Rhabdomyolysis is an extreme degree of muscle damage in which large numbers of muscle cells are destroyed at the same time. The severity varies greatly, ranging from subclinical forms that can only be detected through laboratory tests to life-threatening conditions. The frequency of this disease is not precisely defined. About 26,000 cases of rhabdomyolysis are recorded annually in the United States, but experts believe that this number does not correspond to the true frequency of the disease due to the hypodiagnosis of deleted variants.

- Treatment of contractures
- Basics of treating contractures
- Endoscopic plantar fasciotomy and heel spur removal.
- Mini-invasive transection of the plantar fascia and removal of the heel spur under X-ray control.
- Head and spinal cord injuries in mine explosions
- Abdominal injuries
- Rehabilitation after treatment of Dupuytren's contracture
- Fasciotomy – Fasciotomy
- complications
- complications
- Treatment of rhabdomyolysis
- Conservative treatment
- surgical treatment
- complications
- Treatment of complex pachyderma
- Symptomatic treatment
- surgical treatment
- prognosis and prevention
- Update of the guideline on compartment syndrome (AAOS, January 2019).
- Reviewer
Treatment of contractures
Treating contractures is difficult, time-consuming, and labor-intensive. The patient's age, determination and motivation play an important role. The result of contracture treatment depends on how long ago the contracture occurred, what it was like and where it was located.
- If a congenital contracture is discovered soon after birth, complete cure is possible;
- Transient contractures caused by reflexive muscle contraction spontaneously normalize as motor activity resumes and blood flow improves;
- Active contractures are quite effective in the initial stages, but if left untreated, severe changes in bone surfaces occur and the active contracture becomes passive; in this case treatment is more difficult.
- In case of contractures of hysterical origin, a consultation with a psychotherapist and treatment by an appropriate specialist is necessary.
The treatment of persistent contractures is lengthy and complicated. It is necessary to patiently follow the doctor's instructions and not resort to self-medication. Only then can a satisfactory result be achieved.
Basics of treating contractures
The aim of treatment is to eliminate pain, inflammation and swelling, restore full mobility to the joint and avoid complications. This is achieved through conservative methods and, as a last resort, through surgical techniques.
The principles of conservative treatment of contractures are the same everywhere. These include symptomatic pharmacotherapy, positioning and exercise therapy and physiotherapy.
- Medication.
- Analgesics and NSAIDs reduce pain and inflammation;
- Myorelaxants act on muscle tissue;
- Hormone therapy reduces inflammation and persistent pain;
- Joint blocks are prescribed for severe pain.
- security scheme
Positioning treatment involves wearing a special orthosis for a certain period of time and stretching the contralateral tissue. The force applied should be small. The orthosis or splint should only be applied by a specialist! It should not be used under anesthesia or with force. The pressure must be gentle, painless and continuous. This is achieved by continuously adjusting the orthosis and literally changing it microscopically so that the patient does not feel any pain.
In severe cases, skeletal traction and forced deformation correction (redressing) are used. This includes:
- the gradual application of plaster casts;
- removable bandages that are fixed with elastic bandages;
- Ilizarov brackets are helpful in some cases;
- Articulated trusses produce good results.
Forced single-stage erection should only be carried out by an experienced doctor! If the technique is incorrect, the periarticular tissue can be torn and the consequences can be irreversible.
The range of physiotherapeutic treatments is very diverse. They are primarily used after specialist treatment of atrophied muscles.
Endoscopic plantar fasciotomy and heel spur removal.
Endoscopic fasciotomy. First carried out in 1991. Performed under regional anesthesia. Under a tourniquet on the tibia. A 5 mm long port is created on the medial surface of the heel, approximately 1 cm distal to the aponeurotic insertion. The endoscopic trocar and cannula are inserted superficially from the plantar fascia to the opposite edge of the heel, where an exit wound is created. The cannula is removed and the endoscopic camera is inserted into the medial portal. A retrograde cutting scalpel is inserted into the lateral approach. And the dissection is carried out.
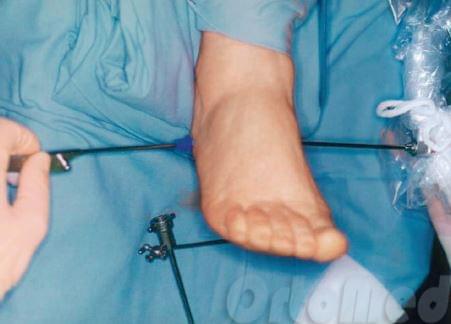
The surgeon can use the camera to observe the operating area. The plantar fascia is cut away from the heel spur (bone) so that its tension is released.
