Neuropathic syndrome is damage to the oculomotor nerve, which is part of the sciatic nerve, and can be caused by leg lengthening after hip replacement, compression of the hematoma on the nerve, or, less commonly, intraoperative trauma resulting from surgeon negligence. Restoration of the nerve is achieved either through etiological treatment with optimal surgery, or through motor rehabilitation.

- What are the risks associated with arthroplasty?
- What is arthroplasty?
- Classification of dentures
- Types of hip arthroplasty
- The 5 most important tips for people who have undergone coxarthrosis prosthesis surgery
- 8 taboos for hip replacement patients
- The main risk factors
- Concept and treatment of complications
- Dislocation and subluxation of the endoprosthesis
- infection of the paraprosthesis
- Variability of leg length after an endoprosthesis
- Wrong product size
- risk of thrombosis
- pulmonary embolism
- Performing an endoprosthesis exchange: an algorithm for management
- After the operation: the patient's condition
- When is an operation important?
- When surgery is contraindicated
- Long-term rehabilitation period
- Baths, saunas and hammams
What are the risks associated with arthroplasty?
If the osteoarthritis reaches the third stage, a specialist doctor may come to the following advice: A joint replacement is recommended. A joint replacement is indicated when the joint or parts of the joint are severely damaged, severe pain occurs and mobility is restricted. How is the operation performed, what are the risks and is there an alternative?
Knee and hip replacements are the most commonly performed joint replacement surgeries.
What is arthroplasty?
Arthroplasty is the surgical replacement of a natural joint with a structure made of ceramic, metal or a particularly strong plastic. The sole purpose of an artificial implant is to model and replace a non-functioning joint. If done correctly, the endoprosthesis allows normal movement for 10-20 years.
The following materials are used in joint endoprosthetics
- alloys of stainless steel;
- Special cement - made of acrylic resin, cobalt and chromium alloys - for fixation of the endoprosthesis;
- Titanium alloys - as a basis for the sliding components;
- Super high-strength polyethylene and aluminum oxide ceramics - for the treatment of the sliding surfaces.
Each prosthesis is subjected to a multi-stage test and is certified.
Classification of dentures
classification Types of THR endoprostheses The prostheses are divided into the following categories:
- type of attachment (cemented, uncemented, combined);
- materials used (polymers, titanium, steel, ceramics);
- primary or revised joint replacement.
Joint replacement surgery can only be performed after a thorough review of the patient's entire medical history, selection of an appropriate implant, diagnostic tests and thorough consultation with all doctors involved. Total surgery may be necessary total hip replacement or the replacement of individual parts.
Types of hip arthroplasty

Endoprostheses can be unipolar or total. Unipolar endoprostheses consist of a single component, while total endoprostheses represent the entire artificial joint.
unipolar Unipolar hip prostheses are used for injuries to elderly or debilitated patients. They can be used if the patient does not have significant acetabular changes due to osteoarthritis.
This procedure is not very traumatic, which increases the number of recommendations for its use. Femoral fragment replacement takes less time and there is less blood loss. Unfortunately, the lifespan of a single component is shorter than one total hip replacement. The lifespan of the femoral component is between two and five years, requiring the patient to undergo revision surgery at the end of its lifespan.
In total arthroplasty, the joint is completely replaced with an artificial structure consisting of the femoral head and the acetabulum. These devices last much longer than Unicompartmental endoprostheses.
Artificial joints are divided into type of prosthesis Cemented and uncemented prostheses.

A cemented endoprosthesis (cemented anchorage) used when the bone structure is very porous. A special substance called bone cement is placed in the socket and femoral canal. It increases the degree of fixation of the components and supports them by redistributing the load. The duration and quality of the rehabilitation is hardly affected because different sliding couples can be used.
In young patients with good bone quality, it is best to use the following prostheses Cementless endoprosthesis (cementless fixation). Endoprostheses for cementless anchoring (press-fit) have a special porous coating. Bone grows into the pores of the shell and over time the implant becomes more firmly anchored.
