Micrographic surgery according to Mohs may be recommended in patients at high risk of recurrence.

- Annular erythema
- symptoms
- Joints of the lower edge of the limb
- The joints of the lower limbs of the free leg
- Is an MRI scan of the foot performed?
- Indications and contraindications for MRI examination of the foot
- symptoms of calcification
- diagnosis
- How can foot swelling be relieved?
- Prevention against swollen feet
- diagnosis
- Treatment of plantar fasciitis
- indications
- Principle of pharmacological action.
- basal cell carcinoma of the skin
- signs and symptoms
- squamous cell carcinoma
- symptoms and signs
- diagnostic methods
- Distinction
Annular erythema
Ringer's erythema is an erythematous skin lesion with ring-shaped patches and rashes. The skin color changes to red, light pink, or bluish. Depending on the underlying disease, swelling, localized fever and other symptoms may occur. The discoloration of the skin is caused by a widening of the lumen of the capillaries penetrating the connective tissue and the associated congestion of blood.
There are different types of erythema annulare, depending on the cause of the condition:
- Erythema migrans (erythema darius centrifugalis) – mostly affects middle-aged men, less often children and the elderly and is classified as an infectious-allergic phenomenon;
- Erythema migrans (transmissible erythema migrans) – an infectious disease caused by the bite of a tick infected with the Borrelia bacterium;
- Erythema rheumatica or erythema annulare, one of the symptoms associated with rheumatic fever that is common in children and adolescents.
Ring-shaped erythema can present as follows:
- in the exfoliative form – with scaling of dead skin at the edges or on the entire surface of the spots;
- in the vesicular form – with small fluid-filled vesicles that appear on the edges or on the entire surface of the spots
- the garland form, with the mildest course, characterized by pale pink spots that appear in chains or garlands and disappear after a few days;
- the microhirlitic form with small spots up to 1 cm in diameter, sometimes accompanied by scaling or blistering, and has a long course.
Other, very rare forms of erythema annulare, e.g. B. the telangiectatic erythema, the purple erythema or the erythema thickens, are mentioned in the medical literature.
symptoms

The main symptom of the disease is a characteristic skin erythema in the form of irregular rings with a light border that stands out against the surface of the skin. In erythema centrifugale dardieri, these rings usually appear on the skin that is usually covered by clothing—on the back, abdomen, chest, and forearms. Erythema dardieri after a mosquito bite is a single spot that spreads from the site of infection and in its final form can reach 20-25 cm in diameter. The spots may be accompanied by itching or burning. With the rheumatic form of the pathology, there are no complaints.
Only a doctor can accurately diagnose the disease. Don't delay in your consultation - call +7 (495) 775-73-60
Joints of the lower edge of the limb
In this part of the human body there are two symmetrically located sacroiliac joints and one semi-recumbent joint - the pubic symphysis, which is also often referred to as the pubic symphysis.

