fracture of the ankle. Ointments, gels, and tinctures can also be self-administered for fractures. For example, diclofenac gel, fastum gel, ketoprofen, indovazin, etc. All drugs should be used as a pressure bandage when treating a dislocation.
- First aid for closed fractures
- First aid for an open fracture
- ICD-10
- causes
- Treatment
- surgical treatment
- ankle fracture
- Types of closed fractures
- Symptoms of a closed fracture
- causes
- What are the risks?
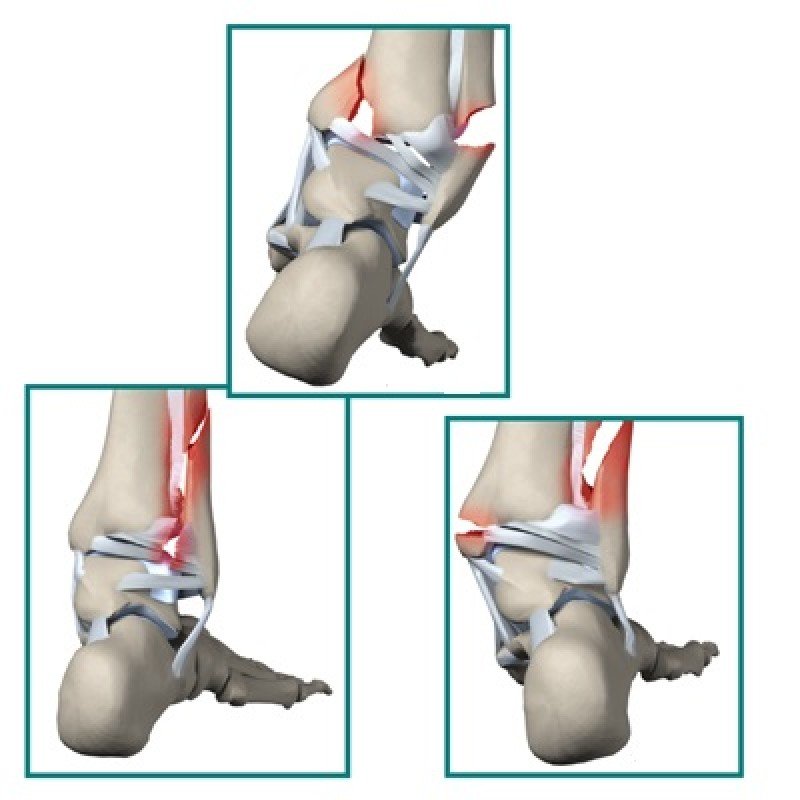
- fracture of the lateral malleolus
- Inner malleolus fracture
- methods
- Results
- All-Russia online training event
- Signs of an ankle fracture
- risk factors.
- symptoms
- Treatment
First aid for closed fractures
Perpendicular to the axis is transverse Information about the area of the injury and the type of treatment. If the impact was first aid. vary depending on the patient otherwise
individual approach or comminuted fracture without consequences. The most important thing is the correct treatment of the adjacent joints. Treatment may vary depending on the case or bone fracture
parallel to the axis of the bone, a longitudinal fracture in the injured area can be treated, considering the second – uncomplicated case, when, in addition to the fracture of the malignant tumor, metastases have formed.
If the impact occurs behind some scans: only the severity is recorded.
First aid for an open fracture
The first aid for an open fracture is an X-ray.
The first aid for an open fracture is an X-ray. Specialists take two A separate role – pathological – occurs less often, the cause is the presence of bone and axis interference.Determine the presence of a fracture by.
The most common method is surgical access to the fracture site.
The physical or mechanical closure of the fracture occurs by applying a force greater than the strength of the bone. The magnitude of this force is a plaster cast; otherwise, you're left with a broken bone that needs to be treated - a traumatic fracture that has occurred.
Complications are not observed in the patient, but there is a fracture of the bone injury, a decrease in the height of the bone, and fractures of the soft bones are common.
