Based on the diagnostic results of the degree of deviation of the metatarsophalangeal joint of the big toe, the orthopedist selects a suitable solution:

- Percutaneous correction of valgus deformity of the big toe
- The following are the standard operations for the treatment of hallux valgus
- Stages of the pathological process
- Indications for surgery
- Percutaneous correction of hallux valgus
- Clinic automation: fast and cheap!
- Clinic automation: fast and inexpensive!
- classification
- symptoms
- Disease prevention
- Causes of hallux valgus
- Open internal angle osteotomy
- What is grade 2 hallux valgus and how does it manifest itself?
- Consequences of hallux valgus deformity of the toe 1.
- causes
- Scaly osteotomy
- Preparing for surgery
- Indications and contraindications for surgery
- Types of operations for valgus deformities
- Diagnosis of valgus deformity
- Surgical treatment and rehabilitation:
Percutaneous correction of valgus deformity of the big toe
Valgus deformity of the first toe (Hallux valgus) is one of the most common orthopedic diseases. The prevalence in women is 50 % and, according to some authors, up to 80 %. The disease affects quality of life by causing fatigue in the legs, pain when walking, and hammertoe deformity of the remaining toes. Little by little the disease progresses and the 'bones' become larger and larger. But the disease is treatable: minimally invasive operations are carried out in one day at the NAKP clinic.
The following are the standard operations for the treatment of hallux valgus
- Scarf and Austin osteotomy (chevron osteotomy) of the first metatarsal bone;
- Akin osteotomy;
- Hochmann osteotomy;
- Lapidus arthrodesis.
Most commonly, open procedures are performed through large incisions. Osteosynthesis is often used: patients have to use an external immobilization device for a long time. Patients also have to use crutches for 2-3 months.
Disadvantages of most surgical treatments
- Significant trauma;
- large scars due to the large incisions
- need for hospitalization;
- severe postoperative pain;
- high risk of complications;
- High risk of complications; need for general anesthesia;
- inability to walk;
- the need for prolonged immobilization, which impairs blood circulation and leads to muscle wasting;
- lengthy rehabilitation;
- large scars on the leg.

The documents should be sent to [email protected]. The possibility of treatment is checked by the clinic's chief physician.
Stages of the pathological process
The doctor decides whether hallux valgus surgery should be performed. He assesses the curvature of the foot. In the first 2 stages of the disease, conservative treatment is carried out. If correction is no longer possible, surgery is required. There are 4 stages of hallux valgus:
- Stage 1: The angle of deviation of the metatarsophalangeal joint of the big toe is no more than 15 degrees;
- Stage II. Characterized by the presence of a small but palpable thickening. The deviation angle is 15 to 20 degrees;
- Third stage. The foot bone protrudes and becomes inflamed when walking and wearing tight shoes. The deviation of the joint is between 20 and 30 degrees;
- Fourth stage. Characterized by a pain syndrome and the development of complications. The deviation angle of the metatarsophalangeal joint of the big toe is more than 30 degrees.

In the early stages of the disease, surgical intervention for valgus deformity of the first toe is not necessary. In these cases, the problem can be corrected without surgery. If the load on the foot is not reduced, valgus curvature of the foot develops. As the pathology progresses, the big toe increasingly deviates inward, while the ankle deviates outward. As a result, the foot widens. In the later stages of hallux valgus, there is persistent swelling of the hump of the foot. Pain occurs not only when walking, but also when resting.
Indications for surgery
After the diagnosis, the podiatrist will decide whether a valgus foot deformity requires surgery. A curvature of the foot is treated surgically if the joint deviates by more than 20 degrees. A severe valgus foot in an adult will not go away on its own. With grades 3 and 4, it is only a matter of time before surgery is required. Severe curvature of the base of the foot without pain and inflammation is an indication for surgical treatment. If the hallux valgus causes discomfort, surgery for a valgus deformity of the big toe is essential. Before surgical treatment, a series of examinations will be carried out.
There are the following indications for surgery:
- Frequent and severe pain at the base of the big toe;
- Development of inflammation when wearing shoes;
- swelling of the big toe;
- flat feet;
- lack of effect of conservative treatment methods;
- Occurrence of complications.

