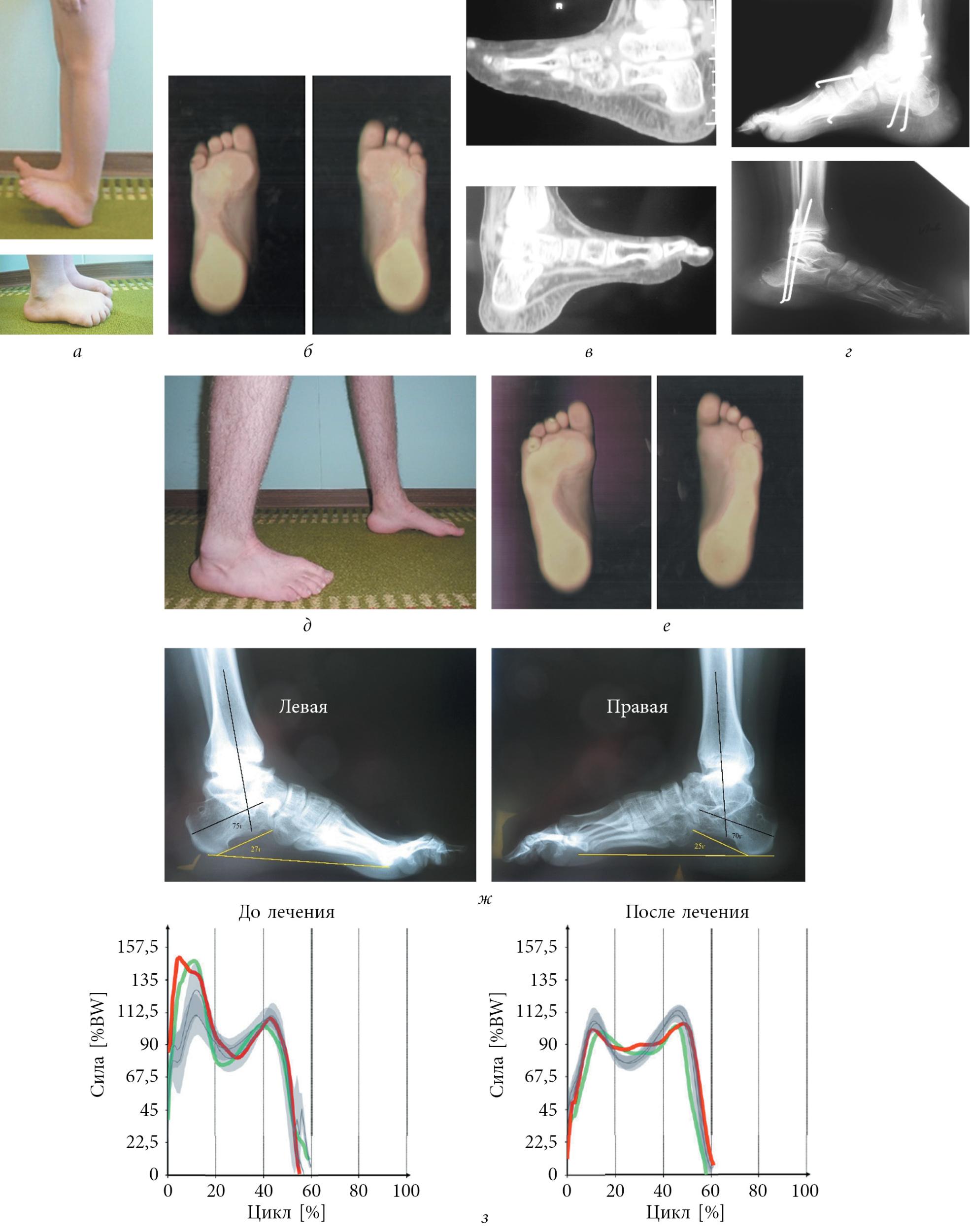
The tactics of surgical treatment depended on the rigidity of the deformity, the age of the child and the degree of muscle dysfunction in the lower leg. Severe trophic disorders of the soft tissues of the foot and the lower third of the tibia were contraindications to surgical correction. A single-stage surgical correction without prior use of a brace was performed when passive correction of the extensor contracture of the ankle to midfoot position without obvious soft tissue tension in the absence of circulatory disorders (skin pallor on the hindfoot surface and capillary reaction) and without the formation of rigid valgus deformity of the hallux valgus due to the tension the shortened extensor tendons was possible. For rigid deformities in which skin deficits on the dorsal surface with signs of circulatory disorders and/or the formation of a rigid toe rolling deformity were noted when attempting to lengthen the foot, a premedial correction was performed with the foot in the equine position to gradually tighten the tendons and soft tissues to stretch. In children under 12 years of age, heel foot deformity was corrected by releasing the soft tissues of the ankle joints (11 feet), taking into account the function of the growth plates. The release resulted in dissection of the joint capsules of the ankle, subtalar joint, scaphoid, and sphenoid. Foot unloading made it possible to correct the heel deformity of the foot with the following radiometric indices: heel-shin angle 30-50°, Meary angle 20-35°, talocrural sagittal angle 30-50°.