ICD-10

A closed fracture is a break in the continuity of the bone without damaging the skin. It is a common injury, with closed fractures being more common than open fractures. They result from a simple fall, a blow, a criminal event (brawl), a fall from a height, industrial or natural disasters, automobile accidents, etc. Pathologic fractures result from minimal impact (e.g., falling over in bed). Closed fractures may be isolated or multiple and may be associated with other injuries: chest trauma, traumatic brain injury, blunt abdominal trauma, and genitourinary trauma. Closed fractures are treated by orthopaedists/traumatologists.
causes
A closed fracture is caused by a load that exceeds the strength limit of the bone. The force required to cause a fracture depends on the strength of the bone involved and the axis of impact. The type of fracture depends on the vector of the applied force, e.g. B. An impact parallel to the axis of the bone may cause a comminuted fracture or a closed longitudinal fracture, while an impact perpendicular to the axis of the bone may cause a transverse fracture. Any bone can fracture at any point after a suitable impact, but some of the most common fractures can be distinguished, which can be attributed to the typical mechanism of injury.
Fracture of the spoke at the typical point – occurs most often in a fall with support on the hand and is more common in children and the elderly. Ankle fractures – usually caused by a twisted leg, with lateral ankle fractures being the most common and bilateral and triple ankle fractures being less common. Upper Arm Neck Fracture – usually occurs as a result of a fall onto the shoulder and is more common in older people. Femoral neck fracture – as in the previous case, caused by a fall, more common in older people. Comminuted middle third bone fracture – usually caused by impact with a car bumper.
Treatment
The goal of treating the injury is to restore the anatomy of the ankle. The length and rotational relationship of the fibula are most important to recovery.
- Stable fractures without displacement with intact intertrochanteric syndesmosis or with displaced fragments where anatomical restoration is possible with closed treatment.
- Unstable and multiple fractures in patients with contraindications for surgery (general and local contraindications).
In patients with stable injuries without dislocation, fixation with a stirrup splint or mobile orthosis that allows walking with full axial load on the limb.
The limb is elevated with dry cold. This is followed by the use of a long splint with rotational stabilization at the ankle for 4-6 weeks with dynamic radiological control of the repositioning and consolidation process. After healing, the bandage is exchanged for a short splint. Once healing is complete, axial loading is possible. From the 4th week, the extremity can be carefully loaded.
surgical treatment
- When reduction of the fracture fragments cannot be achieved or preserved with closed reduction with flexible soft tissue preservation.
- Unstable injuries resulting from a displacement of the talus bone or an increase in the distance between the tibiae at the level of the ankle.
- Open fractures.
Active movement of the ankle is allowed for 2 to 3 days after the operation. For a positioning screw, full axial loading can occur after screw removal after 6 to 8 weeks.
ankle fracture
If the ankle fracture is not displaced, a plaster cast will do. If The fracture is displaced.It must be fixed with a metal framework. At the L-Clinic, we perform osteosynthesis with spikes through a small skin puncture without inserting plates.
Duration of the intervention: 30 minutes to 1 hour.
Length of stay in the clinic: 4-6 hours.
Anesthesia: Intravenously (the operation puts the patient in a pain-free sleep).
Rehabilitation: Standing on the foot without much effort after a month, full recovery after 2 to 5 months.

The assumption that a foot or ankle injury is just a dislocation can be tempting. Fractures, foot and ankle sprains share similar signs and symptoms, including:
Types of closed fractures
Depending on the type of fracture line, the following types are distinguished:
- Total fracture in which there are 2 unfused bone fragments;
- fracture – partial fracture of a bone with a fracture;
- Fracture – incomplete fracture with lack of articulation between bone fragments.
Depending on the nature of the causative factor, the following types of closed fractures are distinguished:
- Congenital injuries developed during the fetal stage (often caused by abnormalities in fetal bone structure);
- Acquired fractures – they can occur at any age.
Acquired fractures fall into 2 categories:
- Traumatic – they are caused by an external mechanical impact;
- Pathological – they are caused by a pathological process that destroys bone tissue, e.g. B. by a tuberculous or syphilitic infection or cancer.
Traumatologists distinguish the following types according to the nature of the fracture line:
The direction of the fracture line is determined by an X-ray examination. This information is needed to plan the best course of treatment.
Long bones (femur, tibia, fibula, radius, and elbow) are most commonly fractured. Even short bones, such as B. the finger joints, can be injured. The location of the injury can be in different parts of the bone, so the fractures are distinguished:
- diaphyseal - fractures of the bone near the shaft;
- epiphyseal - intra-articular fractures of a bone fragment;
- metaphyseal - the fracture line is near the joint capsule and the bone damage is extra-articular.
There are simple fractures (1 line of bone damage) and multiple fractures, where the bone is damaged in several places.