The pubic symphysis is a semi-flexible junction of the upper branches of the pubic bones of the pelvis, which is a disc of fibrocartilage. Their front surface is 3-5 mm wider than the back surface.
Some people have a slit in the pubic conjunctiva that is filled with avascular fluid. The bone tissue is covered by hyaline cartilage at the contact surfaces with the intervertebral disc.
In memory of. In men, the longissimus joint is the attachment point of the ligament on which the penis is suspended. In women, a special hormone called elastin is produced during pregnancy, which allows the pubic symphysis to move more freely, allowing for the birth process.
As the name suggests, the sacroiliac joint is located where the sacrum meets the hip bone in the pelvis. At their points of contact, the so-called articular surfaces, the bone tissue is covered with fibrous cartilage.
These two joints are flat in shape and there is no movement.
The joints of the lower limbs of the free leg
The human leg consists of 3 parts - the hip, the lower leg and the foot. Your mobility is ensured by the hip, knee and ankle joints.
It is also worth noting that the joints of the lower limbs are especially strong and heavily loaded. The knee is one of the most commonly injured joints.
This is due to its 'imperfect' geometry, which nature has equipped with stabilizing ligaments, tendons and meniscus. Damage to these makes the knee the 'problem leader' of all parts of the leg.
Is an MRI scan of the foot performed?
There are two types of MRI scanners: open and closed. In the former, the magnet is at the top and bottom, while in the latter, the perimeter is within the overall gentrification ring. A closed CT scanner provides better quality images than an open device due to the higher field strength directed towards the anatomical area to be examined. The Medical Center 'Magnes' has a 1.5 Tesla CT scanner from Siemens, made in Germany, which differs from its analogue devices in its high performance and the clarity of the results obtained. A number of special functions allow the procedure characteristics to be set for each individual patient.
Indications and contraindications for MRI examination of the foot
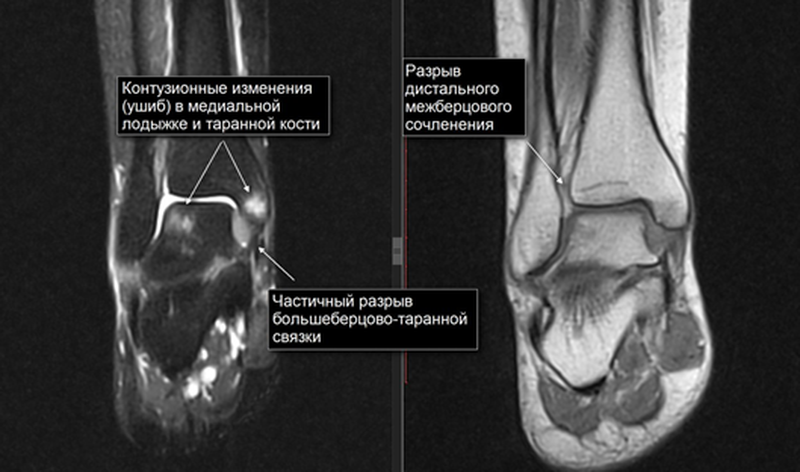
This method is used by doctors to confirm the initial diagnosis and clarify the condition of structures when planning surgical interventions. The specialist decides on the need for a non-invasive instrumental foot examination based on the following complaints of the patient:
- Pain (acute or chronic) in the distal part of the lower extremity that does not respond to treatment for a long time;
- external signs of an inflammatory reaction in the form of discoloration of the skin, swelling, deformation or enlargement of the foot
- Restriction or inability to move
- Discomfort in the form of tingling, grinding or numbness of the foot;
- undifferentiated or ambiguous lesions that need to be clarified by other investigations;
- circulatory disorders of the foot;
- Presence of neoplastic processes of a primary or secondary nature, clearly visible on visual inspection, palpation, etc.
MRI is a painless and completely safe procedure that has no adverse effects on the human body. Contraindications include:
- Pregnancy – the direct impact on the fetus during the examination is not fully understood, so experts do not recommend performing manipulations, especially at the beginning of pregnancy (first trimester);
- the presence of metal plates (except titanium), prostheses, pins, hemostats in the body can be an obstacle to the examination – the above items reduce the significance of the images and, due to their interaction with the magnetic field, can cause undesirable effects;
- Cardiostimulators and neurostimulators installed in the body are a reason to refuse the procedure, since they are affected by the operation of the device;
- Claustrophobia – You can have a panic attack because you are afraid of closed spaces. You should talk to your doctor about how to manage this. A sedative may be prescribed prior to the examination.
symptoms of calcification
In the early stages, it is very difficult to diagnose as there are no symptoms. However, some species have a clear clinical picture.
In the systemic form of calcification, ie when the skin and joints are affected, the epidermis is covered with small vesicles and there is no change in texture or color. With the progression of the pathology, the calcium conglomerates swell, become denser to the touch and change color. Fistula formation is possible.