Heel deformities in children and methods of surgical correction

Introduction. Heel deformity is a rare pathology in children caused by damage to the long flexor tendons of the foot as a result of various diseases of the nervous system. The choice of surgical correction method depends on the patient's age, the parameters of neuromuscular anomalies and the degree of foot deformity.
objective. – Analysis of the results of surgical correction of heel deformities in children in our center.
Material and methods. The surgical treatment of 13 patients (21 feet) aged 1.5 to 15 years with heel deformities of the foot was analyzed. The differentiated approach and surgical treatment methods were described. In children up to 12 years of age, joint unloading of the foot with elimination of the deformity and tendon-muscle transposition with transfer of the functionally preserved muscles to the site of the prolapsed antagonist muscles were performed. In children over 12 years of age, operations on the ankle apparatus of the foot were performed: triceps arthrodesis or corrective osteotomies of the heel bone, supplemented by tendon-muscle transpositions.
Results. Treatment outcomes were assessed using radiometric parameters and AOFAS scores. An improvement in foot support by reducing deformity was noted in all treated patients. The mean AOFAS score increased from 42.42 to 91.14.
Conclusions. Consideration of all causes and components of the deformity and a differentiated approach enable long-term elimination of heel foot despite persistent neuromuscular conductivity disorders.
keywords
heel foot (Pes calcaneus) belongs to the severe forms of foot deformity and is characterized by the presence of a fixed position of foot extension in the absence of active flexion. The development of this deformity in most cases is caused by damage to the long flexors of the foot, especially the calf muscle, as a result of various diseases of the nervous system. According to the literature, paralytic heel deformity develops in 5-30 % of cases of neurogenic foot deformities in children [1]. It occurs most frequently in congenital spinal hernias in 15-30 % [1, 2], in cerebral palsy in 6 % [1] and in myelodysplasia in 1 % [1]. Cases of heel foot deformity due to secondary deformities have also been described, e.g. B. after treatment of a club foot (10 %) [3] and traumatic peripheral nerve injuries (3 %) [4].
In the pathogenesis of this type of deformity, paralysis of the posterior tibial muscle groups with functional preservation of the anterior and lateral muscle groups is considered to be the main cause. As a result of the reduced or complete loss of function of the long flexors of the foot, an imbalance of forces between the flexors and extensors of the foot occurs and the extensors become heavily overweight. As a result, the foot reaches an extreme pronation position and the heel bone gradually shifts from a horizontal to a vertical position, increasing the inclination of the heel bone to over 30° (normal 25-28°) and sometimes even reaching 60-80°. The flexion of the foot may be so great that the back surface of the foot touches the forefoot, and the calf-foot angle, which is normally 70°, may be reduced to 20°. As a result of the pathological alignment of the calcaneus, the osteochondral relationship between the calf and talus is altered. The angle between the heel bone and the talus in the sagittal plane increases to more than 30° (usually 20-25°). If the talus is tilted medially or laterally, disruption of the frontal plane occurs. The anterior calf angle (normal 20-40°) increases or decreases, resulting in a calcaneo-valgus or calcaneo-varus deformity. The forefoot is lifted by the pull of the extensor muscles and positioned over the heel and midfoot. As a result, the angle between the talus and the first metatarsal bone (Meary's angle) increases to 25-30° (normal 0-5°). The degree of foot deformity largely depends on the severity of the neurological disorder, paralysis or paresis of the muscles of the lower limbs.
- The correct angle of waist and heel is.
- Equino valgus.
- Massage for flat feet.
- The bones of the human heel.
- flatfoot μb.
- bones in the heel.
- ICD 10 chalgus valgus.
- Short flexors of the toes.