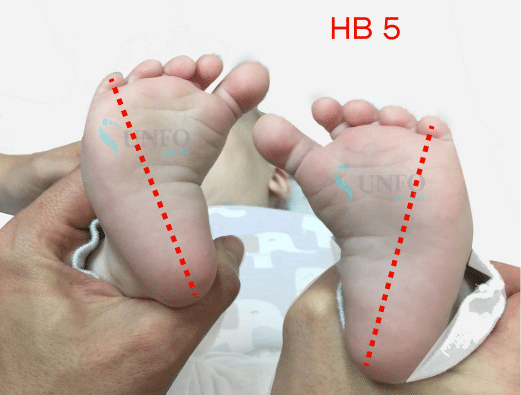
The most important factor is the type of deformity - rigid (cannot be passively corrected) and non-rigid (can be corrected). As can be seen in the photo, the degree of adduction is minimal, so most likely it is a non-rigid deformity.
– Daily physical therapy with trainer, stretching exercises or passive manual manipulation.
– orthoses, footwear.
– Foot and lower limb massage.
– Myostimulation
– Paraffin and ozokerite applications on the lower leg.1. Individual orthopedic insoles. Orthopedic footwear with Thomas heel, high toe or rear heel, 1 cm heel.
3. Foot Therapy. Lower limb massage with emphasis on lower legs and feet 4 times a year for 10 sessions.
5. 10 treatments with SMT stimulation on lower legs and feet four times a year.
6. 10 treatments with paraffin ozokerite on lower legs and feet 4 times a year. Electrophoresis with euphyllin on the lower leg muscles #10, 2 times a year.
8. 1000 IU vitamin D daily - prophylactic dose.
9. Orthopedic observation once every 6 months or more frequently.FYI – Metatarsus adductus can resolve spontaneously (without treatment) in most children.
If severe deformation or in the absence of a positive trend during follow-up, a graded cast is effective.
If there is residual adduction of the forefoot at the beginning of walking and functional impairment, shock-absorbing shoes are indicated.
clubfoot
In clubfoot, the bottom of the foot is turned inward, causing the arch of the foot to pull up. This defect is usually caused by the baby's position in the uterus, does not always resolve after birth, and may require plaster casts.
In heel deformity, the foot is flat or rounded and arched in the plantar direction with the heel pointing outward.
Early treatment with a cast or corrective splint is usually effective.
flat feet
In flat feet, the normal arch in the midfoot area is flattened. Flat feet occur in all children up to the age of about 3 years, after which the arch of the foot begins to form. There are two basic types of flat feet:
W With flexible flatfoot The foot stays flat because the arch is extremely flexible. A flexible flat foot usually does not need treatment. However, if an older child experiences pain or cramps in their feet, corrective footwear may be needed.
If tarsal stiffening The foot is fixed in a flattened position. A stiffening of the tarsus can be a congenital defect or as a result of a disease, e.g. B. a trauma or a long-lasting swelling. The treatment of a tarsal stiffness is often done with a plaster cast. Sometimes foot mobility is restored by surgically separating the stiff joint.
Copyright © 2023 Merck & Co, Inc, Rahway, NJ, USA and its subsidiaries. All rights reserved.
- Massage for flat feet.
- Clubfoot in children therapeutic exercises 7 years old.
- baby splashing.
- Photo of scraped feet.
- Why does a child develop clubfoot?.
- Clubfoot in 7-year-old children.
- How to remove a clubfoot.
- What is clubfoot?.