Calcium deposits can be found during a routine examination by a specialist or an instrumental examination on teeth, bones, vessels, muscle and nerve fibers. Accumulation of the macronutrient on organ tissues leads to impairment of organ function.
When the heart muscle and vascular system are damaged, the patient feels pain in the sternum, arm, neck, and back that lasts for a long time. Blood flow is also impaired, leading to an increase in blood pressure and a feeling of coldness in the limbs.
If the kidneys are damaged, the symptoms of poisoning increase, urine output is impaired and the skin becomes dry and flabby. When the gastrointestinal tract becomes calcified, the gastrointestinal tract becomes compromised, resulting in nausea, vomiting, abdominal heaviness, and constipation.
When the brain is damaged and large amounts of calcium accumulate, frequent headaches and dizziness, increased intracranial pressure, impaired coordination, impaired memory, vision and hearing problems occur. As the disease progresses, fainting may occur.
At the same time, calcinosis leads to poor performance, permanent dementia and fatigue, weakness and weight loss.
diagnosis
X-rays are taken to confirm the diagnosis. With their help, it is possible to determine the type and size of the deposit, as well as the extent of damage to the organ in which the calcareous conglomerate is located. Doppler ultrasound is recommended as an additional examination method:
- Doppler ultrasound to study the condition of the vascular system;
- ECG to study the heart muscle;
- CT examination with administration of contrast agent;
- MRI.
To determine the cause of tissue calcification, additional examinations are ordered in the form of general clinical and biochemical blood tests. With the latter, the calcium, phosphorus and magnesium levels in the blood can be determined. With impaired renal function, a general clinical and bacteriological examination of urine is ordered to assess renal function.
A tissue biopsy is ordered to rule out a malignant tumor in the affected organ. With this method, biological material is removed and examined under a microscope under laboratory conditions. The biopsy also helps differentiate between benign and malignant tumors.
How can foot swelling be relieved?
Treatment varies depending on the cause of the swelling. Diuretics, a special diet, and compression clothing are likely to be prescribed to relieve symptoms. If you have an internal organ condition, follow your doctor's advice and the uncomfortable symptoms will go away with the disease.
To get rid of temporary swelling or relieve symptoms before treatment, you can take a contrast shower, lie down with your feet slightly elevated and a pillow underneath, and gently massage your feet upwards.
Prevention against swollen feet
If you are in good health but your feet are still swollen, you may need to make some lifestyle changes. First of all, you should limit the consumption of salty and spicy foods, as these bind liquid. Be mindful of how much water you're drinking - the average person shouldn't be drinking more than 2.5 liters a day.
Take regular short breaks and stretch tired legs if you work sitting or standing. Try not to wear high heels all day and pay attention to your sitting position: you shouldn't be sitting backwards and the edges of the chair shouldn't press on your thighs.
If all of these measures to reduce swelling don't help, don't put off seeing a doctor. Even if you don't have a health problem, a qualified medical specialist can help you find a remedy for your uncomfortable symptoms, and your life will become more comfortable.
diagnosis
In most cases, the diagnosis is based on a clinical examination of the patient, that is, on subjective and objective symptoms.
Less often, instrumental diagnosis is required. It is needed when the diagnosis is difficult to make or when the doctor needs to differentiate plantar fasciitis from other diseases.
The aponeurosis can be visualized by ultrasound or MRI. The main symptom is a thickening of the plantar tendon, which is usually 2-4 mm and 6-10 mm in heel spurs. Ultrasound and MRI are also used to rule out other diseases that cause heel pain.
Treatment of plantar fasciitis
In most cases, the treatment of plantar fasciitis is conservative. The following techniques are used:
Modification of physical activity. A reduction in physical activity leads to a reduction in pain within 6 months, even without treatment.
NSAIDS. Medicines with analgesic effect. They help with pain relief, but have no effect on the long-term prognosis.