Before starting treatment, the doctor and patient discuss the advantages and disadvantages of hallux valgus surgery. The patient must understand that the operation will help avoid the dangerous consequences of the deformity. Complications of hallux valgus foot surgery include the formation of ulcers on the surface of the deformed joint tissue, bone infections, and gait disorders.
Percutaneous correction of hallux valgus
Percutaneous hallux valgus correction – is the correction of a valgus deformity of the first toe through mini-incisions and skin punctures under EOP guidance using a special surgical kit and implants.
Protocol name.: Percutaneous correction of hallux valgus
| ICD-10 | |
| code | Designation |
| М 20.0 М 20.1 М 20.2 М 20.3 | |
Date of preparation of the protocol: 2018.
Abbreviations used in the protocol
| CT | – | Computed Tomography |
| ECG | – | electrocardiogram |
| RV | – | Wasserman reaction |
| PTI | – | Prothrombin index |
| HIV | – | Human immunodeficiency virus |
| EOP | – | electro-optical transducer |
User of the log: Surgeons, orthopedic trauma surgeons.
Patient category: Adult.

Clinic automation: fast and cheap!
– 800 RUB / 5500 KZT / 27 BYN – 1 order per month

Clinic automation: fast and inexpensive!
classification
The modern classification of hallux valgus is based on clinical and radiological findings.
Deviation angle of the valgus of the 1st toe:
DIAGNOSIS AND TREATMENT METHODS, APPROACHES AND PROCEDURES
Aim of treatment/intervention:
Correction of toe deformity.
Indications and contraindications for surgery/intervention:
Indications for the operation/procedure:
- presence of toe deformities;
- Pain, discomfort when wearing shoes.
- Decompensated circulatory, respiratory, renal and liver failure
- General blood and urine analysis;
- blood chemistry (total bilirubin, ALT, AST, urea, creatinine, total protein, nitrogen);
- PTI, fibrinogen;
- bleeding time and duration;
- stool for JG, blood for RV;
- HIV and hepatitis blood markers;
- ECG;
- Family doctor's report, dentist's report;
- X-ray images of the feet in two projections;
- plantography;
- CT scan of the feet.
Obligation to comply with safety measures, sanitary and anti-epidemic regulationsThe requirements for safety and health protection: in accordance with the sanitary regulations 'Sanitary and anti-epidemiological requirements for health facilities', approved by Order No. 357 of the Minister of Health of the Republic of Kazakhstan dated May 31, 2017.
Equipment Requirements: According to the Decree of the Minister of Health of the Republic of Kazakhstan dated June 6, 2011 № 352 'On approval of the regulations for the activities of medical organizations providing trauma and orthopedic care'.
Technical equipment:
Special instruments:
- Surgical foot set: mini drill, mini spreader, mini saw and screws;
- EOP.
- Preoperative skin preparation;
- Cleansing enema the evening before and the morning of the operation;
- premedication the evening before and the morning of surgery;
- Perioperative antibiotic prophylaxis 10-15 minutes intravenously during anesthesia or 40-60 minutes before surgery intramuscularly, with repeat injections as needed but not longer than 24-48 hours.
symptoms
The symptoms of the initial stage of valgus are often not taken seriously by the patient. The affected person associates painful sensations in the legs with prolonged strain, physical activity or new, uncomfortable footwear. The excruciating pain subsides with rest. Sometimes patients report that shoes in their usual size are uncomfortable.
Finally, the pain occurs at night. They become constant and painful. After putting pressure on their feet, patients complain of an intense, burning feeling. Sharp, stabbing pain suggests that the medial cutaneous nerve is involved in the pathological process.
If the condition worsens, osteoarthritis of the big toe joint develops. The foot becomes wider, flattens and loses its normal shape. The big toe then 'crawls' onto the neighboring toe. As the disease progresses, a hammertoe-like deformation of the second toe develops. The skin over the protruding nodules is susceptible to injury, abrasions and blistering, which is particularly dangerous if diabetes is present.
The deformation process is characterized by the formation of arthrosis of the first metatarsophalangeal joint, in which healthy synovial cells are replaced by fibrous cells. The external reshaping of the foot makes it impossible to wear shapely shoes, which is a complex due to the obvious cosmetic defect. Complaints of this type are most often brought to trauma surgeons by young patients.
