They like to diagnose people who don't understand that we're not the first. And specialists make a healthy child sick and vice versa. So many of my friends left at 14 or paid a premium or left at 9.

- Equinovarus deformity and longitudinal foot: treatment of clubfoot
- Equinovarus foot
- Congenital clubfoot
- Therapeutic rehabilitation for children in their first year of life
- How are the legs corrected for varus curvature?
- Massage your child's legs. Example.
- Also read:
- 14 answers.
- Lower limb deformities in children and their treatment
- The main symptoms of lower limb deformities, apart from the visually visible changes
- Treatment of varus foot deformity (O-foot)
- Why is treatment of varus deformity mandatory?
- Factors that characterize varus deformity of the foot:
- Consultation with an orthopedic surgeon:
- Congenital clubfoot
- Therapeutic rehabilitation for children in their first year of life
- Tips for prevention
- Video
Equinovarus deformity and longitudinal foot: treatment of clubfoot
Podiatrists take great care to ensure that all body parts function properly immediately after birth. It is known that the earlier a disorder is recognized and the sooner it is actively treated, the better the chances of a full recovery later. The most common illnesses in infants involve problems with the musculoskeletal system. In this review we will address a painful problem for many parents and find out what equinovarus foot deformity is, how it is treated using classical methods and how effective surgical intervention is. We will also take an in-depth look at pathogenesis and species diversity.
It is worth remembering that modern medicine makes it possible to diagnose and effectively treat many problems at an early stage. Previously, clubfoot was considered a congenital syndrome that could not be completely eliminated, only the symptoms could be alleviated, but today there is a solution. However, it is important that you take care of it in good time. In advanced stages of pathology, even surgery cannot guarantee a reliable result. In addition, the disease can also be acquired remotely.

Equinovarus foot
This is an abnormal position of the foot. It is characterized by the fact that the inside is raised and slightly curved. The outside, on the other hand, tends to be sunken. It appears as if the person is standing on an edge and the position of the foot looks very unnatural. Not to be confused with the equinus position. When it occurs, the patient moves as if on tiptoes, leaning against the front of the surface.
The catch, however, is that the degree of deviation directly determines how strong it is. While in severe cases it is easy to detect the abnormality without being a doctor or an expert in the field by simply taking a quick look, in less severe stages it is difficult to detect the deformity visually.
And this pathology tends to progress. This happens regardless of the original cause. It is often caused by spastic forms of cerebral palsy. Therefore, if you do not start emergency measures in time, the current condition may worsen and develop a more serious illness. This can make future fights more difficult.
This condition is a type of valgus, commonly referred to as clubfoot.
Congenital clubfoot
Clubfoot is a congenital musculoskeletal anomaly characterized by a bilateral malalignment of the lower limbs in which the feet are on the outer edge.
The characteristic symptoms of this congenital orthopedic anomaly are:
- Varus deformity of the foot in the newborn, when the sole part is bent downward and inward;
- Supination of the foot, when the sole of the foot is turned inward and the supporting part becomes the tarsal or metatarsal bone;
- Adduction, when the arch of the foot is enlarged and directed inward in the forefoot area.
The degree of these symptoms varies both upwards and downwards. Sometimes the supination of the child's lower limbs is so pronounced that the inner heel touches the ankle joint, and a pronounced varus deformity pulls the heel up and turns it inward.
According to medical theory, congenital bilateral clubfoot is defined both as a mild form (osteal sac varus contracture), in which the talar head protrudes with little skin mobility, and as a soft tissue and ligamentous form, in which the skin layer is well developed and there is no bony protrusion is available.
Varus deformity of the foot in children with congenital bilateral clubfoot is characterized by an inward displacement of the tibia, which limits the mobility of the ankle joint support system.
The severity of the situation worsens when the child begins to walk. There is thickening of the skin on the outside of the foot, gradual atrophy of the ankle muscles in the calf area, and an X-shaped recurrence of the knee joint.
