The following treatments are recommended:

- ankle muscle
- Original[edit].
- Afferentation [edit | Edit code]
- Denervation[edit | Edit code]
- Features [Edit | Edit code]
- Plantar flexion of the foot in the ankle joint. Muscle function tests [edit edit source]
- Anatomy of Calf Muscle Pain
- Dangerous calf pain
- Free medical advice and diagnosis
- How to determine if there is an injury
- Raising the toes of one leg with knees bent
- discussion
- Lower limb enlargement with implants in Paris
- Recovery period after surgery
- Why and how to train the multifidus muscle
- The best calf exercises
- Fitted toe separator
- Tiptoe sit-ups on a Smith trainer
- Percussion press with bent knees
- A little anatomy
- Training the calf muscles
- Tiptoes while standing
- Standing donkey - tiptoe.
- Agonists, synergists and antagonists
- Definitions
- Examples of antagonistic muscles
- Upper limbs.
- Lower limbs.
- My videos about synergists, antagonists and agonists
- Specificity of antagonist function.
- symptoms
- Caused
ankle muscle
Original[edit].
- Posterior surface of the head and posterior proximal third of the fibula
- Tendon arch of the biceps muscle (extension of the tendon between the head of the fibula and the tibia)
Afferentation [edit | Edit code]
Denervation[edit | Edit code]
Features [Edit | Edit code]
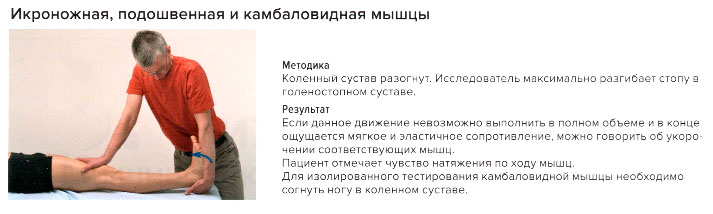
Lambda muscles (M. soleus) forms the triceps muscle together with the calf muscle and the soleus muscle. The cambialis muscle is an important flexor of the ankle joint and supinator of the supporting and ankle joint. However, it plays its most important role when standing by ensuring the balance of the ankle joint.
Plantar flexion of the foot at the ankle joint
Plantar flexion of the foot in the ankle joint. Muscle function tests [edit edit source]

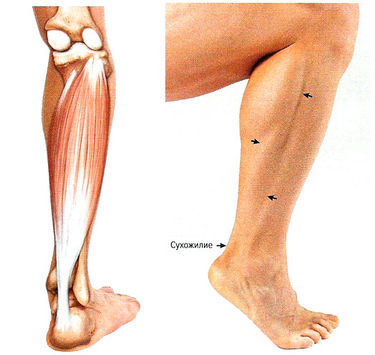
Anatomy of Calf Muscle Pain
A feeling of discomfort occurs on the back of the lower leg from the ankle to the knee. The calf muscle rises above the kidney muscle and is attached to the heel by the thick Achilles tendon. It consists of two muscle heads - a lateral and a medial. The calf muscle is made up of muscle fibers, tendons, ligaments, nerves and blood vessels. Each of these structures is vulnerable to injury, infection, and other disorders. Many of these diseases are accompanied by pain. The discomfort in the calf can be constant or temporary, the wave of pain can affect the entire calf muscle or be limited to a single area. The pain can be monotonous, throbbing or shooting, stabbing or increasing. The pain in the calf muscle can be described as a tingling, burning or numbness in the limb. Sensory disturbances are often referred to as paresthesias. The symptoms can be annoying and uncomfortable and sometimes lead to limited mobility, meaning those affected can no longer bend their leg or even walk.
Calf pain can occur for a variety of reasons. The cause can be an accidental trauma, a muscle spasm or a neurological disease. However, there are also serious diseases that indicate the development of peripheral arterial pathology. Calf pain can be caused by deep vein thrombosis (the formation of a blood clot). This is a life-threatening condition because the blood clot can break off and cause a pulmonary embolism or heart attack. Persistent pain in the calf muscle should not be tolerated. The patient should see a doctor immediately and receive a diagnosis and treatment.
