At this point, early rehabilitation begins under the guidance of qualified doctors. This includes mobility and the beginning of normal digestion. On the 2nd and 3rd day, the patient returns to full life without a colostomy bag and recovers naturally.

- Closure of a permanent colostomy (minimally invasive surgery)
- How does intestinal obstruction surgery work?
- Go
- wound healing
- Training and adjustment to the new body
- Skin care: how to make the process of putting on a colostomy bag easier
- Pavement
- cleaning the skin
- emergency cleaning
- How the procedure is carried out
- preparation phase
- How is the operation performed?
- Contraindications and possible complications of colostomy closure
- Postoperative Recovery
- Working hip prosthesis with elastic insert PN6-50
- Non-modular tibial prosthesis with leather splint PN3-12
- How long does it take to heal and when is it advisable to remove the stitches?
- TRAUMATIC INJURIES OF THE HAND SEGMENTS
- POST-TRAUMATIC CONTRACTURES
Closure of a permanent colostomy (minimally invasive surgery)
The modern surgical techniques available to patients at the IIBS Surgical Center make it possible to close a permanent colostomy and restore the continuity of the colon, eliminating forever the colostomy bag and the inconveniences of this type of defecation.
A colostomy is an exposed section of the large intestine at the front wall that is used to evacuate fecal matter, which is collected in a special colostomy bag that is usually taped to the skin near the colostomy opening.
A large percentage of patients with a permanent colostomy had surgery ten or more years ago. At that time, technologies for safely reconnecting portions of the colon after removal of a fragment due to trauma, an acute condition, or a neoplasm (colon cancer or benign choriocarcinoma) were not well developed, and colostomy was the only option for an acceptable quality of life. Therefore, a permanent colostomy was also performed in cases where the anal sphincter was not damaged by tumor infiltration (the only clear indication for a permanent colostomy).
Today, however, thanks to the development of technologically advanced surgical techniques, there is a unique opportunity to rehabilitate colostomy patients through minimally invasive procedures to repair (reconstruct) the colon and Colostomy Closure.

Surgeons at MIBS Clinic perform laparoscopic surgeries
The successful restoration of the natural excretory function of the intestine is based on the development of three main areas of modern surgery:
- Safe fusion of intestinal parts. – Secure bowel connection using modern suturing devices;
- 'Gentle access to the abdominal cavity'. No abdominal surgery - transanal endoscopic and laparoscopic surgery;
- rapid rehabilitation Patients – quick operation
How does intestinal obstruction surgery work?
The restoration of the continuity of the colon and the closure of the abdominal wall defect are performed in a single operation; no repeat operations or surgical manipulations are required.
- Isolation of the functioning part of the intestine from the mouth of the stoma and insertion of the upper part of the anastomosis device (intestinal connection);
- Isolation of the lower part of the intestine (leading to the sphincter) to achieve the required length;
- inserting the lower portion of the suturing device into the rectum;
- Connection of the two parts of the device, followed by a one-step connection of the two parts of the intestine with the help of titanium staples that do not affect the body and do not need to be removed;
- checking the integrity of the anastomosis (the point where the two parts of the intestine are 'stitched' together);
- Closing the stoma opening with a mesh prosthesis to protect against hernias;
- cosmetic repairs of cosmetic defects to minimize scarring at the stoma site and laparoscopic approaches.
All procedures are performed without incisions and under visual control with a video endoscope inserted into the abdomen and pelvis through small punctures in the abdominal wall.
Go
The patient leaves the hospital on crutches. The crutches are used for 2 weeks. In the first three days after the operation you should not lean on the operated leg, but lie down as far as possible and hold the operated leg over your body (e.g. on three pillows stacked on top of each other) and only walk, if absolutely necessary. Walk as little as possible for 2 weeks after the operation and raise the operated leg when sitting (put it on a chair). After the operation, you are usually allowed to walk in special shoes that shift the load from the operated area to the heel.