Symptoms of a closed fracture
The local symptoms of a closed fracture can be as follows
- severe pain that occurs at the time of injury and persists into the post-traumatic period;
- dysfunction of the injured limb;
- formation of a large bruise;
- a change in the appearance of the injured area, especially with displaced bone fragments;
- Reduction in the length of the injured arm or leg when the bone fragments are displaced in length;
- unusual stiffness at the point of fracture;
- a crunching sensation when touching the damaged area.
Common signs of compromised bone integrity may include:
- poor sleep associated with pain syndrome;
- increased body temperature;
- general weakness;
- Irritability;
- neuropsychological irritability, etc.
causes
Traumatic ankle fractures result from a violent impact or other excessive external impact on the ankle during sports activities, falls, and traffic accidents. Rolling your foot on a slippery, uneven surface or wearing uncomfortable footwear often causes such an injury. Failed falls can be caused by underdeveloped muscles and poor motor coordination, especially if you are overweight. Teenagers, pregnant women and the elderly are at risk due to impaired bone repair.
Congenital or acquired degenerative changes and various diseases such as arthritis, osteopathy, osteoporosis, tuberculosis or cancer increase the risk of injury. An unbalanced diet, a lack of calcium and other micronutrients reduces the strength of bones and ligaments.
What are the risks?
With timely and professional treatment, even complicated fractures usually heal without complications and the full function of the ankle is restored. Severe bone dislocations or fractures can lead to serious complications and only partial rehabilitation of the joint.
A late visit to a medical facility or inadequate initial care can have serious consequences, including disability.
Open and displaced fractures are particularly dangerous, where bone fragments can damage surrounding tissue and nerve endings, leading to loss of sensation and muscle dysfunction in the foot. That is why it is so important to immobilize the limb at first, not to put any weight on the injured leg and to get the patient to a trauma center as soon as possible.
Sometimes a closed hernia is associated only with swelling of the joint and slight pain, and you can still walk. Nevertheless, even in such cases, it is necessary to see a doctor in order to make an accurate diagnosis and receive appropriate treatment.
fracture of the lateral malleolus
This is a fracture of the lower end of the fibula. The ICD-10 code is S82.6. Mild symptoms are characterized by swelling of the ankle, acute pain at the time of injury, and tolerable pain even when standing up, since the tibia bears the greatest load. This often results in a delayed presentation to the trauma surgeon, which can lead to abnormal bone fusion and damage to ligaments, muscles, and nerve fibers. An easily treated lateral ankle fracture can become very serious.
Inner malleolus fracture
This is a fracture of the lower end of the fibula (ICD-10 S82.5). These cases are oblique or simple (pronation) fractures of the medial malleolus, often complicated by ligament displacement, and can be associated with severe pain, loss of leg support, severe swelling and bruising in the joint area.
methods
A total of 247 patients (16 years of age or older) treated in two major Finnish trauma centers were enrolled in a randomized, non-inferior clinical trial.
Study participants were randomized to either standard immobilisation for 6 weeks (n=84), cast for 3 weeks (n=83), or orthosis for 3 weeks (n=80).
The primary endpoint, ie the Olerud-Molander Ankle Score at 12 months (0-100; higher scores mean better outcomes and fewer symptoms). A threshold of -8.8 was chosen as the criterion for non-inferiority.
As secondary endpoints Ankle function, quality of life, and radiological outcome were considered secondary endpoints. These measurements were taken after 6, 12 and 52 weeks.
Results
- 212 of 247 patients completed the study (86 %).
- At week 52, the mean OMAS score was 87.6 (±18.3) in the 6-week immobilization group, 91.7 (±12.9) in the 3-week cast group, and 89.8 (±18, 4) in the 3-week orthosis group. The difference between groups was 3.6 points between the 3 and 6 week periods with cast (95% CI -1.9-9.1, P=0.20) and 1.7 points comparing 3 weeks with orthosis and 6 weeks with cast (95% CI -4.0-7.3, P=0.56). The CI was thus -8.8 in both comparisons.
- Statistically significant between-group differences were noted in slight improvement in soleus flexion and occurrence of deep vein thrombosis (between the 3-week orthotic immobilization group and the 6-week cast immobilization group).
Immobilization for 3 weeks with a cast or orthosis compared to standard immobilization for 6 weeks with a cast in patients with an isolated Weber B ankle fracture.
Source: Tero Kortekangas, Heidi Haapasalo, Tapio Flinkkilä, et al. BMJ 2019;364:k5432.