Mini-invasive transection of the plantar fascia and removal of the heel spur under X-ray control.

In contrast to the endoscopic technique, only an incision of 3 mm is made. A three-bladed scalpel is inserted through this to cut the plantar fascia at the point where it connects to the heel bone.

The exostosis (spur) of the heel bone itself is then removed with a hoe. A major advantage of this method is the minimal trauma to the heel area (sole of the foot). This shortens the rehabilitation time to 2 days.

Many patients ask me: Can flat feet get worse after fascia removal?
No. The flat feet will not get worse because during the operation we only cut the medial (inflammatory) fascia, but the lateral fascia, which is connected to the calcaneus of the same name, remains intact. When heel pain is severe, gait disorders are much more dangerous. The patient reflexively begins to shift his body weight to the forefoot and the other foot. A limp or poor posture may occur. All this can lead to accelerated progression of osteochondrosis or scoliosis!
The results of the heel spur surgery and the x-rays can be viewed here.
Head and spinal cord injuries in mine explosions
The most common component of multifactorial trauma. Penetrating cranial wounds are the most severe, and damage to the dura is the diagnostic criterion as it represents a reliable barrier to the penetration of infection into the cranial cavity.
In the clinical compensation and clinical subcompensation phases, there are usually focal symptoms but no impairment of vital functions. The moderate clinical decompensation phase is characterized by bradycardia, hypertension, shortness of breath, and deep breathing, reflecting increased cerebral edema and impaired vital functions.
The deep clinical decompensation phase is manifested by a change from bradycardia to tachycardia, from hypertension to hypotension, and from infrequent and deep breathing to frequent and shallow breathing. It develops against the background of coma and is characterized by first-degree cerebral dislocation, in which the brain stem is pressed into the cerebellar opening as a result of swelling or compression, a complication of severe traumatic brain injury or late-stage brain compression.
The final stage develops in a second-degree cerebral dislocation, in which the brain stem is blocked up to the greater occipital foramen. It is characterized by progressive tachycardia and hypotension, respiratory arrhythmias up to respiratory arrest and is characteristic of extremely severe brain injuries and irreversible stages of brain compression.
Spinal cord injuries are less common and their extent is difficult to determine in the early stages due to the development of spinal shock, a series of initial symptoms of spinal cord dysfunction that far exceed the extent of neurological damage commensurate with the actual degree of injury. Profound neurological deficits can also occur in the event of a glancing blow if the bony structures of the spine are not damaged. This is usually associated with cerebral hemorrhages, epidural and subdural hematomas, and compression of the spinal cord by intervertebral discs protruding into the spinal canal.
Abdominal injuries
In the case of abdominal jet injuries, the resulting disorders are due to the sum of pathological interactions, which primarily include massive blood loss, endotoxemia and dysfunction of vital organs.
This type of injury is characterized by the predominance of closed injuries to parenchymatous organs (liver, spleen, kidneys).
The great diagnostic difficulties caused by reciprocal severity syndrome require a thorough dynamic examination of the injured person. It should be noted that abdominal pain and distension, abdominal peristalsis, palpation, and abdominal wall tension may occur with abdominal soft tissue injury or significant retroperitoneal hematoma without internal organ injury.
Worsening of the injured person's condition (hypotension, persistent or increasing tachycardia, etc.) without a noticeable effect of intensive infusion and transfusion therapy indicates persistent bleeding, of course, after excluding other sources.
Hematuria is usually an indication of bladder or kidney damage. In all cases, rectal inspection and rectal palpation should be performed.
The main radiological signs of closed abdominal trauma are gas in the abdominal or retroperitoneal cavity, fluid in the abdominal cavity, distension and displacement of the stomach and intestines, and abnormal position, shape and function of the diaphragm.
Intravenous urography, retrograde pyelography, cystography and urethrography are performed if kidney, ureter and bladder injuries are suspected.
A very important diagnostic method is laparocentesis, for which the following indications apply: unclear clinical picture of intra-abdominal trauma; severe combined head, thorax and pelvic trauma with loss of consciousness; combined thoracic, spinal and pelvic trauma when acute abdominal symptoms occur. After laparocentesis, if this is negative, a drain is left in the abdominal cavity for 1-2 days for diagnostic observation.