According to medical experts, varus deformity of the lower limbs in children with bilateral clubfoot has a different cause and effect:
- Contact anastomosis of the amniotic membrane (membrane of the embryo) with the embryo, with gravity pressure of the amniotic membrane against it;
- Belt pressure of the umbilical cord on the lower limbs of the fetus;
- muscular compression of the uterus on the external surface of the fetal foot due to low amniotic fluid;
- compression of uterine tumors;
- impaired spinal innervation of the fetus.
Therapeutic rehabilitation for children in their first year of life
Therapeutic physical training (LFC) for children with congenital clubfoot is indicated from the first days of life against the background of general orthopedic treatment. At the age of 7-10 days, the child's musculoskeletal system is effectively treated.
The comprehensive LFC approach involves the gradual application of corrective casts. A so-called position therapy is carried out, which is reinforced by special massages. After removing the cast, the massage therapist performs exercises on the foot and lower leg, followed by repositioning with a corrective bandage.
The massage is intended to ensure complete relaxation of the muscles of the foot and lower limbs. For this purpose, stroking, vibration, kneading, muscle diastasis and stretching of the heel tendons are carried out.
After the relaxation massage, muscle tension is released, and the masseur performs the next phase of therapeutic rehabilitation - physical exercises:
- The starting position for the child is lying on his back.. The goal is to eliminate external adduction of the foot. Let's say the masseur is working on the right foot. Pressure is applied to the ankle with the left hand, with the first finger on the outer ankle and the second finger on the inner ankle, so that the child's heel rests on the massage therapist's hand. With the right hand on the foot, with the first finger on the outside edge, the massager's curved second finger on the back of the limb, and the third finger on the inside, press the child's foot outward. The same applies to the left foot.
- The starting position is as before. The aim is to eliminate rotation of the foot in relation to the longitudinal axis. The masseur grasps the child's right foot with his right hand and places the first toe on the sole of the foot and the others on the back of the foot. The heel is held with the other hand. The massage is carried out by applying pressure on the first toe from bottom to top on the outer edge of the child's limb, while the massage acts from top to bottom on the inner edge.
- The starting position does not change. The goal is to eliminate plantar flexion. The masseur's right hand presses the child's left shin against the table, with the first and second fingers resting on the ankle joint. The masseur's left hand presses the sole of the foot upwards with the palm of his hand.
How are the legs corrected for varus curvature?

In children, varus curvature of the legs can often be corrected with conservative measures.
The first step is to treat the underlying condition that caused the deformity. For example, vitamin D is prescribed for rickets. In addition, special orthoses and other orthopedic aids, massages and therapeutic exercises are used.
In adulthood, the deformity can only be corrected through surgery. A corrective osteotomy is then performed. In 2010, researchers at Volgograd State Medical University published a paper in which they concluded that axial osteotomy of the tibia using an Ilizarov apparatus is effective for dysplastic labral curvatures of the legs.
Massage your child's legs. Example.
The parents of a boy came to the Happy Baby Center when the child was 1 year and 2 months old. The baby's legs were O-shaped and the sight was frightening. We had a course of 10 massage treatments. We massaged his knees thoroughly. We did a general treatment. He did gymnastics to strengthen the main muscle groups, as well as special exercises, as described above. After working on the knees, we wrapped elastic bandages around the knee joints. A soft pad was placed between the ankles (medial surface of the ankle joint). The braces should stretch the inner edge of the knee joint capsule to make it more flexible and deformable for leg alignment. After the first ten massage sessions, the parents noticed positive dynamics.
After this course, no further massages were performed. The mother received recommendations for gymnastics, including from the district children's clinic. According to the mother, they did primitive exercises like 'cycling', 'leg raises' etc. but not for long. The child simply lived according to a fixed schedule. He went outside alone, without support. The legs were slowly but surely corrected, under the pressure of gravity, with wide feet while walking, the bones and joints of the lower limbs are transformed, it is important to create the conditions to help the body begin this process, what we tried to do with massage and stretching. Check out the before and after pictures of the correction (treatment) of the varus O deformity of the child's legs. Overall, this is a merit of the child's body, we just helped him a little.