Dangerous calf pain
- Varicose veins with a complication in the form of thrombophlebitis - failure to seek medical treatment in a timely manner can cost the patient his life. A dislodged clot clogs an artery and blocks blood flow.
- Diabetic angiopathy and neuropathy – is often a precursor to diabetes that the patient is not yet aware of. The pathology is detected by a blood sugar test.
- Atherosclerosis of the arteries of the lower extremities – creates favorable conditions for the development of a heart attack due to the occlusion or complete narrowing of the artery lumen by cholesterol deposits (atherosclerotic plaques).
- Obliterative arteritis is a serious vascular disease that often occurs in long-term smokers. A serious consequence of this disease is leg amputation.
Free medical advice and diagnosis
During the consultation, we carry out a thorough diagnosis of the entire spine and each of its segments. We determine exactly which segments and nerve roots are affected and cause the pain symptoms. Following the consultation, we make detailed treatment recommendations and prescribe additional diagnostics if necessary.
We carry out a functional diagnosis of the spine
Carrying out manipulations that significantly reduce pain
Development of an individual treatment program
How to determine if there is an injury
If the iliotibialis muscle is injured, you will feel a dull, aching pain during or immediately after exercise. The pain is often described as 'tolerable', but many people have to stop playing sports such as tennis, cycling or running as a result. As the disease progresses, the pain can become so severe that those affected may even have difficulty walking. There are three tests you can use to determine whether an injury to the jagellar muscle is the underlying cause of the pain.

Ask the patient to stand with bare feet on the floor, feet shoulder-width apart and parallel to each other. Then bend your knees as much as possible and place your heels firmly on the floor with your back straight. Ask him to get up on his toes a few times, keeping his knees bent and hopping his heels as high as possible. When the hamstring muscle is damaged, it causes discomfort or pain.
Raising the toes of one leg with knees bent
If the first test shows no signs of injury, try the following variation where you increase the load on the injured area. Ask the client to stand on one leg (the leg causing pain) while holding onto something for balance. Then ask the client to stand with their knee bent and their heel as high off the floor as possible. As previously mentioned, the cambialis muscle is very strong and this test alone may not detect pain, especially if the client is in pain after a five-kilometer run or a half-hour game of tennis. If no pain occurs during the test, repeat the test immediately after an activity that normally causes pain; performing this test should increase the pain or discomfort several times. If the test still shows nothing, the cause of the pain in this case is probably an injury to the calf muscle.

Ask the client to stand in a familiar position and carefully assess the position of the feet. Ideally they should be parallel or rotated outwards by a maximum of 5 degrees. When the feet are turned 10-20 degrees to the side, the arches of their feet can almost touch the ground. As the client bends the knees forward 5-6 cm, the knees look straight ahead with the feet turned outward.
To relieve pressure on the medial part of the leg and prevent damage, the client should develop the habit of standing correctly. Treatment of the extensor muscle is usually long-term: the greater the load, the longer the rehabilitation time.
discussion
The first and most important study of the anatomical structure of the intramuscular veins of the lower leg among Russian phlebologists was the work of Ukhov published in 1974 in the Archives of Anatomy, Histology and Embryology [21]. P. Dumpe, JI Ukhov and PG Schwalb [1] described the variants in the structure of these veins and distinguished three main vein collectors in the thickness of the tibial muscle (central, medial and lateral), which open through the fusion of small branches in the lower third of the tibia with numerous Side and upper branches were formed. The fundamental works of AN Vedensky, AI Gritsianov and YM Stoyko [23] clarified the anatomical structure of the intramuscular veins. They distinguished between trunk, network and intermediate variants of the intramuscular venous structure with the formation of hemodynamic arcs of open or closed type. The most common variant was reported by Savelyev et al. described [5].