Rehabilitation after treatment of Dupuytren's contracture
After a needle aponeurotomy, fingers can be used as early as 2 hours after the procedure. Bandages are not required after this procedure. Only regular observation by the treating doctor (orthopedist).
After open surgery (aponeurotomy, partial aponeurectomy, total aponeurectomy), bandages and observation by the attending physician are required for 2 weeks until the surgical wounds have healed and the sutures have been removed. On the 3rd postoperative day, a functional splint (extensor splint) is applied to keep the fingers in the correct position. If the contracture is mild, the splint can be worn for a short time. If you want, you can do without the splint, but then the patient has to regularly lengthen the finger himself until it becomes painful. It's not enough to simply operate, that's only half the battle. Postoperative rehabilitation in the treatment of Dupuytren's contracture is one of the most important stages.
In addition to wearing a splint, rehabilitation is often accompanied by physiotherapy (magnetic laser therapy before the removal of the stitches, phonophoresis, electrophoresis with hydrocortisone after the removal of the stitches) and mandatory physiotherapy.
Do not self-medicate!
Only a doctor can make a diagnosis and prescribe the correct treatment. If you have any questions, you can call us or send us an email.
The cost of surgical treatment of Dupuytren's contracture is from RUB 32,000.
Cost of needle aponeurotomy – 15,000 (1 finger).
Fasciotomy – Fasciotomy
Fasciotomy or Fasciectomy – is a surgical procedure in which fascia is severed to relieve tension or pressure to treat loss of blood flow to an area of tissue or muscle. Fasciotomy is a limb salvage procedure to treat acute compartment syndrome. It is also sometimes used to treat chronic compartment syndrome. The procedure has a very high success rate, with the most common problem being accidental damage to a nearby nerve.

complications
Delaying the procedure may result in neurovascular complications or the need for limb amputation. Complications may also include the formation of scar tissue after surgery. Thickening of postoperative scar tissue can lead to loss of mobility in the affected joint. This can be managed with professional treatments or physiotherapy.

Limb fasciotomy is usually performed by a surgeon under general or regional anesthesia. A small part of the fascia is removed through a skin incision to relieve the pressure as best as possible.
The plantar fascia is an endoscopic procedure. The doctor makes two small incisions on either side of the heel. An endoscope is inserted into an incision to guide the doctor. A small knife is inserted into the other. Part of the fascia in the heel area is removed. The incisions are then closed.
In addition to a scar, the surgeon may need a skin graft to close the wound. Sometimes, when the fascia is closed again during another surgical procedure, the muscle is still too large to close completely. A slight bulge may be visible, but it is not dangerous. Healing takes much longer, in some cases even several months.
complications
In addition to ARF, which is the main cause of death, life-threatening conditions such as hypovolemic shock and DIC can occur with rhabdomyolysis. Sometimes fatal cardiac arrhythmias occur as a result of hyperkalemia and kidney failure. The patient's immune system is suppressed and severe infectious complications, including sepsis (30-70 % of patients), are common.
The diagnosis is made by trauma surgeons, intensive care physicians or specialists who cared for the patient before the muscle necrosis occurred (infectious disease specialists, rheumatologists, etc.). The clinical diagnosis of rhabdomyolysis in trauma is usually easy to make based on a combination of a characteristic history and significant local swelling in the area of the lesion, which has a woody consistency.
Muscle necrosis of non-traumatic origin is often difficult to differentiate clinically due to the nonspecific nature of the symptoms, the extent of the process, previous illnesses of the patient and the possibility of other complications of the underlying disease. A change in urine color is not a specific sign of rhabdomyolysis, as it can be caused by both hemoglobinuria and myoglobinuria. In some cases, a genetic diagnosis makes sense. The most important role in the diagnosis is played by:
- Biochemical blood test. Elevated myoglobin and creatine phosphokinase levels are early specific signs of rhabdomyolysis. Marker activity increases gradually over the first 12 hours, with myoglobin concentration peaking on day 1 and CPK concentration peaking on days 3-5. In addition, the analysis shows acidosis, increased creatinine, uric acid, hyperkalemia, hyperuricemia, hyperphosphatemia and hypocalcemia.
- Assessment of 'diuresis. The development of ARF is indicated by a decrease in diuresis by 8-10 %. Diuresis then decreases by 25 % or more; in severe cases anuria is possible. An increase in urine volume indicates the restoration of kidney function; at this time, daily urine production can reach 5 liters.