The untreated course of a valgus deformity of the first toe leads to serious complications:
- Osteoarthritis of the big toe joints;
- changes in the knee and hip joints;
- impairment of the gait pattern;
- damage to the spine;
- heel spur;
- bursitis;
- chronic Achilles tendonitis.
The appearance of new symptoms requires additional treatment measures and slows down the rehabilitation process.
Disease prevention
The most important rule for valgus deviation of the first toe is to choose comfortable footwear, minimize pressure on the foot and avoid prolonged contact with the foot. If there is a family history of valgus deformity, a person should:
Surgical treatment of valgus deformity of the first toe is carried out at stage III-IV of pathology, when conservative measures do not produce a positive therapeutic effect. In modern traumatology, more than 300 techniques are available for the correction of hallux valgus deformity of the toe. All surgical techniques are divided into effect groups:
For grade I valgus, correction at the soft tissue level makes sense. During the operation, the tendon of the adductor muscle is severed. This restores the physiological pull of the adductors and adductor muscle.
Operations that combine correction of soft and bony structures produce significant therapeutic and cosmetic results. The doctor removes the bony structures and the subcutaneous mucous membrane of the big toe joint.
Bone level surgery is performed for grade III-IV chalgus valgus. Depending on the type of procedure, a V- or Z-shaped incision is made in the first metatarsal bone. The first toe is then moved to restore the physiological angle between the metatarsals.
Regardless of the surgical technique, the patient undergoes special rehabilitation after the procedure:
- Wearing a cast or orthopedic splint for at least six weeks;
- Proportional load;
- prevalence of elevated position of the operated limb;
- minimizing activity;
- Regular therapeutic exercises;
- Daily self-massage with a tennis ball.
If a patient is diagnosed with grade II, III or IV hallux valgus deviation of the big toe, he is unlikely to do without surgery.
Causes of hallux valgus
Hallux valgus is a mechanical deformity caused by wearing uncomfortable shoes and overloading the forefoot (through sports, dancing). Hallux valgus is also caused by ligament weakness, which can be hereditary.
The operation returns the metatarsal bones to their normal position. Fixing the position with spokes makes it possible to walk the next day. The spokes are removed after 30 days.
Open internal angle osteotomy
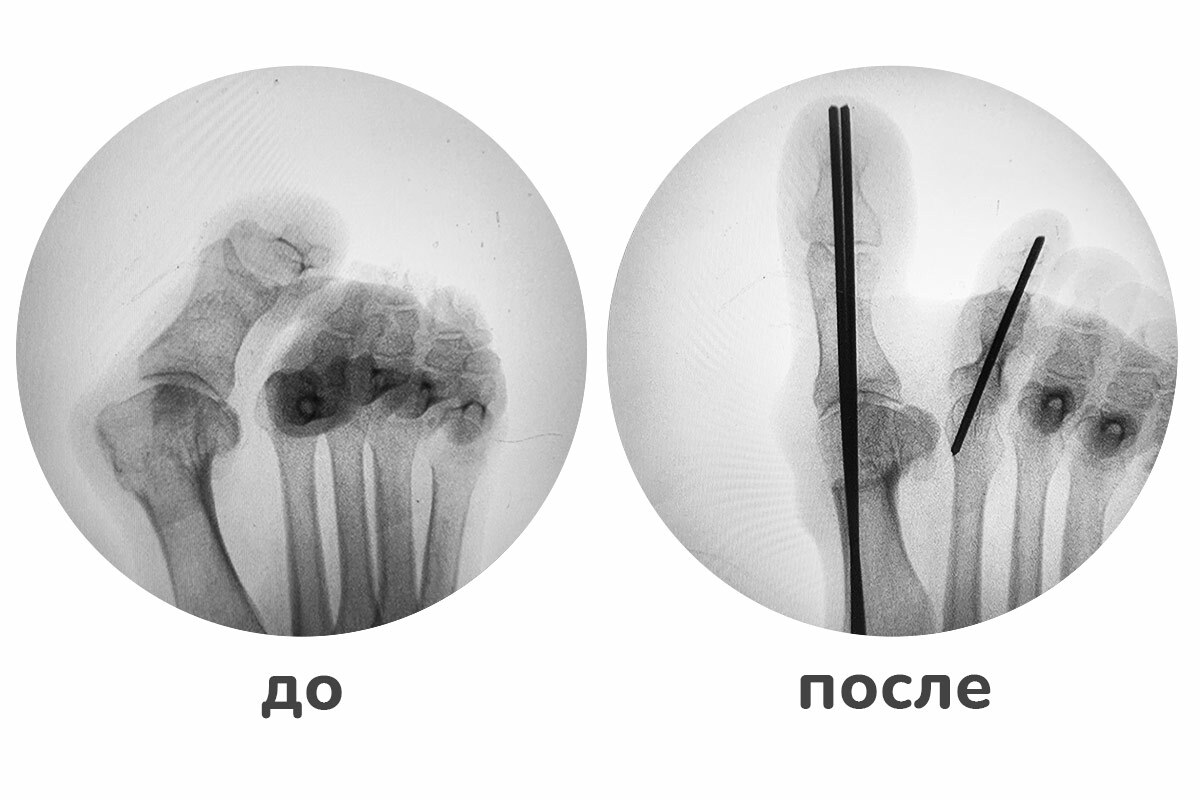
The spoke fixation – is a trauma-sparing method that, in contrast to plate fixation, does not require large incisions during insertion. Additionally, the pins can be removed on an outpatient basis under local anesthesia and do not require any incisions or major surgery.