In recent years, the intramuscular venous structure of the tibia has been studied by Stoyko YM et al. [6], Shevchenko YL et al. [8, 9, 24] and pointed out the well-known difficulties in studying these veins even with modern ultrasound and magnetic resonance imaging (MRI) techniques, in particular the inability to capture the volumetric architecture of these vessels.
Although computed tomography emerged and was used in clinical practice much earlier than MRI, the MSCT method experienced its second birth only with the advent of multidetector systems at the beginning of the 21st century. It is obvious that angiologists immediately looked at the possibility of imaging the venous system with MSCT (25).
The main focus was on the potential of MSCT in the complex diagnosis of VTE. According to AV Pokrovsky et al. [26], MSCT phlebography describes obstructive lesions of the inferior vena cava and pelvic veins with a high degree of accuracy. The advantages of the method are undeniable, e.g. B. in the diagnosis of the consequences of a shot in the limb with developed venous thrombosis or with arteriovenous fistulas that have arisen, in determining the causes and planning embolization of arteriovenous malformations, studying the aortic compression syndrome and the primary cause of pelvic venous varicose veins, determining the indications and evaluating the results of the Hybrid surgery for obstructive lesions of the iliac-femoral veins, performance of endovascular recanalization for chronic obstruction of the iliac-femoral veins in patients with thrombotic disease.
Lower limb enlargement with implants in Paris

Attractive lower leg implants made of silicone
The calf implants are inserted under general anesthesia and the patient spends one night in the hospital; the operation takes between 45 minutes and 1 hour 30 minutes.
The implants consist of a smooth shell filled with a very thick silicone gel. They are very stable and designed to withstand the stress in this area of the body. The implants are available in different shapes, oval or asymmetrical and teardrop-shaped, and their length is adjusted to the anatomy of each patient.
During the procedure, the patient lies on her stomach. The surgeon makes a 4-6 cm long horizontal incision hidden in the knee flexure crease. The scars are very thin and practically invisible over time.
The surgeon places the implant in the space under the muscle . He or she can one or two implants in each shin bone This depends on the patient's anatomy and the desired volume. He then applies self-absorbing sutures with a bandage to each leg.
Recovery period after surgery
The postoperative pain is mild and can be easily controlled with painkillers. They gradually subside during the first week. Mild discomfort persists in the following weeks.
The bruising will gradually disappear within a week, but the swelling in the calves and ankles may last one to three weeks.
The patient must wear compression stockings day and night for a month to ensure that the lower leg implant sits well in the correct place. In most cases, anticoagulants are prescribed to improve blood circulation and reduce the risk of phlebitis for two weeks after the procedure.
The patient can resume his daily activities resume one week after surgery, return to work after one to two weeks and do sports again after two to three months. Driving is not recommended for the first ten days.
Why and how to train the multifidus muscle
A well-developed muscle is a very important part of bodybuilding. Although the calf muscle lies beneath the calves, it also influences the external aesthetics of the bodybuilder's legs. So if an athlete wants to perform at their best on stage, they need to include exercises for the pectoralis muscles in their training program.
Over and beyond, Functions of the extensor muscles are: Flexion and extension of the legs, stabilizing the shins in an upright position and preventing the body from 'leaning forward'. This means that well-developed cheekbone muscles are needed in many sports: skiing, figure skating, gymnastics, games, sports dance, etc.
Now let's look at those Training principlesNow let's move on to the training principles to optimally train the muscles in question:
- The calf muscles work best when the shins are bent at a right angle and fixed in this position;
- Combine the calf muscles and pubic muscles in one workout to increase the load on the shins;
- Perform 4-6 sets of 20-25 reps. The last few repetitions should be accompanied by a burning sensation in the shins;
- Add plyometric loads (deadlifts) to your core exercises.
The best calf exercises
Concentrated exercises to help you get your calves into a 'slim' position.
Fitted toe separator
Use a special trainer to train your knees while sitting. Adjust the height of your knee socks before performing this exercise.