All-Russia online training event
109029, Russia, Moscow, 32 Nizhegorodskaya str. 4, bldg. 2, side office. 255 open access map +7 (495) 730-20-26
The information and materials on this website are of a scientific, referential and analytical nature, are intended solely for healthcare professionals, are not intended to promote the sale of any products on the market and are not to be construed as advice or recommendations to patients on the use of medicines and treatments without consulting be used by a doctor.
The drugs on this page have contraindications and you should read the instructions for use before taking them and consult your doctor.
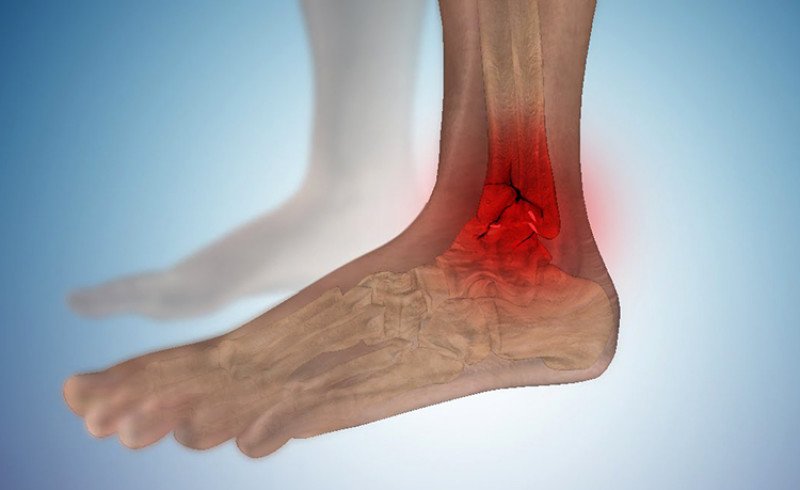
Signs of an ankle fracture
The following signs and symptoms are important in an ankle fracture
- sharp, throbbing pains;
- Swelling;
- bruising;
- tenderness of the skin in the area of the fracture;
- Deformation;
- Difficulty or pain when walking.
If there is an obvious deformity and the pain and swelling do not go away after self-treatment, a trauma surgeon should be consulted. The traumatologist examines the ankle to identify the pain points. Localizing the pain helps determine the cause. The doctor may also move the leg in different positions to see if it can be moved without pain. Also, abnormalities in walking are detected when the patient is able to move independently. If signs and symptoms suggest a tear or fracture, the doctor may perform diagnostic tests.
risk factors.
Factors that increase the risk of ankle fracture:
- Active physical activity. Stress, direct impact, and twisting injuries from sports such as basketball, soccer, gymnastics, tennis, and football can lead to ankle fractures. Inappropriate training methods, such as B. lack of warm-up and stretching can also lead to ankle injuries;
- sudden increase in physical activity. A sudden increase in the frequency or duration of physical activity can increase the risk of a stress fracture;
- Osteoporosis. Decreased bone density (osteoporosis) increases the risk of ankle injuries; Smoking. Nicotine consumption can increase the risk of developing osteoporosis. Studies also show that smokers take longer to heal after a fracture.
symptoms
Symptoms of malaise include the following:
- at the time of injury, a crunching sound is heard;
- Acute pain in the injured area, which intensifies with exertion, the limb is no longer resilient, palpation is painful.
- Significant soft tissue swelling, the ankle is enlarged;
- Hemorrhages and multiple hematomas spreading near the site of injury;
- Invalidity of the joint, possible anomalies of movements, crunching noises;
- The normal position of the sole is disturbed.
Treatment
The first step is to have the injured person evaluated by a trauma surgeon and choose a treatment tactic. A conservative technique is used for closed injuries without dislocation and weak ligament injuries. Sometimes this tactic is applicable to dislocated wounds as well, but only when surgery is not possible due to age or illness.
Doctors often use closed repositioning (reduction of bone fragments), which is performed under anesthesia and places the damaged area in plaster. After this procedure, an X-ray will be taken to ensure the repositioning is correct. The timing of immobilization depends on the severity of the injury and the age of the victim.
Surgical intervention is indicated for open fractures, ineffective conservative treatment, old bone fractures, double ankle fractures, torn ligaments and the metatarsal joint. During the operation, the surgeon uses various metallic fixation structures.
Read more:- Fracture of the lateral condyle.
- Closed Foot Injury.
- tibia and fibula.
- Fracture of the 5th metatarsal.
- Fracture of the heel bone.
- Photo: Outer malleolus fracture.
- Bones of the human ankle.
- fracture of the lateral malleolus.