The 5 most important tips for people who have undergone coxarthrosis prosthesis surgery
- Avoid strenuous exercise and even long walks longer than half an hour.
- Do not lift heavy objects.
- Use a backpack to carry things from place to place.
- Do not carry a weight of more than 3 kg in your hands. Better carry it in front of you by pressing it against your chest.
- Don't stand for very long. Always bring a folding chair that you can lean on.
Do not walk or stand much after an endoprosthesis.
8 taboos for hip replacement patients
- deep chairs. These bring the body far from its natural position and carry the risk of complications.
- Slippery surfaces. The likelihood of injury increases many times over.
- deep squat .. Without stabilizing ligaments, muscles may not be able to handle the increased load.
- Sitting diagonally in a chair.. Only natural positions are acceptable - diagonal positions unevenly distribute the load on the body, which is very dangerous.
- Sitting cross-legged. Another challenge for the prosthesis.
- Sharp twists and turns.. Lead to mechanical injuries.
- lifting heavy weights. That must now finally be forgotten.
- Support for a sore leg….. After an arthroplasty, you need to be careful to evenly distribute your body weight. Standing on the affected leg is very dangerous.
A high chair with armrests is the only way to rest after a total knee replacement.
How to rehabilitate yourself after an endoprosthesis at home? Advice from a man who has been living with an endoprosthesis for more than ten years:
The main risk factors
Surgery does not rule out complications, and these can be serious. Especially when mistakes are made in the intraoperative and/or postoperative phase. Even small mistakes during surgery or during rehabilitation increase the likelihood of an unsatisfactory hip prosthesis outcome. There are also risk factors that increase the body's predisposition to postoperative consequences and often cause them:
- old age of the person;
- Serious comorbidities such as diabetes, rheumatoid arthritis, psoriasis, lupus erythematosus;
- Any previous operation on the original joint for the treatment of dysplasia, hip fractures, coxarthrosis (osteosynthesis, osteotomy, etc.);
- Re-endoprosthesis or new hip prosthesis;
- Local inflammatory and purulent diseases in the patient's history.
It should be noted that older people, especially those over the age of 60, are at greater risk of complications after hip replacement surgery. In addition to their underlying disease, older patients have comorbidities that can complicate the course of rehabilitation, e.g. B. a lower resistance to infection. There is less potential for reparative and reconstructive functions, musculoskeletal weakness, signs of osteoporosis and lymphatic insufficiency of the lower limbs.

In older people, recovery is more difficult but also more successful.
Concept and treatment of complications
The symptoms of hip replacement complications are summarized in the table below for better understanding. Early contact with the doctor at the first suspicious symptoms can help prevent the progression of the adverse events and, in some cases, save the implant without revision surgery. The further the disease has progressed, the more difficult the treatment becomes.
Dislocation and subluxation of the endoprosthesis
A dislocation occurs in the first year after the prosthesis is fitted. It is the most common pathologic condition in which the femoral component displaces relative to the acetabular component, resulting in separation of the prosthetic head and acetabular cup. Triggering factors – excessive loading, errors in model selection and implant placement (insertion angle errors), use of a posterior surgical approach, trauma.
Dislocation of the thigh component on the radiograph.
Patients at risk include people with femoral neck fractures, dysplasia, neuromuscular diseases, obesity, joint hypermobility, Ehlers syndrome and patients over 60 years of age. Patients who have had natural hip surgery in the past are also particularly prone to dislocation. A dislocation requires nonoperative or open reduction. If the problem is treated in time, the head of the hip prosthesis can be put back in place under anesthesia. If the problem is chronic, the doctor will recommend a second surgery to put the prosthesis back in place.
infection of the paraprosthesis
The second most common disease is an increase in acute purulent inflammation in the area of the implant. Infectious antigens are introduced intraoperatively through inadequately sterile surgical instruments (rare) or enter the bloodstream from any problematic organ with a pathogen-bacterial environment after the procedure (common). Poor treatment of the wound area or poor healing (in the case of diabetes) also contributes to the development and multiplication of bacteria.