- Sit on the trainer and support the soft rollers with your knees;
- Place your toes on the foot platform 20-25 cm apart;
- Keep feet parallel to each other, heels in the air;
- As you exhale, lift your shins onto your toes;
- Pause for a second at the apex;
- With an inhalation, slowly lower your feet without placing your heels on the floor.

- Maintain a straight posture and avoid rounding your spine.
- Avoid sluggish weight throws; move fluidly.
- The negative phase (lowering) should be longer than the positive phase (raising).
- Massage your shins between each step to prevent blood congestion.
Tiptoe sit-ups on a Smith trainer
If your gym doesn't have such a shin trainer, perform this exercise on a Smith trainer or with free weights (such as a barbell on your knees).
Percussion press with bent knees
Use a leg press machine. Adjust the angle of the backrest to your body before the exercise.
- Sit on the machine and place the toes of your feet in the center of the platform;
- Keep your feet 20-25 cm apart and put the weight on your heels;
- Bend your knees at a right angle and lock your feet in this position;
- Exhale and push off the platform with your toes;
- At the top, tighten your lower leg muscles as hard as you can and hold them for a few seconds;
- Inhale and lower the wheelchair, but always keep pressure on your heels.
A little anatomy
First, let's get acquainted with the structure of the lower leg. The lion's share falls on the calf muscle, which consists of two heads - the medial and the lateral. It is their development that gives the lower leg the main volume. Below the calf muscle is the hamstring muscle - it is flat but wide, so its development can add width in both lateral and frontal views.
An important difference between the calf muscle and the camel muscle is that the calf muscle crosses the knee joint and attaches to the femur, while the calf muscle does not cross the knee joint and attaches within the shinbone. This means that the calf muscle is used most when standing, but is essentially inactive when the leg is bent at 90 degrees. In these moments, the calf muscle takes over the task.
This anatomical structure of the lower limbs leads to the peculiarity of training the calf and camel muscles - the calf muscles are trained while standing, and the camel muscles are trained while sitting, but more on that later.
In addition to the triceps tibialis anterior, there are also the forefoot extensors, the M. fibula longus and the M. tibialis anterior. To train them directly, you need a special trainer, which is so rare in gyms that you might forget about it. If your gym has such equipment, I recommend using it more often.
Training the calf muscles
We already know that the calf muscles are most active when you are standing and your legs are straight. The most important prerequisite for calf training is to have straight legs while standing.
Tiptoes while standing
The most popular and, so to speak, basic calf exercises are the following. Standing toe raises. For this exercise you can use either a special trainer or a Smith.
You may or may not use a sock rack, but I recommend using one. The height of the stand should be chosen so that your heels do not touch the ground at the lowest point. It is not necessary to deliberately go as deep as possible, a slight stretch at the bottom point is sufficient. The support helps to increase the range of motion, which is quite small in shin exercises.
The legs can be completely straight or slightly bent at the knee joint. The back should be kept straight, the pelvis should not be stretched backwards. Generally, the bar on the arms needs to be in line with the toes.
Standing lifts can also be done with dumbbells. In this variation, one hand should be kept on the bar for balance and the other hand should hold the dumbbells. Each shinbone must be stressed alternately.
Standing donkey - tiptoe.
An interesting and effective exercise is the donkey lift. For this exercise you need to lean your body forward and keep your legs straight. A major downside to this exercise is that it doesn't put enough weight on the calves, leaving you with no choice but to have a partner sit on your back and do the lifts together. But even with a partner, the burden may not be enough. An excellent replacement for this exercise is the calf press on a leg press machine. The advantages are obvious: no strain on the back and a very adaptable stroke. Such equipment is available in almost every gym.
Agonists, synergists and antagonists
Let's continue the discussion about the different classifications of skeletal muscles and talk about antagonists, synergists and agonists. I adopted these definitions from the excellent book Antagonist Muscles in Human Movement by Raisa Samuilovna Persson.