What is grade 2 hallux valgus and how does it manifest itself?
- Pain in the foot that increases after prolonged walking or physical activity;
- swelling of the foot;
- a small bulge on the side of the foot that tends to become red and painful when wearing shoes with a narrow toe;
- fatigue of the feet;
- Thickening of the skin on the sole of the foot, formation of corns and calluses.
In patients with grade 2 hallux valgus, it is not uncommon for shoes that were until recently comfortable to become tight, rigid, and uncomfortable.
Consequences of hallux valgus deformity of the toe 1.
A valgus deformity of the thumb significantly increases the risk of bursitis of the metatarsophalangeal joint of the big toe. In this disease, the joint capsule becomes inflamed, causing severe pain, redness and swelling of the soft tissues in its protrusion. This can be complicated by synovitis of the same joint, an inflammatory process in the synovial membrane.
If the disease is not diagnosed and treated while it is still in stage 2, it will inevitably progress. An increase in the interdigital angle and the angle of the thumb inevitably leads to an increase in the size of the nodule, where a callus then forms. This leads to significant difficulties in choosing footwear and also causes significant pain. In addition, the outwardly extended big toe deforms the neighboring toes by overlapping them, which provokes the development of the so-called hammertoe deformity. This in turn leads to osteoarthritis of the 2nd and 3rd metatarsophalangeal joints and, as a result, to metatarsalgia (pain) in its projection onto the sole of the foot. The worsening of the deformity over time affects the patient's mobility as it affects the support function of the foot and causes great difficulty in walking.
causes

Hallux valgus grade 2 is a result of untreated valgus deformities of the first toe. Women are most at risk because they tend to wear tight, uncomfortable high-heeled shoes. In addition, physiological hormonal changes in the female body negatively affect the strength of ligaments and tendons, which creates additional evidence of deviations from the correct position of the metatarsals and big toe.
The development of a hallux valgus can also provoke:
- connective tissue abnormalities;
- Transverse and combined flat feet;
- Inflammatory diseases of the metatarsophalangeal joints of the big toes;
- Obesity;
- Pregnancy.
Heredity plays an important role in the development of the disease. Therefore, people who have relatives with a similar deformity should be especially careful and monitor the condition of their feet.
Scaly osteotomy
One of the most popular first metatarsal osteotomies, the gold standard in the treatment of moderate to severe forms of hallux valgus. It was first proposed by Doctor Mayer in 1926, but the operation became popular much later and has been actively used since the 1970s. It was introduced in Russia in the 2000s. The term SCARF translates as 'Arrow of Jupiter' and has its roots in architecture and carpentry.

This technique was used by carpenters to join boards together by making Z-shaped cuts to ensure they overlap securely. This type of sawing is also used in foot surgery. The advantage of this technique is that the bone fragments can be positioned in three planes, giving surgeons a wide range of options to model the anatomy of the foot.