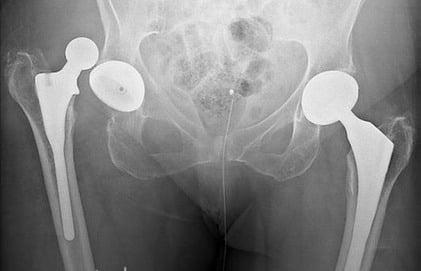
Variability of leg length after an endoprosthesis
Leg length variability after arthroplasty is more common with total hip replacement. Generally, the leg in which the joint has been replaced becomes longer, less often shorter, than the other limb.
- Lack of radiological monitoring during surgery;
- Selection of an implant without prior measurement (offset, RMS). This error is common at knee arthroplasty or hip prostheses with cementless monoblock stems.
In some cases, even with a correctly fitted knee prosthesis, there can be changes in the length of the limbs. … correct adjustment of the knee prosthesis.. A common cause is the lack of quality rehabilitation or carelessness in its implementation.

Measurement of the lateral inclination of the acetabulum. The younger right acetabulum is lower than the left acetabulum, suggesting a leg length discrepancy. Correct horizontal pivot point (red line).
Wrong product size
Today, knee replacements and hip replacements are available in a variety of sizes, shapes, and widths. This allows the surgeon to choose the most appropriate prosthesis for each case.
However, choosing the right size is a serious and responsible process. Mistakes in this process can lead to serious problems:
- A product that is too small can quickly become loose;
- too large a design can lead to broken bones.
Often, a sloppy approach and a negative result are due not so much to the actions of the surgeon as to the limitations of the clinic in question (when a patient is treated with structures that are in stock at the health center so as not to postpone the operation).
risk of thrombosis
After endoprosthesis, there is an increased risk of blood clots in the veins of the lower limbs and pelvis. To minimize the risk of blood clots, special blood-thinning medications are prescribed, which must be taken for a month or two after the operation.
Clots are dangerous because a formed clot can travel to the lungs and cause a pulmonary embolism, which can result in death. Doctors usually teach the patient in the hospital how to recognize symptoms that may indicate a pulmonary embolism so the patient knows what to look for.
pulmonary embolism

As with any major surgery, joint replacement surgery is a significant risk factor for pneumonia, both in and out of the hospital. During your hospital stay, you'll usually be instructed to do regular breathing exercises to reduce the risk of pulmonary congestion and pneumonia.
Performing an endoprosthesis exchange: an algorithm for management
Before the patient is wheeled into the treatment room, the patient is asked to wear a compression stocking on the opposite leg or wrap an elastic bandage around the knee to prevent blood clots.
The patient is then given general or regional anesthesia. In both cases, the patient is medically sedated, but patient feedback on regional anesthesia is more optimistic: it is easier to wake up and the anesthesia remains effective for some time after waking up.
Once the patient has fallen asleep, a catheter is inserted into the bladder.
The entire operation usually takes 1-2 hours. During the operation, the surgeon separates the damaged parts of the joint and puts artificial prostheses in their place. To remove the accumulated blood, a silicone drainage tube is inserted into the wound and a special 'accordion' is used to collect the fluid from the surgical wound.
After all the procedures, the surgeon sews up the incisions, takes care of the wound and applies a special bandage.
After the operation: the patient's condition
After the operation, the patient is transferred to the ward, where he is cared for by a doctor. In the first few days after the operation, he receives antibiotic therapy and anti-inflammatory drugs. On the first day after the operation, the patient is allowed to move in bed, but not very much.
On the second day he is allowed to sit up in bed, do breathing exercises and some physiotherapy exercises.
On the third day, dosed exercises in the form of walking with support (crutches, walking frame or cot) are started.