Definitions
muscle antagonists are two muscles (or two muscle groups) of the same joint that pull in opposite directions when contracted.
Synergistic muscles are muscles of a joint that pull in the same direction.
Of the two antagonistic muscles, the one that performs a specific movement (that is, performs the main task) is called agonistand the other will be as antagonist..
Examples of antagonistic muscles
Upper limbs.
1. The flexion of the forearm is done by the Biceps brachii (m.biceps brachii), and the extension of the forearm is done by the M. triceps brachii (M. triceps brachii) (M. triceps brachii). These two muscles are antagonistic in that they pull in opposite directions relative to the elbow joint. One muscle (M. triceps brachii) is responsible for flexion and the other (M. triceps brachii) for extension.
2 The muscles responsible for flexing the shoulder (humerus): Deltoid (anterior bundle), pectoralis major, beak, biceps brachii. Extension of the shoulder (humerus) is carried out by antagonistic muscles: Posterior deltoid, posterior broad muscle, subscapularis muscle, small obturator muscle, large obturator muscle, long head of the triceps brachii..
3: Abduction of the humerus is carried out by. Deltoid and supraspinatus muscles. The adduction of the upper arm is carried out by the muscles: Subiliacus, small circular muscle, scapular muscle, long head of the triceps brachii and M. pleucolepianus brachii.
Lower limbs.
3 The flexion of the lower limbs is realized, among other things, by Biceps femoris muscle (M. biceps femoris), and the extension of the lower limbs is carried out by the quadriceps (M. quadriceps femoris). The quadriceps femoris (m. quadriceps femoris) (m. quadriceps femoris). These two muscles are antagonistic, meaning they exert an opposite pull on the knee joint. One muscle (biceps femoris) is responsible for flexion and the other (quadriceps femoris) is responsible for extension.
My videos about synergists, antagonists and agonists
Specificity of antagonist function.
1. The presence of antagonists is necessary because a muscle can only pull a bone, not push it. For example, in order for a bone limb to be able to flex and extend, two muscles must be present. One muscle is responsible for flexing the joint and the other for extension.
(2) Antagonist muscles do not need to work alternately when performing a motor action. Already at the beginning of the 20th century, the German scientist R. Wagner (1925) showed that depending on the conditions of the external force field, the ratio of the phases of activity of the antagonistic muscles changes. The complete correspondence of muscle activity with movement is observed only in movements against frictional forces. When working against inertial forces, the agonist muscle is only active in the first phase of the movement. Thereafter, movement continues by inertial forces with increasing activity of the antagonist, which slows the movement (Fig. 1).
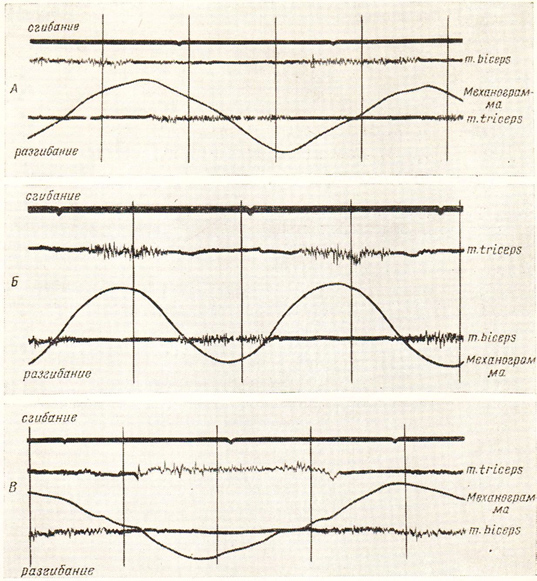
3 The activity of the antagonist is strongly dependent on the speed of the movement. When the movement is performed more slowly, the activity of the antagonist muscles corresponds to the phases of the movement for which they are responsible. During flexion, the flexor muscles are active, while during extension, the extensor muscles are active. By increasing the speed of movement, the extensor muscle can become active at the end of the flexion phase. In this case, the extensor muscle (antagonist) acts as a brake. During fast movements there are also phases with simultaneous activity of the antagonists (AV Samsonova, 1998).
symptoms
Pain from trigger points in the cambialis muscle occurs primarily in the heel, calf, and back of the ankle (Fig. 10.28 and 1 0.29). Ironically, trigger points in this muscle can respond with deep sacral pain and cause spasms in the muscles of the lower back.