Therapeutic exercises (LFK). The exercises serve to stretch the plantar fascia. They eliminate functional risk factors for a heel spur, such as B. short foot muscle weakness and Achilles tendon overload. The patient crouches, braces himself against a wall, and climbs up and down stairs, placing only the front foot on the step.
footwear. A firm sole of at least 5 mm thickness and a 2-3 cm high heel are required. Changing footwear is particularly important for patients who are on their feet for long periods of time. Tight, worn, oversized, or uncomfortable shoes make plantar fasciitis symptoms worse.
insole. Only custom-made insoles, not factory-made ones, are effective. Insoles include foot pads. They support the longitudinal arch of the foot by stretching the plantar fascia. This is a pathogenetic process that reduces tension at the heel bone insertion site. Orthotics are more effective than heel soles. They not only reduce the symptoms, but also contribute to the patient's recovery (the aponeurosis gradually builds up again).
Kinesio taping. A tape (self-adhesive rubber band) is placed on the foot to reduce arch mobility and lengthen the fascia in the second phase of the stride (when the foot rolls off). This method is effective, but uncomfortable for the patient, and the bandage needs to be changed regularly. It is therefore mainly used as a temporary measure: to improve symptoms while waiting for the insoles.
indications
Ibuprofen belongs to the group of nonsteroidal anti-inflammatory drugs (NSAIDs): derivatives of phenylpropionic acid. In the instructions for use of tablets and capsules for adults, there are mainly indications for the symptomatic treatment of joint or spinal diseases (rheumatoid arthritis, osteoarthritis, synovitis, radiculitis), pain control in trauma, myalgia and neuritis. The forms for children include the following indications: sore throat, otitis media pain, teething pain, fever associated with acute respiratory infections or influenza, alleviation of febrile symptoms associated with childhood infections, and post-vaccination reactions.
Of course, the indications are not limited to those mentioned above. The following are the most common conditions where ibuprofen reduces inflammation and pain:
- Musculoskeletal disorders, pain relief: ankylosing spondylitis, radiculitis, spinal osteochondrosis, exacerbation of gout, polyarthritis, psoriatic arthritis, tendinitis, soft tissue inflammation in trauma, back pain, joint pain, trauma, sprains, dislocations, various types of myalgia.
- Peripheral nervous system disorders: neuralgia and neuritis.
- Gynecology: primary dysmenorrhea, secondary dysmenorrhea, pain associated with painful menstruation, with inflammation of the appendages.
- Analgesic effect in various types of pain: toothache, headache, migraine, sore throat, earache in otitis media, muscle pain.
- Use as an antipyretic for fever, flu, SARS and colds. Fever in infectious and inflammatory diseases.
- Relief after vaccinations, also against corona viruses.
Principle of pharmacological action.
Ibuprofen belongs to the group of nonsteroidal anti-inflammatory drugs (NSAIDs), which are derivatives of phenylpropionic acid.
Four dosage forms are available in the pharmacy:
- If there are no gastrointestinal contraindications, tablets or capsules are usually chosen.
- In case of acute problems with the stomach or if for some reason the patient cannot swallow pills, suppositories are prescribed.
- Young children are prescribed syrups. Most pediatricians prefer ibuprofen to acetaminophen for fever because ibuprofen works faster and longer and has a lower safety profile because it contains no toxic metabolites.
- An ointment is ideal for joint, muscle and back pain and injuries.
basal cell carcinoma of the skin
basalioma – is the most common but also the safest form of skin cancer. Death from basaliosis is possible only in very advanced cases or in aggressive (basosquamous) forms of the tumor. The favorable course of basaliosis is due to the fact that it almost never metastasizes (only 0.5 percent of cases).
signs and symptoms
Basal cell carcinoma occurs most frequently on the skin of the nose, slightly less frequently on the face and much less frequently on other parts of the body.
The highest incidence is over 40 years of age. The youngest patient to be histologically diagnosed with basal cell carcinoma was 39 years old.
What basal cell carcinoma of the skin looks like depends on its shape:
- nodular form (equivalent to 'knotty). The tumor appears as a nodule. It is distinguished from other skin growths by an increased number of vessels on the surface, a waxy sheen, and small bluish-gray inclusions. All these signs can be seen in the photo.