- urine test. Myoglobinuria, proteinuria, and electrolyte abnormalities are detected in the urine of patients with rhabdomyolysis. The urine density is changed, the ratio of urea/creatinine in the blood and urine as well as the ratio of sodium/creatinine clearance are determined.
Treatment of rhabdomyolysis
Conservative treatment
Suspicion of rhabdomyolysis is an indication for intensive care unit emergency room, early use of infusion therapy and control of diuresis. Patients are prescribed a special diet that limits products containing protein and potassium. The underlying pathology causing rhabdomyolysis is corrected. Pharmacotherapy depends on the stage of the disease and the severity of the patient's condition and may include the following
- Prevention of ARF. Upon admission, patients receive diuretics and sodium bicarbonate solution via an intravenous drip to reduce damage to the renal tubules by myoglobin casts.
- Correction of hypovolemia. Saline infusions for rhabdomyolysis should be started within 6 hours of injury. The amount of fluid injected reaches 1 l/hour in the first 2 hours and 500 ml/hour in the following 2 hours. The infusions are administered under the control of diuresis and CPR of the blood. Efforts are made to ensure urine output greater than 300 ml/hour.
- Treatment of intoxications and metabolic disorders. Calcium gluconate and sodium bicarbonate are administered intravenously. Beta-adrenoceptor agonists and insulin with glucose are used. Enterosorbents are used to reduce the absorption of toxins in the intestines.
- Extracorporeal hemocorrection. Hemosorption is considered a promising treatment for rhabdomyolysis. In some cases, plasmapheresis is prescribed. In cases of ARF, hemodialysis is performed.
surgical treatment
Surgical treatment of rhabdomyolysis is either prophylactic or curative and is performed within the first hours of hospital admission or within 1-2 weeks of admission. Surgical techniques used are:
- Decompressive fasciotomy. The goal of surgery is to relieve pressure in the muscle sheath when compartment syndrome develops. This technique reduces the occurrence of necrosis and reduces the likelihood of gross metabolic abnormalities and ARF.
- Necrectomy. It is performed for deep thermal burns, electrical trauma, long crush syndrome and other injuries and vascular diseases. In severe cases, amputation or disarticulation of the limbs is performed.
complications
The main problem of positional compression syndrome is acute renal failure, which is accompanied by massive myoglobinemia. The development of ARF increases the likelihood of death threefold and correlates with an unfavorable long-term prognosis. Of great importance are complications of the underlying disease or intoxication that caused compression of the soft tissues of the body.
Depending on the prevailing symptoms, the patient is examined by an intensive care doctor or a trauma surgeon. A detailed history is essential, the circumstances preceding the injury should be explained, the exact position of the patient as well as chemical dependencies and other risk factors should be determined. The following techniques are used in the diagnosis of positional compression syndrome:
- Soft tissue ultrasound. Ultrasound diagnosis shows signs of damage to the compressed muscles: wasted muscle pattern, absence of transverse stripes and mosaic hypoechoic zones (myolysis foci). To rule out a venous cause of PPS, a Doppler ultrasound of the affected area is indicated.
- Radiography. Radiological imaging is informative to exclude dislocations and fractures, which, when combined with external skin lesions, give a similar clinical picture. Radiographic changes are not observed in positional compression syndrome.
- ECG. The electrocardiogram shows signs of hyperkalemia: altered QT interval, increased T waves in the chest leads, single bigma and ventricular premature beats. The examination is supplemented by a cardiac ultrasound, which does not reveal any pathological changes.
- Biochemical blood test. The main diagnostic sign is an increase in myoglobin in the blood above 1000 ng/ml, which correlates with a high risk of kidney damage. An increase in blood creatinine levels suggests the development of renal dysfunction, which, combined with a reduced glomerular filtration rate, confirms the diagnosis.
- Urinalysis. In PPS, the specific gravity of urine is above 1015 and contains large amounts of myoglobin. The osmolarity is more than 500 mosm/l, the sodium content is less than 20 mmol/l. An osmolarity ratio of urine to plasma of more than 1.1 is characteristic.
Treatment of complex pachyderma
Symptomatic treatment
No uniform scheme has been developed for the treatment of pachyderma. The treatment measures depend on the disease and the wishes of the patient. It is important to maintain local scalp hygiene in order to avoid secretion accumulation, maceration, unpleasant odor and secondary infections. If an infection occurs, antibiotic therapy, retinoic acid preparations and zinc pyrithione shampoos are recommended to care for the scalp.