There are cases when the pain is reflected in the jaw. In some cases, a trigger point in the inner part of the muscle at the posterior edge of the tibia causes pain in the inner bony prominence of the ankle joint (Fig. 10.31). Some real medical problems are characterized by symptoms similar to those caused by trigger points in the cambialis muscle, leading to misleading diagnoses. Examples include thrombosis, phlebitis, fractures and ligament or tendon tears. Myofascial pain is sometimes confused with a split shinbone or a symptom of a heel spur. The latter may actually be present but not cause pain. If you have pain in the back of your ankle, the typical diagnosis is Achilles tendonitis.
Heel pain is usually referred to as plantar fasciitis. Traditional treatment for both conditions in the form of painkillers, steroid injections, physical therapy and rest is often unsuccessful. This is understandable considering that none of these methods affect trigger points. Pain in the heel and in the Achilles tendon area usually originates from trigger points in the gastrocnemius muscle, the posterior tibialis or the quadriceps muscle of the thigh.
Trigger points in the calf muscle can be an indirect cause of calf cramps if they affect blood circulation in the muscle. This muscle is sometimes called the second heart because it helps pump blood up from the legs. As long as these muscles are active, healthy and flexible, they pump blood very efficiently by contracting during shortening and lengthening, but trigger points reduce their efficiency. Drops in blood pressure and fainting are in some cases due to weakness or dysfunction of the cambium muscles.
Caused
A strain of the cheekbone muscles occurs from slipping, running, or walking on sand or gravel. They are stressed by an unsteady gait caused by stiff leather soles. Problems can also arise from inflexible soles, pressure from behind on the feet when sitting on a chair with a footrest, and skating and skiing without good ankle support. A very common cause of yoke muscle fatigue is aerobic dancing. High heels keep muscles shortened, and that's a sure way to trigger points and stabilization. Ankle instability, a common consequence of walking in high heels, also puts strain on the flounder muscle with every step.
Fix the position of the camel toe muscle, which contracts under the lower edge of the calf when the toe is extended. Use the same massage techniques as for the calf muscles. The knee of the other leg is particularly helpful. Be sure to cover the entire width of the back shin in several parallel vertical movements.
If you feel dizzy after getting up from a sitting position, try shifting your body weight from one leg to the other for a few seconds once you are on your feet, at the pace at which you normally walk. This promotes the pumping function of the cambium muscle and faster oxygen supply to the brain.
The same technique helps to restore breathing and strength after sports or physical exercise: after any physical exercise, the alternating contraction of the calf muscles accelerates the flow of blood from the legs to the entire system, at the exact moment that Tissue needs this accelerated blood flow. It is known that soldiers can lose consciousness if the calf muscles are inactive for a long time while on duty. Once trained, they know how to prevent fainting by rhythmically tensing and relaxing their calves.
The calf muscles need to be trained to maintain their pumping function and be able to move the body forward. At the same time, they must not be overused by putting unnecessary strain on them. A sudden increase in normal activity levels in the form of a new exercise program, weekend-only exercise, or unfamiliar gardening can affect both the calf muscles and other calf muscles. Prevention is particularly important for the calf muscles. It is very useful to learn the following
Read more:- The flexor muscles of the foot.
- lower leg flexion.
- Lift your heels off the floor during the squat.
- Exercises for the triceps tibialis muscle.
- Triceps femoris muscle.
- lower leg muscles.
- lower leg stretches.
- The muscles that move the foot.