Another characteristic feature can also appear on the surface of a nodular basal cell carcinoma: the ulceration.

- Superficial shape The basalioma usually appears as a reddened area on the skin. Elements of flaking and the already mentioned waxy sheen are also possible.

- The scleroderma-like form is very rare and often difficult to diagnose. It is characterized by a lighter and firmer thickening compared to the surrounding skin.

squamous cell carcinoma
Occurs less frequently than basal cell carcinoma, is the second most common skin cancer and has a somewhat less favorable prognosis. However, it should be noted that the course of the disease clearly less malignant than that of melanoma.
Metastases are relatively rare, with an average of 16 % cases (1). Patients with cutaneous squamous cell carcinoma less than 2 cm in size have a 5-year survival rate of about 90 %; for larger tumors and overgrowths, the survival rate is less than 50 % (1).
It can appear on any part of the body, including the genitals and mucous membranes, but is most common in sun-exposed areas.
symptoms and signs
What cutaneous squamous cell carcinoma looks like largely depends on the clinical form of the disease.
keratotic form – A raised or flat surface covered with horn-like scales that can accumulate and fall off. May bleed from wounds.

Cutaneous squamous cell carcinoma in the keratinized form
It is important to note that under the mask of skin horns a keratinized form of squamous cell carcinoma may be present. Therefore, such growths should always be removed only with a histological examination:

The horn of the skin must be removed and examined histologically - under its mask a horny squamous cell carcinoma may be hidden.
Endophytic form 'non-horny' (grows into surrounding tissue). It usually looks like a long-standing sore or ulceration that can deepen and widen over time.

diagnostic methods
Instrumental radiological diagnostic methods are used to detect pathology:
The aim of the examinations carried out is to determine the exact location of the pathological focus and its structural analysis.
All methods are important to distinguish enostosis from benign or malignant tumors, which require different therapeutic measures.
Let's take a closer look at some of the diagnostic indicators of enostosis.
'Bone islands' appear on the radiograph as a homogeneous darkening of areas of bone, the contours of which are clear and irregular.
They should not be present in the image received:
- bone dislocations;
- periosteal reaction;
- Thinned, damaged periosteum;
- Periperiosteal tissue structure reaction of the bony epiphyseal soft tissue structures;
- Accumulation of contrast medium.
The pathology usually has a single nidus, but multiple nidus may be present in osteoporosis or congenital diseases.
Computed tomography (CT) shows a density of 600-1500 units on the Hounsfield scale.
This method is more meaningful than the previous one. With it, the tissue structures can be distinguished based on their liquid content.
An enostosis is shown by the following features:
- Homogeneous hypointense signal in all programs;
- Clear outer contours;
- absence of periorbital edema;
- absence of bone marrow sclerosis;
- Absence of contrast medium when an intravenous contrast medium is administered.
MRI can distinguish enostoses from bone pathologies such as osteogenic sarcoma, osteoblastic metastases, and osteoid osteomas.

Distinction
Differentiation of pathology is extremely important. Enostosis is usually manifested by pathognomonic symptoms. Significant lesions often cause problems in the differential diagnosis, requiring further investigation.
The importance of differentiation increases considering that some malignancies share symptoms similar to enostosis.
Let's take a closer look at the question of differential diagnosis.
In most cases, the localizations of this pathology are the same:
In very rare cases, the pathological focus can arise in the short and long bones.
The lesion is based on bony tissue structures of different degrees of maturity.
The biggest problem in the differential diagnosis is the localization of the ossifications in the jawbone.
In most cases, the pathology is discovered accidentally during radiological examinations due to trauma, sinusitis and other diseases.
Table 1 provides examples of the differences and similarities between osteoma and enostome.
The vast majority of flat bones (skull base, scapula, paranasal sinuses)
Long tubular bones, ribs, spines
Read more:- Outer malleolus of the right tibia.
- foot pattern.
- Description of the human foot bone.
- Front lower leg area.
- hole in the heel.
- Rubbing the heel.
- What to do if the sneakers pinch in the heel?.
- The bones of the human heel.