In secondary pachyderma, the focus is on treating the underlying disease. To treat dermatitis, topical GCS are used, to improve tissue trophics, vasodilators, antihypoxants and corrective microcirculation are used. Physiotherapy is carried out: electrophoresis and ultraphonophoresis with lidase, laser therapy.
surgical treatment
Plastic surgeries are performed to improve appearance. However, they do not prevent the progression of pachydermal folds. The following techniques are used for aesthetic correction:
- Percutaneous needle fasciotomy. It allows tension in skin folds to be released by making deep incisions in the skin with a hypodermic needle.
- Scalp lifting. Here, the excess dermis that forms the wrinkles is resected and the skin is then lifted in the longitudinal and transverse directions. Extensive resections may require the use of tissue expanders or free flap skin grafts to close the defect.
prognosis and prevention
Primary pachydermal folding is a progressive disease that cannot be completely cured. With medical procedures and proper care, only improving appearance, eliminating unpleasant symptoms and complications are possible. No cases of malignant skin lesions have been reported.
The prognosis of secondary pachyderma is related to the course of the primary disease. Prevention is also about avoiding possible causes (trauma, infectious dermatitis of the scalp, steroid use) and preventing systemic diseases.
1. folded pachyderm of the scalp / V. Okhlopkov, E. Zubareva, E. Radul, S. Bocharova // Russian Journal of Cutaneous and Venereal Diseases. – 2015.
2. clinical case of scalp complex pachydermia / Nemchaninova OB, Sklyanova E.Yu., Sokolovskaya AV, Chernikova EV, Reshetnikova TB, Pozdnyakova ON // Pharmateca. – 2021. – Т.28, №8.
3. The folded pachyderm of the scalp / Pankratov VG, Pankratov OV, Kasperovich LS // Medical Journal. – 2002. – №2.
Update of the guideline on compartment syndrome (AAOS, January 2019).

On January 17, 2019, the American Academy of Orthopedic Surgeons updated its guidelines on compartment syndrome.
-There is limited evidence that myoglobinuria and serum troponin levels may be helpful in diagnosing acute compartment syndrome in patients with traumatic lower limb injuries.
-There is moderate evidence that in patients with acute vascular ischemia, testing of femoral vein lactate levels, performed during surgical embolectomy, may be helpful in diagnosing acute compartment syndrome.
– There is limited evidence that myoglobinuria not is not helpful in diagnosing acute compartment syndrome in patients with electrical trauma.
– This point is an expert opinion as there is no reliable evidence: Serum biomarkers do not provide any useful information when considering fasciotomy for suspected long-standing or overlooked acute compartment syndrome.
– There is moderately strong evidence that intracompartmental pressure monitoring is helpful in the diagnosis of acute compartment syndrome.
- There is moderate evidence to support the use of repeated/continuous intracompartmental pressure monitoring and the use of a diastolic blood pressure threshold minus intracompartmental pressure > 30 mmHg to rule out acute compartment syndrome.
– This point is an expert opinion due to the lack of reliable evidence: Intracompartmental pressure monitoring there are none useful information when considering fasciotomy in adult patients with evidence of irreversible intracompartmental (neuromuscular/vascular) damage.
Reviewer
Author of reviews for medical journals on MedElement – General Practitioner, Surgeon Talant Imanalievich Kadyrov.
He graduated from the Kyrgyz State Medical Institute (red diploma) and is fluent in English. Has experience as a surgeon in Chui Regional Hospital; currently working in private practice.
Regular training: Advanced Cardiac Life Support, International Trauma Life Support, Family Practice Review and Update Course (England, USA, Canada).
- Self-treatment can lead to irreversible damage to health.
- The information contained on the MedElement website and in the MedElement, Lekar Pro, Dariger Pro and Disease: Therapist's Guide mobile apps cannot and is not intended to replace direct medical advice. Always seek the advice of your doctor if you have an illness or symptoms that worry you.
- The choice of medication and its dosage should be discussed with a specialist. Only your doctor can prescribe the right medication and dosage considering your disease and condition.
- The MedElement website and mobile apps MedElement, Lekar Pro, Dariger Pro and Disease: Therapist's Guide are for informational purposes only. The information contained on this website should not be used to inadvertently change your doctor's recommendations.
- MedElement is not liable for any personal injury or property damage resulting from the use of this website.
- blunt.
- Pronation of the shoulders - what is it?.
- squinting in adults.
- straightening of the fingers.
- Why are a teenager's toes crooked?.
- Treatment of plantar fasciitis.
- A tricky stump.
- Immobilization of the ankle.