Depending on the operation, the special shoes are only worn for 6-8 weeks for walking and are removed at rest and before going to bed.  Shoes are removed before going to bed. Driving on public transport and driving a car is possible after 6-8 weeks, depending on the operation. Cycling and swimming can be tried out after the time with the special footwear. Walking with sticks, jogging, jumping and cross-country skiing are possible around 16-24 weeks after the operation. When doing sports, you can put weight on your foot until it hurts. Normal shoes can be worn for 6-8 weeks after the operation. Until the swelling of the foot and the pain in the surgical site have subsided, it is advisable to wear soft shoes that are slightly larger than your normal size. Only 3-4 months after the operation you can wear the shoes you like.
Shoes are removed before going to bed. Driving on public transport and driving a car is possible after 6-8 weeks, depending on the operation. Cycling and swimming can be tried out after the time with the special footwear. Walking with sticks, jogging, jumping and cross-country skiing are possible around 16-24 weeks after the operation. When doing sports, you can put weight on your foot until it hurts. Normal shoes can be worn for 6-8 weeks after the operation. Until the swelling of the foot and the pain in the surgical site have subsided, it is advisable to wear soft shoes that are slightly larger than your normal size. Only 3-4 months after the operation you can wear the shoes you like.
wound healing

Some bleeding after surgery is normal. A bandage with a small amount of blood does not need to be changed because the blood is sterile and does not interfere with the healing process. It is not advisable to remove the bandage for up to 48 hours after the operation as this will cause the wound to become inflamed. Bandage the small amount of blood yourself with non-sterile gauze or a bandage. If the bandage is very bloody or just badly soiled, ask a competent healthcare professional to change it as soon as possible. If the wounds are to heal, bandage the leg once every seven days. The sutures are removed 17-21 days after the operation. If the wound heals normally, the surgical scars on the fingers are barely visible. Contractubex gel can be used for three months after the stitches have been removed to avoid excessive scarring. If you have problems with wound healing, consult your doctor before washing your foot. Signs that the wound is fully healed: the edges of the wound have healed, there is no discharge from the wound, and the scabs have come off.
After surgery, it is important to keep the toe in the correct position to allow the soft tissues surrounding the bone to heal properly and the toe to maintain its normal shape.

After the operation, the big toe must be held in the correct position 24 hours a day with an interdigital spreader or bandage. When the big toe is immobilized, there is no need to maintain its position.

Training and adjustment to the new body
Ostomy clinics have an ostomy care consultation that you can go to if you have any questions. You will usually have many of these questions immediately after your operation. On average, it takes six months or more to master ostomy care (and multiple treatments per day for loose stools). You can and should also contact him if care becomes difficult, if the stoma is leaking, if you notice skin irritation, discoloration or bulging of the stoma or other complaints.
However, the adaptation process is not limited to physiology. In many societies, the process of defecation is a taboo subject, and in the case of an intestinal stoma, it takes place in a completely different way than everyone is used to. This can create both disgust at one's ostomy and a constant sense of shame for fear that others will perceive someone with a colostomy bag as 'unclean', particularly when visiting gyms, swimming pools and public places. Another negative aspect of self-perception is the perception of a changed body that has lost some of its functions. What helps to deal with it?
- Controlling the stoma to get used to it. In addition, it is important to examine the stoma regularly to notice changes over time.
- Remind yourself that your stoma helps relieve distressing symptoms of illness, restore health, or avoid death.
- Talk to other people who have a stoma. This will help you learn both the ins and outs of caregiving as well as effective ways to manage stress.
- Give yourself time to adjust and become aware of how an ostomy looks, works and affects your body.
- Talk to a medical psychologist or psychotherapist.