Within a few days after the prosthesis, the catheter is removed from the bladder. The normal condition after the procedure is swelling of the leg, pain in the groin and in the joint itself, radiating to the limbs. Pain medication may be given to the patient.
Postoperative wound care consists of changing the sterile bandage daily and cleaning the wound surface with aseptic solutions. The sutures can be removed 10-14 days after the procedure. At the same time the patient is discharged from the hospital. The next stage is the rehabilitation process.
When is an operation important?
Hip surgery restores the function of the lower limb – it eliminates the deformity, provides full mobility, allowing the patient to walk, run, lead a normal life and, if desired, play sports.
The connective tissue is destroyed by causal factors and can no longer regenerate. Conservative treatment, however effective, can only slow the progression of the disease and repair cells that have only just begun to break down. If the patient misses a timely chance to be treated with medication and restorative treatments, surgery is always necessary.
Main indications for arthroplasty:
- The most common reason for surgical intervention is osteoarthritis - the disease progresses quickly and is not always treatable with conservative treatment. As the disease progresses, articular cartilage gradually dies and is shed by the body. Patients who have had surgery for osteoarthritis typically have difficulty moving or are unable to walk at all;
- Age-related joint destruction – this problem is more common in old age when there are circulatory disorders. The reduced blood flow slows down the renewal of connective tissue cells and makes the cartilage less elastic, thinner and more susceptible to wear and tear. First of all, the doctor prescribes medication, physiotherapy and exercise, and if this does not help, surgery is performed;
- Trauma – Femoral neck fractures in old age are the most common reason for surgery. In this case, the broken bones either do not heal, or the leg is severely deformed. If the patient can survive the surgery, this is the only way to avoid disability;
- Local inflammation – in advanced stages, some inflammatory diseases contribute to the deformity or ossification of the joint. In these diseases, medication is ineffective and surgery is necessary.
Read more:Danger!!!
When surgery is contraindicated
Hip arthroplasty is a procedure that allows you to return to your normal life, but sometimes this is not possible.
The main contraindications to surgical treatment are.
- inflammation in the joint cavity and surrounding tissues;
- presence of a chronic infection in the body;
- Chronic diseases;
- infectious diseases.
When inflammation is active, surgery cannot be performed effectively—there is an increased risk of complications. Some chronic diseases contribute to immunological disorders that can lead to implant rejection. If there is a chronic nidus of germs in the body, there is a risk that they will enter the bloodstream after surgery and spread throughout the body.
Long-term rehabilitation period
This period begins 3 months after the operation. During this time, exercises to strengthen the musculoskeletal system and bones can be carried out at home so that the prosthesis can be better anchored. The final strengthening of the prosthesis requires everyday exercises, so more gymnastic exercises and the use of machines can be carried out. Physiotherapy is also actively used.
The most popular devices for rehabilitation after endoprosthetics:
- Bicycle simulator - recommended as one of the first devices. Provides the joint with dynamic loads that strengthen the musculoskeletal system;
- Treadmill – Allowed 1-2 weeks post-treadmill workout;
- Special hip extension machine - indicated in the 5th to 6th month of rehabilitation.
Baths, saunas and hammams
Many patients worry about going to the sauna or similar facilities during rehabilitation. Surgery is stressful on the body and the operated area can cause swelling and inflammation of the joint tissues. The body destroys dead tissue so that healthy cells can multiply.
If the temperature rises during this period, the inflammation increases, which can lead to limb amputation. Bathing is allowed no earlier than three months after the operation. It is important that you consult your doctor.
Replacement of an endoprosthesis is a complex procedure that requires a long rehabilitation period. Successful recovery of the leg and its function depends on constant movement and compliance with doctor's recommendations. You can go to the sauna after three months at the earliest.
- How much does a hip prosthesis cost?.
- acetabulum.
- Walking school with prosthesis.
- cost of the prosthetic leg.
- Leg prosthesis below the knee.
- prosthetic legs.
- Life after a leg amputation.
- Modern leg prostheses.