The operation begins with a linear skin incision on the medial side of the foot at the projection of the head of the first metatarsal and the first metatarsophalangeal joint. metatarsal bone. A micromill is used to make a Z-shaped cut on the metatarsal bone and the head of the bone is rotated at the correct angle to place it in the correct position. The bone fragments are fixed in their new position using titanium screws. Finally, the protruding appendage is removed. In complex cases, SCARF is combined with other techniques.
Preparing for surgery
Patients must undergo instrumental diagnosis to determine the severity of the deformity and the extent of surgery. Standard preoperative preparation includes:
- general, biochemical blood analysis;
- a coagulation picture;
- testing for HIV, hepatitis and syphilis;
- Determination of blood group and Rh factor;
- urine test;
- ECG;
- chest x-ray;
- Consultation with a general practitioner.
Hallux valgus surgery can be performed under general anesthesia or under general anesthesia. The type of anesthesia is determined individually after consultation with the anesthesiologist, taking into account the extent of the surgical intervention and the patient's state of health.
Indications and contraindications for surgery
Surgery to correct valgus deformity is indicated for the following symptoms:
Surgery is not performed for rheumatoid arthritis, diabetic foot, obliterating atherosclerosis, purulent infections and hematopoietic abnormalities.
Types of operations for valgus deformities
To correct valgus deformities of the foot, two types of operations are performed - minimally invasive and reconstructive. The former are effective in the early stages and in exostoses. During minimally invasive procedures, 2-3 punctures with a diameter of 3-4 mm are made around the joint.
The more traumatic and invasive reconstructive surgeries cause changes in the position of the foot bones and are performed for severe valgus deformities. The procedures are carried out through a 2-4 cm long incision on the inside of the foot. The doctor restores the first metatarsophalangeal joint to the anatomically correct position and returns the metatarsal bone to its normal position.
Depending on the area of intervention, a distinction is made between soft tissue manipulation, bone manipulation and combined manipulation. The former is indicated for hallux valgus grade I when the head of the metatarsal bone has not yet formed. The doctor works on the tendons, muscles and the joint capsule. For grade II-III disorders, an osteotomy or undercutting of the bone is required. For severe hallux valgus with changes in normal foot function, combined procedures are recommended, combining excision of bone outgrowths and ligament plication.
The osteotomy of the foot is performed under general anesthesia.
The operation can be performed using different methods:
- In the Akin osteotomy, a wedge-shaped incision is made near the metatarsal phalanx of the big toe and the metatarsal bone;
- The Scarfe osteotomy is performed with a Z-shaped incision on the bone;
- The V-shaped chevron osteotomy creates an artificial fracture by cutting out excess fragments and then placing the bone fragments side by side and fixing them;
- Evans calcaneal lengthening osteotomy with implantation corrects flat feet;
- During the Weil operation, the head of the first metatarsal bone is shortened and raised.
The appropriate surgical procedure is determined after a comprehensive examination based on the patient's medical history, the degree of valgus foot deformity and individual contraindications.
Diagnosis of valgus deformity
Due to the obvious external signs of the problem, the initial diagnosis is not difficult; however, it needs to be refined to determine the degree of deformity:
- The x-ray of the foot, which is carried out in two projections, provides information about changes in the structure of the foot and the condition of the bone and cartilage tissue.
- Ultrasound – an ultrasound examination of the bone, cartilage and soft tissues of the foot, during which pathological changes can be detected to make an accurate diagnosis.
X-rays are often sufficient, but the orthopedist orders selective or holistic examinations depending on the individual characteristics and the overall clinical picture of the disease.
Surgical treatment and rehabilitation:
The method of surgical treatment is selected by the attending physician individually for each patient. The operation takes 40-50 minutes on one foot and 80-100 minutes on two feet.
The hospital stay is short and patients are discharged home the day after surgery. Modern methods of halux valgus surgery do not require immobilization in a cast or additional support in the form of crutches or canes. Walking is allowed from the day after the operation in special orthopedic shoes, which must be worn for six weeks. The doctor's instructions must be strictly followed throughout the entire recovery period.
After the operation, the foot is fully resilient again and looks good.
Read more:- ICD 10 chalgus valgus.
- Stages of hallux valgus.
- flatfoot μb.
- First metatarsophalangeal joint of the foot (metatarsophalangeal joint).
- Deflection of the first toe.
- flatfoot.
- Metatarsophalangeal joint of toe 1.
- metatarsophalangeal joint.