Also read:
If you found this article interesting, please share it on social media, maybe someone else will find it useful. Moms always have a lot of questions, let us help them find the answers!
14 answers.
Lower limb deformities in children and their treatment

Lower limb deformities are congenital or acquired anomalies that involve changes in the length, shape and axis of the limbs (legs). They can be noticeable in the child's footwear and gait.
Orthopedists distinguish between the following types of foot and toe deformities: flatfoot, clubfoot, clubfoot, equine foot, heel foot, hollow foot and flatfoot. Sometimes a combination of several deformities occurs. In the first year of life, it is important not to rush the child onto its feet, as the load on the feet increases as the weight increases.
The main symptoms of lower limb deformities, apart from the visually visible changes
- Inability to fully straighten the knees;
- The child becomes less active,
- and unsteady gait,
- feeling of heaviness,
- Pain in the legs;
- difficulty walking,
- running, playing;
- Frequent falls of the child,
- and frequent falls and clumsy jumps.
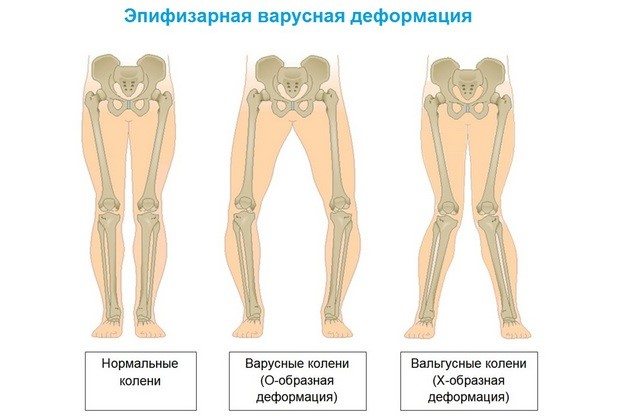
A valgus tibia deformity is X-shaped when the legs are straight, the knees touch, and the distance between the feet is greater than 5 cm, creating a valgus foot deformity. The causes of this condition can be congenital or acquired.
Varus deformity of the lower limbs – the O-shaped foot is visually round, creating a varus deformity of the foot. This deformation puts strain on the ligaments and increases the load on the joint tissues of the lower limbs. Varus misalignment of the knee joint can be a congenital or acquired defect.
Congenital shin deformity is caused by abnormal development of the fetus, which can be detected during pregnancy.
Acquired leg deformities in children are caused by a strong load on the foot due to abnormal development of the joints, ligaments and the entire musculoskeletal system, as well as vitamin D deficiency. This defect can be detected as early as two years old, when the child begins to walk independently.
Treatment of varus foot deformity (O-foot)
Most treatments for O-shaped feet are surgical. There are many different methods, but the Ilizarov brace is the most commonly used treatment for valgus. The main principle of this surgical procedure is to cut the bone at the site of the deformity and allow it to grow together in its correct position.
This method is quite good, but has the major disadvantage that it is traumatic. The Ilizarov device leaves many unsightly scars, and its use can lead to infections. The doctors at the Ladisten Medical Center use a patent from our chief physician in their practice - the Veklich device. The brace is minimally traumatic, does not leave large scars, treatment with the Veklic structure has a short rehabilitation period and the operation is practically bloodless.
Why is treatment of varus deformity mandatory?
It is important to detect and eliminate the pathology in a timely manner in order to avoid undesirable consequences:
Leg straightening in children and adults is carried out in the Ladisten clinic by osteotomy with partial bone transection and fixation before stiffening in the correct position with the help of external fixation devices. The operations to correct leg curvature in children and adults (women and men) performed in our medical center include.
- The use of patented external fixation devices (AVF) developed by the founder and managing director of the Ladisten Clinic, medical student Veklich V. They are lighter than Ilizarov devices and can support more patient weight;
- Minimal soft tissue trauma as each Veclitz brace is inserted into the leg with only three 2mm punctures through which the bone is cut and secured;
- Virtually bloodless operation - the puncture sites are chosen where there are no large blood vessels;
- Using the most modern X-ray equipment, which allows precise dissection of the bone and correction of its position;
- Quick recovery from surgery and short rehabilitation period. Rapid healing of puncture wounds that heal with little or no scar;
- Possibility of straightening bowed legs at the knees, shins and feet using the same device, with the design being adjustable depending on the location and degree of the deformity and the individual anthropometric data of the patient.