When my ostomy was done I spent a lot of time dealing with the physical discomfort, the hole in my abdomen and the constant thoughts of the colostomy bag. The thought that it was time to change the bag completely spoiled my mood. I was afraid it would leak, smell, or stain, and I was consumed with thoughts like, 'why did this happen to me? ....' haunted. I wanted to lock myself in the house and had to go to work.
Skin care: how to make the process of putting on a colostomy bag easier
Even if there is no scarring where the pouch is attached, the skin may be uneven. It can also become irritated by contact with the adhesive layer of the patch, which means it needs to be protected. What helps?
- A barrier cream around the stoma to improve adhesion of the patch to the skin.
- A sealing paste that comes in the form of a stick or putty. A good trick is to combine the two, using the putty to flatten the skin and the stick to seal it afterwards. For ileostomies, when the time to change the bag is very short, the first layer of sealant can be dried with a hair dryer (and the colostomy bag too, making it easier to adjust the stoma).
- Special powder.
- 'Air out' once every 5-7 days to allow the skin around the stoma to recover.
Don't immediately focus on a single brand of sealant, cream, or band-aid. First, what works for a colostomy will not work for an ileostomy due to the more aggressive bowel contents. Second, the vulnerability of the skin, its topography, is different. And if something goes wrong, you have to keep experimenting with different preparations, preferably in consultation with the medical staff in the clinic.
Pavement
Ostomy plasters can and should be chosen even if the skin is sensitive. Silk plasters, paper plasters, textile plasters, surgical plasters and one-piece and two-piece plasters are available. Tip: If you are unable to get a band-aid to stick firmly to the skin in an uneven area, you can add more strips.
cleaning the skin
It is advisable to clean the leather with a special cleaning agent when changing the bag - this removes glue, cream or sealing compound residue from the leather. As a rule, water and soap alone are not enough. Remember that ordinary lotions, creams, skin oils, etc. leave a film that prevents devices from sticking. When applying body cosmetics, avoid the stoma area.
emergency cleaning
Kits with special sponges and absorbent materials are helpful when water is not available at the site where the emergency bag is to be replaced or when the container is leaking.
How the procedure is carried out
After disinfecting the skin, a longitudinal incision is made along the neurovascular bundle. The great saphenous vein and saphenofemoral junction are removed from the surgical wound. The great saphenous vein and its tributaries are ligated as far as possible from the femoral vein.
The postoperative phase lasts 2 to 3 days. After 24 hours you can slowly walk independently again. The skin sutures are removed 7 days after the procedure. The skin sutures are removed after a week.
In the rehabilitation period, conservative treatment is carried out: anti-inflammatory drugs, phlebotherapy, therapeutic physical exercises. It is advisable that the patient should not sit or stand for 4-6 weeks after the operation. When lying down, it is advisable to place a soft pillow under your legs. The rehabilitation phase lasts between one and two months (may vary depending on the healing progress).
The surgeons of the St. Petersburg Longevity Clinic have extensive clinical experience and are constantly educating themselves at various advanced training seminars, symposia and conferences.
The success of an operation largely depends on the surgeon's clinical practice, and our clinic's surgeons are among the best in the city in this field. If you entrust your health to us, you will be examined without waiting and you will receive all the medical care you need.
On our website you can register for a consultation with a phlebologist 24 hours a day.
preparation phase
To prepare for leg vein surgery, you must undergo a medical examination. This allows you to identify existing problems and possible contraindications.
The following laboratory tests are ordered before the crossectomy:
Even before the operation, the doctor must know exactly where the thrombosis is located, how much of the vessel is affected by varicose veins and whether there is an inflammatory process.

The patient must be psychologically prepared. It is important that you understand what the surgery is, what it is for, and that you discuss any questions you do not understand with your doctor. Tell your doctor in advance about all medications you are taking. Some of them should be stopped before the operation.
A word of warning!
Blood-thinning medications, such as warfarin and aspirin, usually need to be stopped some time before surgery. This will help avoid possible complications.
The preparation for the operation also includes the following measures:
- showering or bathing the morning of the day of the crossectomy;
- Refraining from shaving the legs at the surgical sites for several days to avoid infection and inflammation;
- Refrain from eating and drinking for 6-8 hours if the operation is performed under general anesthesia.
Adequate preparation is very important. This avoids many complications during the operation.
How is the operation performed?
- The skin at the incision site is treated with antiseptics;
- The operation area is covered with a special sterile pad;
- The doctor palpates the femoral artery and locates the great saphenous vein;
- A small incision, up to 4 cm long, is made over the vein;
- By moving the subcutaneous tissue, the doctor approaches the vein;
- The vein is exposed up to its confluence with the femoral vein;
- At the point where the great saphenous vein joins the femoral vein, the vessel is ligated and excised;
- All arteries are isolated, ligated, and excised;
- The incision is closed and a sterile dressing is applied.
Interesting!!!
The doctor decides on the type of anesthesia depending on the patient's condition, age and existing contraindications. Local, regional or general anesthesia is used.

Contraindications and possible complications of colostomy closure

Only in forty percent of cases is it possible to restore bowel function to its former state. After a colostomy is closed, some complications are possible that affect the colostomy area and bowel function after prolonged inactivity. The most serious complications occur after closure of a bundle-ended colostomy, as this type of colostomy is considered permanent and designed for life.
The following complications occur with the closure of any type of colostomy
- prolapse of the rectum from the anus;
- Perforation or rupture of the bowel at the surgical site;
- Intestinal obstruction in the surgical field due to accumulation of large amounts of faeces;
- infectious inflammatory or purulent processes in the area where the colostomy was previously located.
There are a number of contraindications for colostomy:
- atrophy or damage to the sphincter;
- Removal of more than thirty percent of the bowel at the stoma site, in addition to the rectal exit;
- Long-term treatment with chemotherapy for cancer;
- Atrophy, or more than 50 percent damage to the villous epithelium, as stool obstruction can occur, often leading to sepsis.
Postoperative Recovery
The rehabilitation phase after a colostomy closure operation usually lasts several months. If the patient does not follow the doctor's instructions at this stage, or only insufficiently, all sorts of complications can arise.
When the recovery and rehabilitation period ends is decided solely by the patient's doctor, based on the diagnostic examinations of the intestine.
The most important thing in the postoperative period is to follow a diet and a healthy lifestyle with a strict daily rhythm.