The operation to correct bow leg curvature is performed under epidural anesthesia, and the insertion of AVF on one leg takes 15 minutes. One month after the operation you will be able to walk independently and without support, and after two months you can have the devices removed. Removal of Beklich external fixation devices is non-surgical and takes 10-25 minutes depending on type and design.
Factors that characterize varus deformity of the foot:
- more uneven; 'wobbly', unsteady gait, tendency to fall frequently;
- pain in the foot;
- inability to straighten the knees; the knee joints develop unevenly;
- If you look at the child's shoes, you can see that the shoes are worn on the outside of the sole.
The final diagnosis of a varus misalignment of the foot can only be made by an orthopedic trauma surgeon in a personal consultation.
Consultation with an orthopedic surgeon:
At the initial stage of development of varus deformity in children's feet, the curvature can be corrected quite quickly - specially selected orthopedic shoes, a set of exercises, physiotherapy and therapeutic massage can help.
Since the ligaments and muscles are fully developed and strengthened by the age of 7, complete correction of the child's curvature is possible. The most important thing is early treatment and appropriate management to prevent the development of complications.
Children with a varus deformity need special orthopedic shoes with a high, rigid lateral foot and heel support and an orthopedic insole with a mandatory notch in the heel area to keep the hindfoot in a strictly upright position.
Congenital clubfoot
Clubfoot is a congenital musculoskeletal anomaly with a bilateral malalignment of the lower limbs in which the feet are on the outer edge.
The characteristic symptoms of a congenital orthopedic anomaly are:
- Varus deformity of the foot in the newborn, when the sole part is bent downward and inward;
- Supination of the foot, when the sole of the foot is turned inward and the supporting part becomes the tarsal or metatarsal bone;
- Adduction, when the arch of the foot is enlarged and turned inwards in the forefoot area.
The degree of these symptoms varies both upwards and downwards. Sometimes the supination of the child's lower limbs is so pronounced that the inner heel touches the ankle joint, and a pronounced varus deformity pulls the heel up and turns it inward.
In medical theory, congenital bilateral clubfoot is divided into a mild form (osteal sac varus contracture), in which the talar head protrudes with little skin mobility, and a soft-tissue, ligamentous form, in which the skin layer is well developed and not bony Protrusion is present.
Varus deformity of the foot in children with congenital bilateral clubfoot is characterized by an inward displacement of the tibia, which limits the mobility of the ankle joint support system.
The severity of the situation worsens when the child begins to walk. There is thickening of the skin on the outside of the foot, gradual atrophy of the ankle muscles in the calf area, and an X-shaped recurrence of the knee joint.
According to medical experts, varus deformity of the lower limbs in children with bilateral clubfoot has a different cause and effect:
- Contact anastomosis of the amniotic membrane (membrane of the embryo) with the embryo, with gravity pressure of the amniotic membrane on it;
- the girding pressure of the umbilical cord on the lower limbs of the fetus;
- muscular compression of the uterus on the external surface of the fetal foot due to low amniotic fluid;
- compression of uterine tumors;
- Impairment of the spinal innervation of the fetus.
Therapeutic rehabilitation for children in their first year of life
Therapeutic physical training (LFC) for children with congenital clubfoot is indicated from the first days of life against the background of general orthopedic treatment. At the age of 7-10 days, the child's musculoskeletal system is effectively treated.
The comprehensive LFC approach involves the gradual application of corrective casts. A so-called position therapy is carried out, which is reinforced by special massages. After removing the cast, the masseur performs exercises on the foot and lower leg, followed by repositioning with a corrective bandage.
The massage is intended to ensure complete relaxation of the muscles of the foot and lower limbs. For this purpose, stroking, vibration, kneading, muscle diastasis and stretching of the heel tendons are carried out.
After the relaxation massage, muscle tension is released, and the masseur performs the next phase of therapeutic rehabilitation - physical exercises:
- The starting position for the child is lying on his back.. The goal is to eliminate external adduction of the foot. Let's say the masseur is working on the right foot. The ankle is pressed with the left hand, with the first finger on the outer ankle and the second finger on the inner ankle, so that the child's heel rests on the masseur's hand. With the right hand on the foot, with the first toe on the outer edge, the flexed second toe of the massager on the back of the limb, and the third toe on the inside, push the child's foot outward. Do the same with your left foot.
- The starting position is as before. The goal is to eliminate the rotation of the foot in relation to the longitudinal axis. The masseur grasps the child's right foot with his right hand and places the first toe on the sole of the foot and the other toes on the back of the foot. With the other hand, the heel is held. The massage is done by pressing the first toe from bottom to top on the outer edge of the child's limb, while the massage works from top to bottom on the inner edge.
- The starting position does not change. The goal is to eliminate plantar flexion. The masseur's right hand presses the child's left shin against the table, with the first and second fingers resting on the ankle joint. The masseur's left hand presses the sole of the foot upwards with the palm of his hand.
Tips for prevention
The development of varus foot can often be prevented. For this purpose, the following is recommended:
- Wear orthopedic shoes from an early age;
- Teach your child simple exercises and maintain a daily routine;
- Pay attention to the child's diet and make sure the child is getting nutrients with food, or ask the pediatrician about taking a multivitamin;
- Visit your pediatrician regularly for checkups (once or twice a year);
- Give your child vitamin D in fall and winter.
Until the age of 3 years, ensure that the child walks and stands with the correct foot position. Gradually this will emerge and the foot will straighten up automatically.
This diagnosis will not bring quick results. Parents must be patient and follow all the doctor's recommendations. Surgery is indicated in children who have failed conservative treatment. In advanced cases, surgical methods are preferred.
Video

*The information contained herein should not be used for self-diagnosis or to determine treatment and is not a substitute for seeing a doctor!
We live in Kaliningrad, I found it through an ad on Avito
To the neurologist and orthopedist, will give recommendations – massage + shoes + physiotherapy.
I saw a program on TV and you should watch Regina +1 and there the pediatrician talks about feet…. Children up to the age of 5 have shaped feet and there is no reason to force anything to straighten them.
Go to an orthopedist and he will prescribe orthoses, massages and physio. But I think you are still young ))) And don't focus on it, but up to 3-4 years there are. But go, calm your soul.
I don't know, found information on the Internet, how old are you? What did you do?
You look pretty valgus. We're 1.9 now, but we've seen feet like that when we were 10 months old. The orthopedist prescribed electrophoresis, massage, orthopedic mats, walking on stones if possible, sea salt baths and massaging the foot if possible. He didn't say anything about shoes.
I had two massages 8 months ago. Everything was in order.
In our case it was only now diagnosed. So it took you several months for the treatment?
We did it in the 3rd and 6th months. 10 times each.
How did the malformation become noticeable at 3 months? We didn't see it until our daughter started standing on her feet.
She was born, and it was immediately visible in the maternity ward. Until the 3rd month I did it myself, and then professional massage, physiotherapy. So when she was up, everything was fine.
Massage 10 times, once every six months. Physiotherapy. At home, shoes and a massage mat.
How long did it take in the end?
One year, 2 massages and 2 physiotherapies. All at the same time. Massage mat for children - just type it into a search engine, we bought them a long time ago, they cost up to 1000, now they cost 1100 or more. There are different degrees of stiffness. As the orthopedist said, even if you put them at the entrance to the room and forget to move, if you walk a little every day, the effect will be
Read more:- Clubfoot in children therapeutic exercises 7 years old.
- Therapeutic exercises for scoliosis.
- Massage for flat feet.
- Massage for varus deformities of the legs in children.
- Exercises for the triceps tibialis muscle.
- Foot.
- 1 year old child with clubfoot.
- Clubfoot Treatment.