The diet program during recovery looks something like this:
- 3 to 5 days after the operation only intravenous fluid supply with the necessary medications;
- From the fifth to the twelfth day it is allowed to eat only liquid porridge with added sugar;
- From the twelfth to the twenty-first day, other foods may be gradually introduced, with the exception of raw fruits and vegetables;
- apple peels, corn, raw cabbage, legumes, fried and spicy foods can be eaten only three months after the operation.
Working hip prosthesis with elastic insert PN6-50
For middle-aged or elderly users with upper, middle, or lower hip stump. Suitable for weight-bearing and physically demanding work.
Modular composite hip prosthesis made up of modular units from different manufacturers with laminated bushings, designed for the prosthesis of disabled people of all ages (except children) after unilateral or bilateral amputation of the upper, middle or middle and lower third of the thigh.
Non-modular tibial prosthesis with leather splint PN3-12
Suitable for users with a clubfoot residual limb and residual limbs of different shapes and lengths whose volume changes throughout the day.
Suitable for users with a clubfoot Pirogow with a shortening of at least 6 cm.
The company is licensed (License No. 99-08-000004 dated 03/19/07, License No. 99-01-004831 dated 06/13/07).
How long does it take to heal and when is it advisable to remove the stitches?
Medical sutures should not be removed until the wound area has completely healed, which is diagnosed when the edges of the wound are firmly attached. The healing time is affected by the following factors:
- the individual body characteristics;
- Age and general health of the patient (presence of chronic diseases, concomitant pathologies)
- the correctness and accuracy of the surgeon's actions during the manipulation;
- compliance with the doctor's recommendations during the recovery period.
TRAUMATIC INJURIES OF THE HAND SEGMENTS
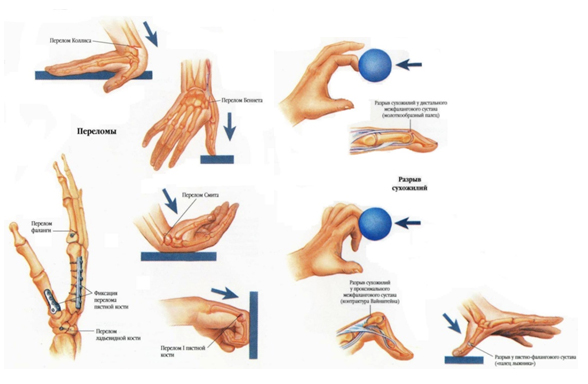
Traumatic injuries of various segments of the hand occur as a result of severe mechanical trauma with primary tissue destruction, as well as after deep burns, frostbite and ischemia.
I. Causes:
mechanical injuries;
thermal injuries;
other.
II. Number of beams: single; multiple; in total.
III. degree: compensated; subcompensated; decompensated 1st, 2nd, 3rd degree.
The number of rays determines the number of defects on the hand segments. It can be an isolated defect of one ray, more common on ray I in the form of defects of the phalanges and metacarpal bones at different levels. A multiple beam defect is the total or partial loss of two or three to four beams. A total defect is an amputation of the hand at the level of the carpal bones, in which the hand as an organ loses its form and function.
Depending on the severity of the damage to the hand, three degrees of severity can be distinguished, which enable an indication and a suitable method for reconstruction of the residual limb.
Defects in the distal phalanges are compensated and do not require reconstruction.
Decompensated defects are defects at the level of the main phalanges of the fingers, and the indications for reconstruction are determined individually to improve gripping function.
Decompensated defects in the fingers are divided into three degrees of severity. In the first stage, the defect runs along the metacarpal line. Such a stump has a significant functional limitation and is suitable for reconstruction. In the second degree of severity, the decompensation is in the area of the metacarpal line. This hand has no gripping function and should be reconstructed. The third stage of decompensation is along the metacarpal and represents a loss of the hand. It is currently not possible to reconstruct such a stump. She has to be treated with a prosthesis.
POST-TRAUMATIC CONTRACTURES
A contracture is a limitation in the range of motion of a joint as a result of pathological changes in the surrounding tissues that are functionally related to the joint.
I. By cause:
1. traumatic.
2. immobilized as a result of prolonged immobilization by plaster casts.
3. Ischemic, resulting from circulatory disorders due to trauma or tissue compression.
4. other.
Contractures of the hand are classified according to the anatomical structure of the joints: contractures of the wrist, metatarsophalangeal joint, metatarsophalangeal joint, interphalangeal joint and are characterized by clinical features.
According to the frequency of occurrence, a distinction is made between isolated contractures of one joint and multiple contractures of several joints in the hand.
With regard to the functional impairment, a distinction is made between flexion contractures with different extension deficits of the hand and fingers. Flexion contractures with severe deficits in extension of the hand and fingers are the most severe contractures with scarring of the palmar and dorsal surfaces and concomitant fibrosis of the joints, tendons and muscles. As a rule, they are often associated with an impairment of the gripping function of the hand! Abduction contractures in the extended position of the fingertips and adduction contractures and deficits in finger abduction, limited interfinger and surface grip. Scarring of the tissues of the wrist is a cause of wrist dysfunction.
Various types of hand and finger trauma: closed intra-articular fractures, joint dislocations with hemarthrosis and subsequent plastic arthrosis; open, also gunshot wounds to the hand, ranging from head wounds to injuries to the bone and joint apparatus, the muscles and the tendons and nerves. Post-traumatic contractures include the most common consequences of deep, thermal and chemical burns, electrical trauma and frostbite, which are accompanied by extensive scarring of the skin and subcutaneous tissues of varying depths.
Read more:- stump care.
- Cult at Shopar.
- Colostomy - what is it?.
- blunt.
- Are human legs the same?.
- The lateral side is.
- Sore muscles in the calf.
- incision on the leg.